Liver Transplantation: Current Status and Patient Selection in BC
•
2 likes•1,164 views

British Columbia Medical Journal, May 2010 issue Please download or visit this entire issue online at http://bcmj.org/may-2010
![Liver transplantation: Current status in British Columbia
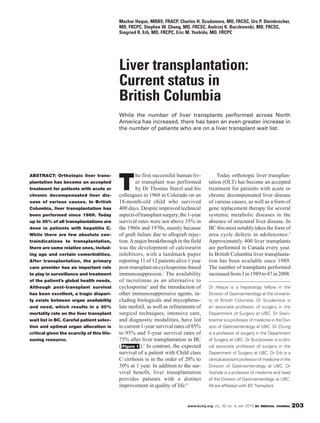
Patient selection
100% Careful patient selection and proper
organ allocation are critical given the
90% scarcity of this life-saving resource.
The transplant team has an ethical
80%
obligation to act in the best interests
Survival rate
of both the individual patient referred
70%
for assessment and the entire group
of patients who are in need of trans-
60%
plantation. 6 A successful outcome
Patient survival depends on optimal patient selection
50%
Graft survival and timing.
40%
0 1 2 3 4 5 6 7 8 9 10 General considerations
Years post-transplant A patient should be considered for
liver transplantation if this option
extends life expectancy and improves
Figure 1. Patient and graft survival for first liver transplants in BC, 1995–2004. quality of life beyond the expectation
Source: BC Transplant of the natural history of the underly-
ing liver disease. Current candidate
selection in BC occurs in two stages.
In the first stage, patients are asses-
200
172 178
sed to see if they are suitable to be
180
“activated” on the waiting list, and in
160 155
the second stage a decision is made
140 regarding which patient will receive a
120 given donor organ.
100 During assessment, scoring sys-
80
tems are used to determine patient sta-
tus and suitability. One of these sys-
60
35 36 32 tems is the model for end-stage liver
40 disease (MELD), which was original-
20 ly developed to estimate procedure-
0 related mortality in patients undergoing
2003 2004 2005
transjugular intrahepatic portosystem-
Referrals Transplants ic shunts.7 Today MELD is the most
commonly used prognostic model for
estimating disease severity and sur-
Figure 2. Number of referrals vs number of transplants in BC, 2003–2005.
vival in end-stage liver disease. It has
Source: BC Transplant
been prospectively validated in sever-
al patient populations and is currently
Initial referrals for liver transplant are on a liver transplant wait list. BC used by most transplant centres in the
assessment usually come from com- Transplant data for the number of world. The MELD score is based on
munity specialists with expertise in referrals for transplantation and the laboratory values for serum bilirubin,
the area who have decided that there number of transplants performed re- serum creatinine, and international
are no options other than transplanta- flect the situation across North Amer- normalized ratio (INR) in a log-
tion. While the number of liver trans- ica, and mean longer waiting times for transformed equation where Ln is
plants has increased across North very ill patients ( Figure 2 ). In recent the natural logarithm: (3.8[Ln serum
America, there has been a greater years the rate of death on the wait list bilirubin (mg/dL)] + 11.2[Ln INR] +
increase in the number of patients who has been approximately 30%. 9.6[Ln serum creatinine (mg/dL)] + 6.4).
