
Recommended
More Related Content
Similar to Bladder Cancer risk factors pathophysiology and treatment
Similar to Bladder Cancer risk factors pathophysiology and treatment (20)
Recently uploaded
Recently uploaded (20)
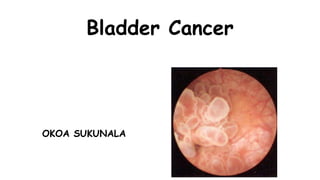
Bladder Cancer risk factors pathophysiology and treatment
- 2. …so that's the problem…
- 3. Bladder cancer: Epidemiology • Incidence: 20/100000/year (Europe) • Mortality: 8-9/100000/year • Fourth most common cancer in men • Incidence: 31.1 mortality: 12.1 • Thirteenth most common cancer in women • Incidence: 9.5 mortality: 4.5 • At diagnosis >70%: > 65 y of age
- 4. Bladder cancer: Epidemiology • In Tanzania the study done by Mahenda D.E at Muhimbili and Tumaini hospital in 2012 identified women are more affected than men, and the male to female ratio was 1:1.7. • Globally men are more commonly affected than females with a male/female ratio of 10:3
- 5. Bladder cancer: Aetiology • Smoking – 4x increased risk • Causes 50% of cases • Occupational – rubber/dye industry • Napthylamine, benzidine • Schistosomiasis, chronic infection • Medications – cyclofosfamide, fenacetin
- 6. Bladder cancer: Histology • 90-95% transitional-cell carcinoma • 3% squamos-cell carcinoma • 2% adenocarcinoma • <1% small-cell carcinoma • 99% primary tumors
- 7. Situation in our setting Study at MNH and Tumaini hospital documented four histological types in all patients of bladder cancer, • squamous cell carcinoma 47 (70.1%) • transitional cell carcinoma 16(23.9%) • Adenocarcinoma 3 and Adenosquamous 1. • Histological grades; were either well or moderately differentiated.
- 8. Bladder cancer: Presentation • Classically painless frank haematuria, sometimes intermittent • Frequent urination, urgency • symptoms with involvement of neighboring organs /kidneys, lymphoedema, pelvic pain
- 9. Bladder cancer: Examination • History • Physical examination • Urine examination / urinalysis, cultivation, cytology – can be only 60% sensitive • Ultrasound
- 10. Bladder cancer: Examination • Cystoscopy is mandatory • Biopsy or TURBT • Bimanual pelvic examination /before and after TURBT/ • Chest X-ray • IVU – not routinely, (5% chance upper tract involvement)
- 11. Bladder cancer: Stage and Prognosis • Ta – confined to the epithelium, no invasion through basement membrane • Tis – carcinoma in situ – aggressive (grade 3) cells confined to epithelium – 50% progression risk • T1 – invades lamina propria • T2 – invades bladder muscle • T3 – outside bladder • T4 – adjacent organs involved
- 12. Bladder cancer: Stage and Prognosis
- 13. Bladder cancer: Stage and Prognosis Stage TNM 5-y. Survival 0 Ta/Tis NoMo >85% I T1 NoMo 65-75% II T2a-b NoMo 57% III T3a-4a NoMo 31% IV T4b NoMo 24% any T N+Mo 14% any T M+ med. 6-9 Mo
- 14. Bladder cancer: Grade (WHO 1973) • Grade 1 – well differentiated – good prognosis • Grade 2 – moderately differentiated • Grade 3 – poorly differentiated • Least common • Most progress to invasive disease
- 15. Bladder cancer: Grade (WHO/ 1998) • PNLMP - papilar neoplasia low malignant potential • LG - papillary carcinoma of low-grade malignancy • HG - papillary carcinoma of high-grade malignancy
- 16. Carcinoma in situ (CIS) • Precursor infiltrating tumors • Primary or secondary • Subjectively – frequent urination, urgency, cystalgia • Objectively – no pathologies • Laboratory • Microhematuria • Cytology positive
- 17. CIS diagnosis • Cystoscopy • Pink areas • Random biopsy • Fluorescent cystoscopy
- 18. CIS treatment • Primary CIS: BCG • Secondary CIS: TURB + BCG • Recurrent CIS /after therapy/: cystectomy
- 19. Bladder cancer: Treatment • Superficial Bladder Cancer pTa, pT1, Tis • Invasive bladder cancer pT2-pT4
- 20. Superficial Bladder Cancer pTa, pT1, Tis • Standard of care=intravesical therapy transurethral resection bladder tumors /TURBT/ • Relapse rate: 70% adjuvant therapy
- 21. TURBT
- 22. TURBT
- 23. TURBT
- 24. TURBT – bladder perforation
- 25. Superficial Bladder Cancer • Histological grading is important G1 G2 G3 Relapse rate 42% 50% 80% Progression rate 2% 11% 45%
