2 of 21
CourseOverview
2 of 21
Welcome and Introductions
• Course Director
• Faculty
• Course Coordinator
3.
3 of 21
CourseOverview
3 of 21
Welcome and Introductions
We would like you to introduce yourselves now:
Who are you?
What is your professional background?
What is your experience with trauma?
What do you hope to gain from this course?
4.
4 of 21
CourseOverview
4 of 21
Safe Learning Environment
• Interactive, unfolding case discussions, stimulus questions
• Participation required
• Respect for each other
• Try answering the questions – it’s ok if you get it wrong
5.
5 of 21
CourseOverview
5 of 21
M
43 year old male, driver MVC,
involved in head on collision
with truck
I
Right sided bruising and
abrasions on Chest, deformed
right leg,
S
Non responsive, RR 30, HR 130,
BP 80/60
T
On spine board with C spine
collar
Discussion Question:
What are your concerns with this
patient?
6.
6 of 21
CourseOverview
6 of 21
The ATLS course provides one
acceptable method for the safe,
immediate management of
trauma patients.
7.
7 of 21
CourseOverview
7 of 21
Program Goals
ATLS course provides participants with a safe and reliable method to:
1. Assess a patient’s condition rapidly and accurately.
2. Resuscitate and stabilize patients according to priority.
3. Determine whether a patient’s needs exceed a facility’s resources and/or provider’s
capabilities.
4. Arrange transfer when indicated
8.
8 of 21
CourseOverview
8 of 21
Course Objectives
Upon completion of the ATLS student course, you will be able to:
1. Demonstrate the concepts and principles of the primary and secondary
patient assessments.
2. Establish management priorities in the initial management of a trauma
patient.
3. Initiate the primary and secondary management of a simulated trauma
patient in a timely manner.
4. In a given trauma simulation, demonstrate the skills that are often required
in the initial assessment and treatment of patients with multiple injuries.
9.
9 of 21
CourseOverview
9 of 21
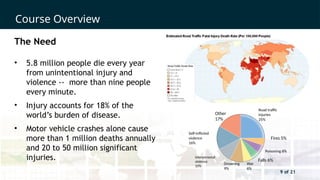
The Need
• 5.8 million people die every year
from unintentional injury and
violence -- more than nine people
every minute.
• Injury accounts for 18% of the
world’s burden of disease.
• Motor vehicle crashes alone cause
more than 1 million deaths annually
and 20 to 50 million significant
injuries.
Self-inflicted
violence
16%
Interpersonal
violence
10%
Other
17%
Road traffic
injuries
25%
Fires 5%
Poisoning 6%
Falls 6%
War
6%
Drowning
9%
10.
10 of 21
CourseOverview
10 of 21
ATLS provides a
common language
12 of 21
CourseOverview
12 of 21
“When I can provide better
care in the field with
limited resources than what
my children and I received
at the primary care facility,
there is something wrong
with the system, and the
system has to be changed.”
James Styner, MD, FACS
1977
13.
13 of 21
CourseOverview
13 of 21
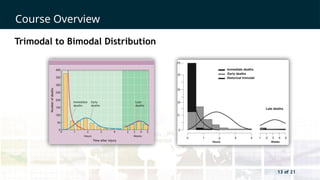
Trimodal to Bimodal Distribution
14.
14 of 21
CourseOverview
14 of 21
ATLS Concept
• Follow ABCDE approach to evaluation and treatment.
• Treat the greatest threat to life first.
• Recognize the definitive diagnosis is not immediately important.
• Understand that time is of the essence.
• Do no further harm.
15.
15 of 21
CourseOverview
15 of 21
ATLS Concept
Airway with restriction of cervical spine motion
Breathing and ventilation
Circulation with hemorrhage control
Disability: Neurological status
Exposure / Environmental control
16.
16 of 21
CourseOverview
16 of 21
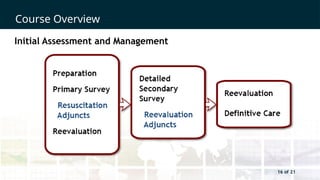
Initial Assessment and Management
17.
17 of 21
CourseOverview
17 of 21
ATLS Educational Format
• Introductory lecture
• Interactive group discussions
• Interactive skill sessions
• Simulated patient scenarios
• Written examinations
• mATLS online learning modules
• MyATLS mobile app
18.
18 of 21
CourseOverview
18 of 21
International ATLS Program
• 83 countries
• 3,380 courses
• 68,000 students
• MyATLS mobile app 181 countries,
216,000 downloads
19.
19 of 21
CourseOverview
19 of 21
Impact of ATLS Program
• Documented improvement in the care of injured patients after
implementation of program
• Organized trauma care resulting in reduced injury mortality
• Retention of organizational and procedural skills
21 of 21
CourseOverview
21 of 21
Summary
• ABCDE approach to trauma care
• Do no further harm
• Treat the greatest threat to life first
• One safe way
• A common language
Editor's Notes
#2 Introduce all the faculty – including additional observers
#3 Take time to invite the participants to introduce themselves, so that the faculty can have an understanding of their audience, their experience and specialty.