204 BC MEDICAL JOURNAL VOL. 52 NO. 4, MAY 2010 www.bcmj.org](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Liver Transplantation: Current Status and Patient Selection in BC
Similar to Liver Transplantation: Current Status and Patient Selection in BC (20)
More from British Columbia Medical Journal
More from British Columbia Medical Journal (15)
Recently uploaded
Recently uploaded (20)
Liver Transplantation: Current Status and Patient Selection in BC
- 1. Mazhar Haque, MBBS, FRACP, Charles H. Scudamore, MD, FRCSC, Urs P. Steinbrecher, MD, FRCPC, Stephen W. Chung, MD, FRCSC, Andrzej K. Buczkowski, MD, FRCSC, Siegried R. Erb, MD, FRCPC, Eric M. Yoshida, MD, FRCPC Liver transplantation: Current status in British Columbia While the number of liver transplants performed across North America has increased, there has been an even greater increase in the number of patients who are on a liver transplant wait list. he first successful human liv- Today orthotopic liver transplan- T ABSTRACT: Orthotopic liver trans- plantation has become an accepted er transplant was performed tation (OLT) has become an accepted treatment for patients with acute or by Dr Thomas Starzl and his treatment for patients with acute or chronic decompensated liver dis- colleagues in 1968 in Colorado on an chronic decompensated liver disease ease of various causes. In British 18-month-old child who survived of various causes, as well as a form of Columbia, liver transplantation has 400 days. Despite improved technical gene replacement therapy for several been performed since 1989. Today aspects of transplant surgery, the 1-year systemic metabolic diseases in the up to 35% of all transplantations are survival rates were not above 35% in absence of structural liver disease. In done in patients with hepatitis C. the 1960s and 1970s, mainly because BC this most notably takes the form of While there are few absolute con- of graft failure due to allograft rejec- urea cycle defects in adolescence.5 traindications to transplantation, tion. A major breakthrough in the field Approximately 400 liver transplants there are some relative ones, includ- was the development of calcineurin are performed in Canada every year. ing age and certain comorbidities. inhibitors, with a landmark paper In British Columbia liver transplanta- After transplantation, the primary reporting 11 of 12 patients alive 1 year tion has been available since 1989. care provider has an important role post-transplant on cyclosporine-based The number of transplants performed to play in surveillance and treatment immunosuppresion.1 The availability increased from 3 in 1989 to 47 in 2008. of the patient’s global health needs. of tacrolimus as an alternative to Although post-transplant survival cyclosporine2 and the introduction of Dr Haque is a hepatology fellow in the has been excellent, a tragic dispari- other immunosuppressive agents, in- Division of Gastroenterology at the Universi- ty exists between organ availability cluding biologicals and mycopheno- ty of British Columbia. Dr Scudamore is and need, which results in a 30% late mofetil, as well as refinements of an associate professor of surgery in the mortality rate on the liver transplant surgical techniques, intensive care, Department of Surgery at UBC. Dr Stein- wait list in BC. Careful patient selec- and diagnostic modalities, have led brecher is a professor of medicine in the Divi- tion and optimal organ allocation is to current 1-year survival rates of 85% sion of Gastroenterology at UBC. Dr Chung critical given the scarcity of this life- to 95% and 5-year survival rates of is a professor of surgery in the Department saving resource. 75% after liver transplantation in BC of Surgery at UBC. Dr Buczkowski is a clini- ( Figure 1 ).3 In contrast, the expected cal associate professor of surgery in the survival of a patient with Child class Department of Surgery at UBC. Dr Erb is a C cirrhosis is in the order of 20% to clinical assistant professor of medicine in the 30% at 1 year. In addition to the sur- Division of Gastroenterology at UBC. Dr vival benefit, liver transplantation Yoshida is a professor of medicine and head provides patients with a distinct of the Division of Gastroenterology at UBC. improvement in quality of life.4 All are affiliated with BC Transplant. www.bcmj.org VOL. 52 NO. 4, MAY 2010 BC MEDICAL JOURNAL 203
