RBC
M.R. COLLEGE OFPHARMACEUTICAL
SCIENCES AND RESEARCH
( Affiliated by M.A.K.A.U.T , W.B.S.C.T.E. & V.E. )
NAME : MR. ASIM KUMAR JANA
UNIVERSITY REGISTRATION NO. :
SUBJECT : HUMAN ANATOMY AND PHYSIOLOGY – I (PT105)
CLASS ROLL NO. : 21
1ST
SEMESTER , 1ST
YEAR , B.PHARM
SUBMITTED BY -
SUBMITTED TO -
MR. ASIM KUMAR JANA
MR. SUBHADIP NANDI (ASSISTANT
PROFESSOR OF PHARMACOLOGY)
PAGE - 2
INTRODUCTION
RBC - red cells / red blood corpuscles / haematids /
erythroid cells / erythrocytes.
Derived from Greek erythros for "red" and kytos for
"hollow vessel", with cyte translated as "cell" in
modern usage.
Non-nucleated formed elements in the blood.
It lacks cytoplasmic organelles such as nucleolus,
mitochondria & ribosomes.
The red color of RBC is due to the presence of
Hemoglobin (90%).
4.
PAGE - 3
The cytoplasm of a red blood cell is rich in hemoglobin ,
an iron-containing biomolecule that can bind oxygen and is
responsible for the red color of the cells and the blood.
Each human red blood cell contains approximately
270 million hemoglobin molecules.
The cell membrane is composed of proteins and lipids, and
this structure provides properties essential for
physiological cell function such
as deformability and stability of the blood cell while
traversing the circulatory system and specifically the
capillary network.
In humans, mature red blood cells are flexible biconcave
disks.
Approximately 2.4 million new erythrocytes are produced
5.
PAGE - 4
DESCRIPTION
HISTORICAL BACKGROUND :-
JAN SWAMMERDAM-1658 - Dutch biologist and microscopist. He
called them ruddy globules
ANTON VAN LEEUWENHOEK-1674- Discovered Microscope and
established its size.
OTTO FUNKE 1851 - German physiologist was the first scientist to
successfully crystallize hemoglobin. "Blutfarbstoff“
DR. MAX PERUTZ- 1959 - by use of X-ray crystallography
unravelled the structure of hemoglobin
MENGHINI-1747- presence of iron in the blood, identified the red
corpuscles as the chief site of iron within the organism.
6.
PAGE -
PAGE -5
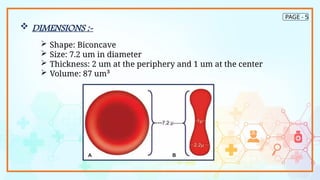
DIMENSIONS :-
Shape: Biconcave
Size: 7.2 um in diameter
Thickness: 2 um at the periphery and 1 um at the center
Volume: 87 um³
7.
PAGE -
6
NORMALCOUNT :-
Adults males : 4.5-6 million cu mm of
blood
Adult females : 4 - 5.5 million cu mm of
blood
At birth : 6.7 million cu mm of blood
COMPOSITION :-
62.5% water
35% Hemoglobin
2.5%
a)Sugar – glucose
b)Lipids - Cephalin, Cholesterol & Lecithin
c) Protein - Glutathion: insoluble protein which acts as
a reducing agent and prevents damage of
hemoglobin- Enzymes - Carbonic anhydrase and
catalase
d)Ions - Na+, K+, Ca2+, PO43-
8.
PAGE -
7
FUNCTION:-
The most important function of an RBC is the transportation of
oxygen to tissues with the help of HbA present in normal adults.
Hemoglobin + oxygen = oxyhemoglobin
The 4 units of HbA take up oxygen in succession which results in
stepwise affinity of hemoglobin for oxygen and thus is responsible
for the sigmoid shape of the oxygen dissociation curve.
Another important function of RBC's is the transportation of CO2
from the tissues to the lungs.
Hemoglobin + carbon dioxide = carbhemoglobin
In determination of blood groups: Carries blood group antigens
like antigen A,B etc. that help in determination of blood groups &
enables to prevent reactions due to incompatable blood
transfusion
9.
PAGE - 8
DISORDERS OF RBC :-
Most erythrocyte disorders are classified as either anemia or
polycythemia
ANEMIA :
Anemia occurs when a person has a low number of
healthy RBCs. This may happen due to changes in the cell
itself or components of the cell, such as hemoglobin.
There are different types of anemia, each with its own
causes.
Symptoms : fatigue, pallor, dyspnea, and chills
Three groups based on cause
Blood loss
Not enough RBCs produced
Too many RBCs being destroyed
10.