#4 The success of the course relies on a safe learning environment and it is important to set the scene and explain what you mean by a safe environment.
#5 The idea of this scenario is to contextualise ATLS for the learner. You need to state that ATLS is one safe way of managing trauma in the first hour.
This is also the time to check if the participants know the MIST acronym and if not clarify:
M = Mechanism
I = Injuries
S = Vital signs
T= Treatment
#6 The ATLS course provides one acceptable method for the safe, immediate management of trauma patients.
#7 Program Goals
Read and explain each program goal.
1. Assess a patient’s condition rapidly and accurately.
2. Resuscitate and stabilize patients according to priority.
3. Determine whether a patient’s needs exceed a facility’s resources and/or provider’s capabilities.
4. Arrange appropriately for a patient’s interhospital or intrahospital transfer (what, who, when and how).
5. Ensure that optimal care is provided and that the level of care does not deteriorate at any point during the evaluation, resuscitation, or transfer process.
#8 Course Objectives
ATLS is primarily directed at providing initial care during the “Golden Hour.” The concept of the “golden hour” emphasizes the urgency necessary for successful treatment of injured patients and is not intended to represent a “fixed” time period of 60 minutes. Rather, it is the window of opportunity during which doctors can have a positive impact on the morbidity and mortality associated with injury.
The ATLS course provides the essential information and skills for doctors to identify and treat life-threatening and potentially life-threatening injuries under the extreme pressures associated with the care of these patients in the fast-paced environment and anxiety of a trauma room.
#9 The Need
According to the latest information from the WHO and CDC, more than nine people die every minute from injuries or violence and 5.8 million people of all ages and economic groups die every year from unintentional injuries and violence. The burden of injury is even more significant accounting for 18% of the world’s burden of disease. MVCs alone cause more than 1 million deaths and an estimated 20-50 million significant injuries; they are the leading cause of death due to injury worldwide. Improvements in injury control efforts are having an impact in most developed countries, where trauma remains the leading cause of death in persons 1-44 years of age. More than 90% of MVCs occur in the developing world. Global trauma-related costs are estimated to exceed $500 billion annually. This amount increases when lost wages, medical expenses, insurance administration costs, property damage, fire loss, employer costs, and indirect loss from work-related injuries are considered. Unfortunately federal research funding for trauma remains low, at less than 4 cents of each research dollar.
#11 The Beginning
In 1976, Dr. Styner, an orthopedic surgeon, crashed his plane in rural Nebraska. Dr. Styner and his three children were seriously injured, and his wife was killed instantly when she was impaled by the propeller of the plane. Dr. Styner sustained serious injuries, and three of his four children sustained critical injuries. The surviving family members were taken to a rural hospital, where they received inadequate care.
Before 1980, the delivery of trauma care in the United States was at best inconsistent.
#12 A group of surgeons and physicians in Nebraska, along with the Lincoln Medical Education Foundation, the Lincoln Area Mobile Heart Team nurses, the University of Nebraska Medical Center, the Nebraska State Committee on Trauma of the American College of Surgeons, and the Southeast Nebraska Emergency Medical Services, identified the need for training in advanced trauma life support. This occurred around the time the Advanced Cardiac Life Support (ACLS) course was developed in Nebraska, and ATLS was modeled after that course.
#13 In the early 1980s, Dr. Trunkey described a trimodal distribution of trauma deaths based on the time interval from injury to death (graph on screen left). Three distinct peaks could be identified. Since that time, trauma systems have been developed and trauma education standardized. A 2010 population study (graph screen right) involving a similar analysis failed to show the same 3 peaks. The immediate peak persisted, as did the early peak, likely reflecting improved prehospital care and the arrival of sicker patients faster from the field. The late peak was greatly diminished. Only 4% of deaths occurred after the first 24 hours, suggesting improvements in resuscitation and critical care and prevention and treatment of complications.
#14 ATLS Concept
ABCDE is the universal language for the primary exam. It is also the order in which the injuries will kill patients. The definitive diagnosis and an in-depth history are not required initially.
#15 ATLS Concept
ABCDE is the universal language for the primary exam. It is also the order in which the injuries will kill patients. The definitive diagnosis and an in-depth history are not required initially.
#16 Initial Assessment and Management
The primary survey, adjuncts and resuscitation should occur simultaneously.
Waiting for tests should not delay resuscitation and treatment.
Patients should be re-evaluated frequently after resuscitation and treatments.
Patients who exceed the capabilities of your facility should be identified early and arrangements made for transfer while continuing with resuscitation.
#17 ATLS Educational Format
Encourage the students to ask questions and clarify issues before moving on.
Participation in the interactive sessions increases retention.
The mATLS online course is an evolving aspect of the ATLS course, and the instructor/course director needs to know what is available at the time the course is given.
#19 A recently published study found surgery residents trained in ATLS had higher scores on the trauma section of a national board style, objective structured clinical examination (OSCE) than those without ATLS training
Bull Emerg Trauma 2016;4(2):75-79.
#21 Summary
ATLS provides an easily remembered approach to the evaluation and treatment of injured patients.