- 2. Liver transplantation: Current status in British Columbia Patient selection 100% Careful patient selection and proper organ allocation are critical given the 90% scarcity of this life-saving resource. The transplant team has an ethical 80% obligation to act in the best interests Survival rate of both the individual patient referred 70% for assessment and the entire group of patients who are in need of trans- 60% plantation. 6 A successful outcome Patient survival depends on optimal patient selection 50% Graft survival and timing. 40% 0 1 2 3 4 5 6 7 8 9 10 General considerations Years post-transplant A patient should be considered for liver transplantation if this option extends life expectancy and improves Figure 1. Patient and graft survival for first liver transplants in BC, 1995–2004. quality of life beyond the expectation Source: BC Transplant of the natural history of the underly- ing liver disease. Current candidate selection in BC occurs in two stages. In the first stage, patients are asses- 200 172 178 sed to see if they are suitable to be 180 “activated” on the waiting list, and in 160 155 the second stage a decision is made 140 regarding which patient will receive a 120 given donor organ. 100 During assessment, scoring sys- 80 tems are used to determine patient sta- tus and suitability. One of these sys- 60 35 36 32 tems is the model for end-stage liver 40 disease (MELD), which was original- 20 ly developed to estimate procedure- 0 related mortality in patients undergoing 2003 2004 2005 transjugular intrahepatic portosystem- Referrals Transplants ic shunts.7 Today MELD is the most commonly used prognostic model for estimating disease severity and sur- Figure 2. Number of referrals vs number of transplants in BC, 2003–2005. vival in end-stage liver disease. It has Source: BC Transplant been prospectively validated in sever- al patient populations and is currently Initial referrals for liver transplant are on a liver transplant wait list. BC used by most transplant centres in the assessment usually come from com- Transplant data for the number of world. The MELD score is based on munity specialists with expertise in referrals for transplantation and the laboratory values for serum bilirubin, the area who have decided that there number of transplants performed re- serum creatinine, and international are no options other than transplanta- flect the situation across North Amer- normalized ratio (INR) in a log- tion. While the number of liver trans- ica, and mean longer waiting times for transformed equation where Ln is plants has increased across North very ill patients ( Figure 2 ). In recent the natural logarithm: (3.8[Ln serum America, there has been a greater years the rate of death on the wait list bilirubin (mg/dL)] + 11.2[Ln INR] + increase in the number of patients who has been approximately 30%. 9.6[Ln serum creatinine (mg/dL)] + 6.4). 204 BC MEDICAL JOURNAL VOL. 52 NO. 4, MAY 2010 www.bcmj.org
- 3. Liver transplantation: Current status in British Columbia High MELD scores are associated with a poor short-term prognosis. (An online Acute fulminant Other Autoimmune chronic MELD calculator that accepts SI units hepatitis 9% active hepatitis is accessible at www.mdcalc.com/ 8% 6% meld.) One of the requirements for Tumor 1% Chronic hepatitis listing in the United Network for Type B Organ Sharing in the US is a MELD Other chronic 10% score of at least 14. With scores lower diseases 6% than 14, short-term prognosis without transplantation is predicted to be Primary sclerosing similar or better than that with trans- cholangitis plantation. Conversely, 3-month sur- 3% Chronic hepatitis vival drops to less than 20% in patients Primary Type C biliary 35% with a MELD score of 40. Some of cirrhosis Cirrhosis alcoholic these patients may be too sick for 12% 10% transplantation. The Child-Turcotte-Pugh (CTP) is another scoring system for quanti- Figure 3. Liver transplants in BC by primary diagnosis, 2003–2005. fying the severity of liver disease. It Source: BC Transplant scores five variables: ascites, serum albumin, bilirubin, INR, and encepha- lopathy. CTP is less useful for assign- patients the best chance for a favor- ribavirin is associated with sustained ing priority on a transplant wait list able outcome. virological response of approximately because two of the parameters (ascites 27% (23% to 31%).12 Use of growth and encephalopathy) are subjective. Chronic hepatitis C factors to support the hematological Furthermore, it has not been validated Up to 35% of all liver transplantations parameters may improve compliance as a reliable indicator of short-term are done in patients with chronic and success of antiviral therapy after prognosis. For those reasons, MELD hepatitis C–related liver disease. Re- transplant.9 Immunoglobulin therapy is now the only scoring system used in currence of HCV infection in the for HCV has been found to be inef- the United States for allocating organs transplanted organ is universal,9,10 but fective.13 from deceased liver donors. In BC we the rate of progression is quite vari- consider the global clinical assess- able. About 20% of patients develop Chronic hepatitis B ment of the candidate as well as rapidly progressive fibrosis that may Significant improvements have been MELD and CTP scores when allocat- lead to graft failure within a few years made recently in the treatment of ing a donor organ. Patients who re- of transplantation. However, most chronic hepatitis B infection; howev- ceive organs in BC have usually been studies show 5-year survival rates in er, liver transplantation remains the diagnosed with the conditions and dis- HCV-positive recipients to be similar only option for many patients with eases described below ( Figure 3 ). to those in HCV-negative recipients. end-stage liver disease due to HBV. Some of these patients will have rela- After the incorporation of hepati- Fulminant hepatic failure tively quiescent disease for many tis B immunoglobulin (HBIG) along Fulminant hepatic failure (FHF) is the years, but in general the rate of fibro- with combination antiviral therapy, acute onset of liver failure with devel- sis progression is faster in the trans- the 1- and 5-year survival rates of opment of encephalopathy in a short planted liver than in the native liver. patients transplanted for HBV equals period of time. Despite the differences Successful treatment of HCV before that of non-HBV transplant patients.14 in etiology, the progression of FHF is transplantation usually prevents post- Several reports show a combination similar in all cases.8 Without liver operative recurrence but is often not of lamivudine and low-dose intramus- transplantation, patients with FHF feasible. Unfortunately, antiviral treat- cular HBIG are effective in prevent- will either have a complete recovery ment after liver transplantation is ing allograft reinfection by HBV at of liver function or will die. Early often poorly tolerated.11 The combina- higher intravenous doses.15 Studies referral to a transplant centre gives tion treatment of peginterferon and have also suggested that the rate of www.bcmj.org VOL. 52 NO. 4, MAY 2010 BC MEDICAL JOURNAL 205
- 4. Liver transplantation: Current status in British Columbia reinfection can be reduced further if non-ALD are comparable.18,19 waiting for an organ. Bridging mod- the anti-HBs titers are kept consis- All Canadian transplant centres, alities such as transcatheter arterial tently above 500 IU/L.16 A recent study as well as most American centres, chemoembolization, radiofrequency of intramuscular low-dose HBIG (400 require a documented 6-month mini- ablation, percutaneous ethanol injec- to 800 IU daily for 1 week then month- mum period of supervised abstinence tion, and surgical resection are also ly) plus lamivudine (100 mg daily) in association with some form of alco- used in carefully selected patients. following liver transplantation show- hol rehabilitation before transplanta- ed patient survival was 92% at 1 year tion. Like BC, many centres expect Autoimmune hepatitis and 88% at 5 years. A higher HBV patients to sign a contract to maintain Autoimmune hepatitis (AIH) is an ex- DNA titer at baseline was associated abstinence. Six months of abstinence cellent indication for liver transplan- with an increased risk of recurrence. with a good social support system is tation. Five-year patient and graft sur- There is no consensus on the most associated with a favorable outcome.20 vival after liver transplantation range appropriate initial antiviral therapy. A A 6-month abstinence requirement from 83% to 92%.25 There is a high combination of lamivudine and ade- also gives patients a chance to recov- prevalence of autoimmune liver dis- fovir/tenofovir, as well as entecavir, er spontaneously from advanced liver ease, specifically AIH and primary along with HBIG is currently used in disease and thereby avoid transplanta- biliary cirrhosis (PBC), among British our centre. Combination therapy allows tion. When transplantation is neces- Columbia’s First Nations people.26 more rapid viral suppression and min- sary, abstinence also affects immedi- Patients with autoimmune liver imizes the risk of drug resistance when ate postoperative outcome. disease may have fairly rapid clinical compared with using each of these decompensation after a long period of drugs alone. Active immunization Hepatocellular carcinoma disease stability. Such episodes may using standard hepatitis B vaccines Hepatocellular carcinoma (HCC) is not be well tolerated and thus permit has been explored as an alternative to one of the most common cancers little time to undertake pre-transplant lifelong HBIG prophylaxis. Unfortu- worldwide and is the most frequent assessment. Liver transplantation is nately, anti-HBs titers achieved in the primary malignancy of the liver. It indicated for patients who are refrac- responders were low despite the use ranks third among causes of cancer- tory to or intolerant of immunosup- of higher doses and multiple courses related deaths. In the US, there has pressive therapy and develop end- of vaccine.17 been a 70% increase in HCC over a stage liver disease. A subset of patients 20-year period, which is likely due to may present with fulminant hepatitis Alcoholic liver disease the HCV epidemic,21 and similar trends and liver failure. All patients with ful- Alcoholic liver disease (ALD) is the have been projected in a Canadian minant disease should be transferred third most common indication for study.22 It is not uncommon to find to a liver transplant centre for moni- liver transplant in British Columbia HCC in patients with viral hepatitis or toring and management. The rate of and the second leading cause for trans- alcoholic liver disease during pre- acute and chronic allograft