- 26. Superficial Bladder Cancer Adjuvant Therapy • Reduces relapse rate by 30-80% • Mitomycin C – in patient with intermediate-risk Bladder tumor • BCG – in patient with CIS, high risk Bladder tumor
- 27. Invasive bladder cancer • Standard of care = Radical cystectomy with pelvic lymphadenectomy Only about 50% of patients with high-grade invasive disease are cured
- 30. Chemotherapy for bladder cancer • Bladder cancer is a chemosensitive disease • Active single agents. • Cisplatin 30% • Carboplatin 20% • Gemcitabine 20-30% • Ifosfamide 20%
- 31. Chemotherapy for bladder cancer Combination chemotherapy. RR CR • MVAC 40-75% <20% • Gemzar / Cisplatin 40-70% 5-15% • Gemzar / Carboplatin 65% 5% • Taxol / Carboplatin 20-40% • CR-Clinical reponse • RR-reduced relapse rate • MVAC-Methotrexate, vinblastine, doxorubicin (Adriamycin), and cisplatin
- 32. Neoadjuvant chemotherapy • Meta-analysis of ten randomised trials (2688 patients) 13% reduction in risk of death 5% absolute benefit at 5 years Overall Survival(O.S) increased from 45% to 50% ABC Meta-analysis Collaboration. Lancet 2003;361:1927
- 33. Combined Radio- and Chemotherapy CR 5y.OS • Radiotherapy 57% 47% • RT and cisplatin 85% 69% • RT and carboplatin 70% 57% Birkenhake et al. Strahlenther Onkol 1998;174:121
- 34. Bladder-sparing protocol Transurthral resection Induction Therapy: Radiation + chemotherapy (cisplatin, paclitacel) Cystoscopy after 1 month no tumor tumor Consolidation: RT + CT cystectomy
- 35. Combined-modality treatment and organ preservation in invasive bladder cancer • Rödel et al. JCO 2002;20:3061 • Complete remission 72% • Local control after CR 64% (10 y.) • distant metastasis 35% (10 y.) • Disease-specific survival 42% (10 y.) • Preservation of bladder >80%
- 36. Situation in our setting In a study done by Mahenda D.E at MNH and Tumaini hospital patients presented with clinical stage 4 diseases (46.3%). Among all 67 patients 13 (26.5%) had cystectomy and 3 (6.1%) had TURBT. The rest had palliation either in the form of chemoradiotherapy or home palliative care (16(12.2%) and 27 (55.1%) respectively. Anaemia was the leading complication (30.5%). 49.3% died before any treatment . 15.2% died of renal failure and 54.5% died of advanced bladder cancer
- 37. ….so, the bladder has been removed….then?? and urine, how to get it out…?
- 38. Urinary diversion • Diversion of urinary pathway from its natural path • Types: • Temporary • Permanent
- 39. A nephrostomy is a surgical procedure by which a tube, stent, or catheter is inserted through the skin into the kidney
- 40. Cutaneous Ureterostomy… •One kidney drainage, with short-live prognosis •Complications (infection, stone, stenosis)
- 41. Permanent urinary diversion • Uretero – sigmoidostomy • Ileal conduit • Colon conduit • Ileocaecaecal segment
- 42. Cutaneous urinary diversions Ileal conduit (ileal loop) A 12 cm loop of ileum led out through abdominal wall Stents used The space at cystectomy site drained by a drainage system After surgery a skin barrier and a transparent disposable urinary drainage bag Constantly drains
- 44. Complications of ileal conduit • Wound infection • Wound dehiscence • Urinary leakage • Ureteral obstruction • Small bowel obstruction • Ileus • Stomal gangrene • Narrowing of the stoma • Pyelonephritis • Renal calculi
- 45. Continent Urinary Diversions • Continent Ileal Urinary Reservoir Indiana Pouch • Most common continent urinary diversion • Periodically catheterized Koch Pouch Ureterosigmoidostomy • Voiding occurs from rectum
- 47. Uretero- sigmoidostomy • Complications: • Reflux of urine • Hyperchloraemic acidosis (ammonium chloride reabsorption, bicarbonates secretion) • Renal infection • Stricture formation
- 49. Potential complications • Peritonitis due to disruption of anastomosis • Stoma ischaemia and necrosis due to compromised blood supply to stoma • Stoma retraction and separation of mucocutaneous border due to tension or trauma
- 53. references • Slideshare.com Tomáš Novotný urinary bladder cancer • Mahenda E.M profile and early treatment outcome of patients with carcinoma of the urinary bladder as seen in two hospitals (Muhimbili National hospital and Tumaini) in Dar es Salaam from March 2012 to December 2012.