rejection plant after viral hepatitis in many transplant assessment. Only selected and steroid-resistant rejection is high- western countries, although the ALD patients with HCC who meet accept- er among AIH post-transplant patients. group often has additional primary able criteria (Milan criteria) are con- The recurrence rate of primary dis- liver disease causes (e.g., hepatitis C). sidered for transplant. ease is also higher—at least 17%.27 Due to the lack of consensus on a def- Vascular invasion is the most im- inition for “relapse,” there is discrep- portant prognostic factor for HCC and Primary biliary cirrhosis ancy among published reports of post- is present in up to 50% of tumors PBC is one of the most common indi- transplant alcoholism relapse rates, greater than 5 cm.23 HCC is an aggres- cations for liver transplantation in which range from less than 10% to sive tumor. The wait list dropout rate British Columbia and the rest of the 90%.18 as a result of tumor progression western world. The current 5-year sur- Transplantation for alcoholic liver beyond acceptable criteria is between vival rate for liver transplant because disease in an era of organ shortage and 5% and 20%.24 To overcome this prob- of PBC is 80% to 90%.28 Management against a background of recidivism lem, a MELD score of 22 is automat- of progressive PBC requires predict- raises both ethical and clinical con- ically assigned to high-risk HCC ing the prognosis and optimal time for cerns. However, survival rates follow- patients (solitary lesions 2 to 5 cm or transplantation. A model developed at ing liver transplant for both ALD and up to three lesions of 3 cm) currently the Mayo Clinic that does not require 206 BC MEDICAL JOURNAL VOL. 52 NO. 4, MAY 2010 www.bcmj.org
- 5. Liver transplantation: Current status in British Columbia liver biopsy has been used for predic- Metabolic diseases tions in the recent past may no longer tion.29 Prognosis is predicted from the Liver transplantation may play a vital even qualify as relative contraindica- patient’s age, serum bilirubin, and role in the management of hemochro- tions. Current absolute contraindica- al bumin concentrations, the pro- matosis, Wilson’s disease (WD), and tions include uncontrolled infection, thrombin time, and the presence of alpha-1 antitrypsin deficiency. Liver extrahepatic malignancy, severe cardio- edema. Of these variables, serum transplantation is the only effective pulmonary comorbidity, noncompli- bilirubin concentration is the most option for those with WD who present ance, active substance abuse, advanced heavily weighted. Patients should be with acute liver failure. It is also indi- hepatoma, and cholangiocarcinoma. referred for transplant assessment cated for all patients with WD who Relative contraindications include when their serum bilirubin concen- have decompensated liver disease un- extreme age and difficult psychoso- tration approaches 100 µmol/L and responsive to medical therapy. Liver cial factors. before it reaches 150 µmol/L.30 Primary sclerosing cholangitis Liver transplantation is the treatment of choice for patients with end-stage At present there are relatively few primary sclerosing cholangitis (PSC). absolute contraindications to liver Five-year survival after transplanta- tion is as high as 85%.31 As it has for transplantation. Conditions that were PBC, the Mayo Clinic has devised a considered as absolute contraindications model for predicting lifespan in prima- ry sclerosing cholangitis. It includes in the past may no longer even qualify as age, serum bilirubin, serum albumin, relative contraindications. serum AST, and a history of variceal bleeding.32 The model suggests that liver transplantation be undertaken when the estimated 6-month survival is less than 80%. A generally accepted transplantation corrects the hepatic A retrospective study of BC Trans- list of indications in PSC also includes metabolic defects of WD and may nor- plant data collected from 1997 to 2001 quality-of-life issues such as intract- malize extrahepatic copper metabo- reveals that 150 of 737 patients re- able itch or fatigue. lism.36 One-year survival following ferred for assessment were considered Recurrence of PSC following liv- liver transplantation ranges from 79% unsuitable. Of these, 74 patients (49%) er transplantation in up to 20% of to 87%. Data collected between 1997 were found unsuitable on medical patients has been reported in several and 2006 from the United Network for grounds. The most common cause for studies.33 The diagnosis of recurrence Organ Sharing indicate that recipients medical unsuitability was no need for is based upon consistent findings on with a diagnosis of hemochromatosis liver transplant—29 patients (39%). liver biopsy and cholangiography in had 1-, 3-, and 5-year survival rates Other medical causes included hepa- the absence of other conditions that comparable to that of all other trans- toma or extrahepatic malignancy—20 could lead to similar findings, such as plant recipients.37 Transplantation may patients (27%)—and multisystem fail- hepatic artery thrombosis, dominant also cure the underlying metabolic ure—12 patients (16%). Psychosocial anastomotic stricture, or ABO blood disorder of alpha-1 antitrypsin defi- contraindication accounted for 73 group mismatched liver allograft. ciency since the metabolic defects patients (49%). Within this group, The risk of cholangiocarcinoma is reside within the liver.38 failure to meet minimal alcohol absti- increased in PSC patients, with report- nence criteria excluded the largest ed life-time prevalence rates varying Contraindications number of patients (39, 53.4%) fol- from 5% to 20%.34 Several reports and challenges lowed by unsatisfactory social sup- have suggested that the incidence of At present there are relatively few port (12, 16.4%), medical noncompli- colon cancer is increased in patients absolute contraindications to liver ance (10, 13.7%), and active substance with ulcerative colitis and PSC who transplantation. Conditions that were abuse (6, 8.2%).39 undergo liver transplantation.35 considered as absolute contraindica- www.bcmj.org VOL. 52 NO. 4, MAY 2010 BC MEDICAL JOURNAL 207
- 6. Liver transplantation: Current status in British Columbia HIV vival in a study among HIV patients tive complications than a deceased Prior to the introduction of highly was similar to that among age and race donor transplant. There are also sig- active antiretroviral therapy (HAART), comparable patients without HIV.42 nificant risks to the donor that must be the transplantation outcomes for pa- British Columbia is one of the few addressed when considering risks and tients with human immunodeficiency centres in Canada that have been rou- benefits of LDLT versus deceased virus infection were unfavorable.40 tinely assessing HIV patients with donor liver transplantation. Because HIV and HCV have similar end-stage liver diseases for transplan- tation. Complex drug interactions, Retransplantation immunosuppressive dosing, and the Currently, retransplantation accounts possibility of HCV recurrence are the for almost 10% of all liver transplants. main issues that require the special Retransplantation is effective in the Patients progressing consideration of an experienced mul- setting of primary nonfunction. Sur- tidisciplinary team. vival after retransplantation for late- beyond their 1-year onset graft failure is less than after ini- post-transplant Age tial transplantation.44 The outcome of Transplantation in extreme-age pa- retransplantation for recurrent HCV is anniversary will mostly tients, either very young or old, is dif- poor and this remains a controversial be stable and will need ficult. However, the age boundary is subject. ever-changing. It has been reported their primary care that there are no differences in post- Role of the primary providers to actively transplant outcomes in older versus care physician younger patients in several centres. Primary care physicians play a very participate in Transplant can be successfully per- important role in liver transplantation. surveillance and formed in patients as old as 70. In BC All physicians in BC need to under- the general philosophy is to consider stand that the role of BC Transplant is treatment of their the “biological age” rather than the limited to assessment and investiga- global health needs. “chronological age.” tion for transplant suitability and fea- sibility in the pre-transplant period. Comorbidities As pre-transplant referrals arise from It is part of the assessment process to all regions of BC and the Yukon, it is evaluate any existing comorbidity and not possible for the Liver Transplant transmission routes, 16% to 29% of decide whether it increases surgical Program to assume primary and sec- HIV-infected patients have coinfec- and anesthetic risk. Cardiovascular ondary care of these patients, so the tion with hepatitis C.41 While survival and pulmonary morbidity, including community primary care physicians of HIV infection is improving on coronary artery disease, need careful and specialists still need to follow HAART, hepatitis-related end-stage consideration. Potential surgical prob- these patients. Post-transplant, the liver disease has become a major lems such as portal vein thrombosis Liver Transplant Program follows all cause of morbidity and mortality in and other anatomical difficulties re- patients carefully and manages all this group. Patients with HIV and sulting from previous abdominal surg- post-transplant complications. How- HCV coinfection progress faster to eries and trauma are also carefully ever, patients progressing beyond cirrhosis than patients with HCV explored. their 1-year post-transplant anniver- alone; the morbidity and mortality risk sary will mostly be stable and will of end-stage liver disease and hepato- Living donor liver need their primary care providers to cellular carcinoma is also increased. transplantation actively participate in surveillance Patients can be considered for In response to the growing shortage and treatment of their global health transplantation with a current CD4 of organs from deceased donors, adult needs. count of more than 200 per mL, low living donor liver transplantation HIV viral load, and limited oppor- (LDLT) was introduced in 1998.43 This Conclusions tunistic complications with standard is a technically demanding procedure Over the past 20 years liver transplan- listing criteria. The cumulative sur- and carries higher risks of postopera- tation has evolved in BC from a pro- 208 BC MEDICAL JOURNAL VOL. 52 NO. 4, MAY 2010 www.bcmj.org
- 7. Liver transplantation: Current status in British Columbia cedure considered experimental to 506) and cyclosporine for immunosup- dian transplant hepatology workshop. standard therapy for patients with end- pression in liver transplantation. N Engl J Can J Gastroenterol 2006;20:725-734. stage liver disease. Today the main Med 1994;331:1110-1115. 10. Gane EJ, Portmann BC, Naoumov NV, et limitation is the tragic disparity be- 3. Walker SR, Parsons DA, Coplestons P, et al. Long-term outcome of hepatitis C tween organ availability and organ al. The Canadian Organ Replacement infection after liver transplantation. N need. Given the scarcity of available Register. Clin Transpl 1996:91-107. Engl J Med 1996;334:815-820. donor organs and the physiologically demanding nature of every liver trans- plant operation, candidates need to be evaluated carefully for medical and psychological comorbidities to im- prove the post-transplant outcome. Given the scarcity of available donor Although not all patients referred for liver transplantation can undergo liver organs and the physiologically demanding transplantation, the Liver Transplant nature of every liver transplant operation, Program ensures that all are treated fairly. candidates need to be evaluated carefully to improve the post-transplant outcome. Acknowledgments On the 20th anniversary of the Liver Trans- plant Program, the authors sincerely thank the staff of the BC Transplant Society; the nurses of the Solid Organ Transplant Ward, the Solid Organ Transplant Clinic, the 4. Hunt CM, Tart JS, Dowdy E, et al. Effect 11. Watt KD, Lyden ER, McCashland TM. Department of Pharmacy, the intensive of orthotopic liver transplantation on Poor survival after liver retransplantation: care unit and the operating room staff of employment and health status. Liver Is hepatitis C to blame? Liver Transpl the Vancouver General Hospital, and the Transpl Surg 1996;2:148-153. 2003;9:1019-1024. staff of the Fraser Valley Transplant Clinic. 5. Sirrs S, Yoshida E, Wong L, et al. Ortho- 12. Rodriguez-Luna H, Khatib A, Sharma P, et The authors especially thank the living relat- topic liver transplantation in a patient with al. Treatment of recurrent hepatitis C ed donors and the families of the cadaver- carbamyl phosphate synthetase defi- infection after liver transplantation with ic organ donors, without whom lifesaving ciency and cystic fibrosis. Paediatr Child combination of pegylated interferon liver transplantation would not be possible. Health 2003;8:497-498. alpha2b and ribavirin: An open-label 6. Yoshida EM. Selecting candidates for series. Transplantation 2004;77:190-194. Competing interests liver transplantation: A medical ethics 13. Davis GL, Nelson DR, Terrault N, et al. A Dr Steinbrecher served on an Astellas Phar- perspective on the microallocation of a randomized, open-label study to evaluate ma advisory board for clinical trials in 2009 scarce and rationed resource. Can J Gas- the safety and pharmacokinetics of and received a liver transplant fellow troenterol 1998;12:209-215. human hepatitis C immune globulin stipend from 2004 to 2009. Dr Yoshida has 7. Kamath PS, Wiesner RH, Malinchoc M, (Civacir) in liver transplant recipients. received honoraria and unrestricted re- et al. A model to predict survival in Liver Transpl 2005;11:941-949. search grants from a range of pharmaceu- patients with end-stage liver disease. 14. Steinmuller T, Seehofer D, Rayes N, et al. tical companies, including Roche, Scher- Hepatology 2001;33:464-470. Increasing applicability of liver transplan- ing-Plough, Gilead, and Novartis. 8. Ostapowicz G, Fontana RJ, Schiodt FV, tation for patients with hepatitis B-relat- et al. Results of a prospective study of ed liver disease. Hepatology 2002;35: References acute liver failure at 17 tertiary care cen- 1528-1535. 1. Starzl TE, Klintmalm GB, Porter KA, et al. ters in the United States. Ann Intern Med 15. Yoshida EM, Erb SR, Partovi N, et al. Liver Liver transplantation with use of cyclo- 2002;137:947-954. transplantation for chronic hepatitis B sporin a and prednisone. N Engl J Med 9. Watt KD, Burak K, Deschenes M, et al. infection with the use of combination 1981;305:266-269. Recurrent hepatitis C post-transplanta- lamivudine and low-dose hepatitis B 2. The US Multicenter FK506 Liver Study tion: Where are we now and where do immune globulin. Liver Transpl Surg Group. A comparison of tacrolimus (FK we go from here? A report from the Cana- 1999;5:520-525. www.bcmj.org VOL. 52 NO. 4, MAY 2010 BC MEDICAL JOURNAL 209
- 8. Liver transplantation: Current status in British Columbia 16. McGory RW, Ishitani MB, Oliveira WM, tion: A 10-year retrospective analysis. 38. Vennarecci G, Gunson BK, Ismail T, et al. et al. Improved outcome of orthotopic Can J Gastroenterol 2000;14:775-779. Transplantation for end stage liver dis- liver transplantation for chronic hepatitis 27. Neuberger J. Transplantation for autoim- ease related to alpha 1 antitrypsin. Trans- B cirrhosis with aggressive passive mune hepatitis. Semin Liver Dis 2002; plantation 1996;61:1488-1495. immunization. Transplantation 1996;61: 22:379-386. 39. Alali J, Ramji A, Ho JK, et al. Liver trans- 1358-1364. 28. Liermann Garcia RF, Evangelista Garcia plant candidacy unsuitability: A review of 17. Lo CM, Liu CL, Chan SC, et al. Failure of C, McMaster P, et al. Transplantation for the British Columbia experience. Can J hepatitis B vaccination in patients receiv- primary biliary cirrhosis: Retrospective Gastroenterol 2006;20:95-99. ing lamivudine prophylaxis after liver analysis of 400 patients in a single center. 40. Bouscarat F, Samuel D, Simon F, et al. An transplantation for chronic hepatitis B. J Hepatology 2001;33:22-27. observational study of 11 French liver Hepatol 2005;43:283-287. 29. Wiesner RH, Porayko MK, Dickson ER, transplant recipients infected with 18. McMaster P. Transplantation for alcoholic et al. Selection and timing of liver trans- human immunodeficiency virus type 1. liver disease in an era of organ shortage. plantation in primary biliary cirrhosis and Clin Infect Dis 1994;19:854-859. Lancet 2000;355(9202):424-425. primary sclerosing cholangitis. Hepatol- 41. Sherman KE, Rouster SD, Chung RT, et 19. Bird GL, O’Grady JG, Harvey FA, et al. ogy 1992;16:1290-1299. al. Hepatitis C Virus prevalence among Liver transplantation in patients with alco- 30. Neuberger JM, Gunson BK, Buckels JA, patients infected with human immuno- holic cirrhosis: Selection criteria and rates et al. Referral of patients with primary bil- deficiency virus: A cross-sectional analy- of survival and relapse. BMJ 1990;301: iary cirrhosis for liver transplantation. Gut sis of the US adult AIDS Clinical Trials 15-17. 1990;31:1069-1072. Group. Clin Infect Dis 2002;34:831-837. 20. Gish RG, Lee AH, Keeffe EB, et al. Liver 31. Graziadei IW, Wiesner RH, Marotta PJ, 42. Ragni MV, Belle SH, Im K, et al. Survival transplantation for patients with alco- et al. Long-term results of patients under- of human immunodeficiency virus-infect- holism and end-stage liver disease. Am J going liver transplantation for primary ed liver transplant recipients. J Infect Dis Gastroenterol 1993;88:1337-1342. sclerosing cholangitis. Hepatology 1999; 2003;188:1412-1420. 21. El-Serag HB, Davila JA, Petersen NJ, et 30:1121-1127. 43. Brown RS, Jr., Russo MW, Lai M, et al. A al. The continuing increase in the inci- 32. Kim WR, Therneau TM, Wiesner RH, et survey of liver transplantation from living dence of hepatocellular carcinoma in the al. A revised natural history model for pri- adult donors in the United States. N Engl United States: An update. Ann Intern mary sclerosing cholangitis. Mayo Clin J Med 2003;348:818-825. Med 2003;139:817-823. Proc 2000;75:688-694. 44. Facciuto M, Heidt D, Guarrera J, et al. 22. Zou S, Tepper M, El Saadany S. Predic- 33. Campsen J, Zimmerman MA, Trotter JF, Retransplantation for late liver graft fail- tion of hepatitis C burden in Canada. Can et al. Clinically recurrent primary scleros- ure: Predictors of mortality. Liver Transpl J Gastroenterol 2000;14:575-580. ing cholangitis following liver transplan- 2000;6:174-179. 23. Figueras J, Ibanez L, Ramos E, et al. tation: A time course. Liver Transpl 2008; Selection criteria for liver transplantation 14:181-185. in early-stage hepatocellular carcinoma 34. Bergquist A, Broome U. Hepatobiliary with cirrhosis: Results of a multicenter and extrahepatic malignancies in primary study. Liver Transpl 2001;7:877-883. sclerosing cholangitis. Best Pract Res 24. Yao FY, Bass NM, Nikolai B, et al. Liver Clin Gastroenterol 2001;15:643-656. transplantation for hepatocellular carci- 35. Vera A, Gunson BK, Ussatoff V, et al. Col- noma: Analysis of survival according to orectal cancer in patients with inflamma- the intention-to-treat principle and tory bowel disease after liver transplan- dropout from the waiting list. Liver tation for primary sclerosing cholangitis. Transpl 2002;8:873-883. Transplantation 2003;75:1983-1988. 25. Ratziu V, Samuel D, Sebagh M, et al. 36. Groth CG, Dubois RS, Corman J, et al. Long-term follow-up after liver transplan- Metabolic effects of hepatic replacement tation for autoimmune hepatitis: Evi- in Wilson’s disease. Transplant Proc dence of recurrence of primary disease. 1973;5:829-833. J Hepatol 1999;30:131-141. 37. Yu L, Ioannou GN. Survival of liver trans- 26. Yoshida EM, Caron NR, Buczkowski AK, plant recipients with hemochromatosis et al. Indications for liver transplantation in the United States. Gastroenterology in British Columbia’s Aboriginal popula- 2007;133:489-495. 210 BC MEDICAL JOURNAL VOL. 52 NO. 4, MAY 2010 www.bcmj.org