PAGE - 9
POLYCYTHEMIA :-
Polycythemia, or erythrocytosis, is a condition in which the
body has an increased number of RBCs. The extra blood cells
can make the blood thicker and lead to difficulties with blood
flow, which can increase the risk of other health issues.
Polycythemia may be primary or secondary. Primary
polycythemia, called polycythemia vera, is a slow-growing type
of blood cancer. It will typically also cause an increase in white
blood cells and platelets. Secondary polycythemia, or
erythrocytosis, can result from factors -
such as:
smoking
steroid use
chronic oxygen deficiency in the
arteries
some types of tumors
11.
PAGE -
10
REFERENCES
1) SmithJE. Erythrocyte membrane: structure, function, and pathophysiology. Vet
Pathol. 1987 Nov;24(6):471-6. [PubMed]
2) Kuhn V, Diederich L, Keller TCS, Kramer CM, Lückstädt W, Panknin C, Suvorava T,
Isakson BE, Kelm M, Cortese-Krott MM. Red Blood Cell Function and Dysfunction:
Redox Regulation, Nitric Oxide Metabolism, Anemia. Antioxid Redox Signal. 2017
May 01;26(13):718-742. [PMC free article] [PubMed]
3) Adewoyin AS, Nwogoh B. Peripheral blood film - a review. Ann Ib Postgrad Med.
2014 Dec;12(2):71-9. [PMC free article] [PubMed]
4) Barcia JJ. The Giemsa stain: its history and applications. Int J Surg Pathol. 2007
Jul;15(3):292-6. [PubMed]
5) Ford J. Red blood cell morphology. Int J Lab Hematol. 2013 Jun;35(3):351-7.
[PubMed]
12.
PAGE -
11
6) TsukitaS, Tsukita S, Ishikawa H, Sato S, Nakao M. Electron microscopic study of
reassociation of spectrin and actin with the human erythrocyte membrane. J Cell
Biol. 1981 Jul;90(1):70-7. [PMC free article] [PubMed]
7) Schnitzer B, Rucknagel DL, Spencer HH, Aikawa M. Erythrocytes: pits and
vacuoles as seen with transmission and scanning electron microscopy. Science.
1971 Jul 16;173(3993):251-2. [PubMed]
8) Pretorius E, Olumuyiwa-Akeredolu OO, Mbotwe S, Bester J. Erythrocytes and their
role as health indicator: Using structure in a patient-orientated precision
medicine approach. Blood Rev. 2016 Jul;30(4):263-74. [PubMed]
9) Azar S, Wong TE. Sickle Cell Disease: A Brief Update. Med Clin North Am. 2017
Mar;101(2):375-393. [PubMed]
10)Lynch EC. Peripheral Blood Smear. In: Walker HK, Hall WD, Hurst JW, editors.
Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd ed.
Butterworths; Boston: 1990. [PubMed]

![PAGE -
10
REFERENCES
1) Smith JE. Erythrocyte membrane: structure, function, and pathophysiology. Vet
Pathol. 1987 Nov;24(6):471-6. [PubMed]
2) Kuhn V, Diederich L, Keller TCS, Kramer CM, Lückstädt W, Panknin C, Suvorava T,
Isakson BE, Kelm M, Cortese-Krott MM. Red Blood Cell Function and Dysfunction:
Redox Regulation, Nitric Oxide Metabolism, Anemia. Antioxid Redox Signal. 2017
May 01;26(13):718-742. [PMC free article] [PubMed]
3) Adewoyin AS, Nwogoh B. Peripheral blood film - a review. Ann Ib Postgrad Med.
2014 Dec;12(2):71-9. [PMC free article] [PubMed]
4) Barcia JJ. The Giemsa stain: its history and applications. Int J Surg Pathol. 2007
Jul;15(3):292-6. [PubMed]
5) Ford J. Red blood cell morphology. Int J Lab Hematol. 2013 Jun;35(3):351-7.
[PubMed]](https://image.slidesharecdn.com/asimkumarjanarbcroll21seca-250903135230-159c1544/85/ASIM-KUMAR-JANA-RBC-bbbbbbbbb-SEC-A-pptx-11-320.jpg)
![PAGE -
11
6) Tsukita S, Tsukita S, Ishikawa H, Sato S, Nakao M. Electron microscopic study of
reassociation of spectrin and actin with the human erythrocyte membrane. J Cell
Biol. 1981 Jul;90(1):70-7. [PMC free article] [PubMed]
7) Schnitzer B, Rucknagel DL, Spencer HH, Aikawa M. Erythrocytes: pits and
vacuoles as seen with transmission and scanning electron microscopy. Science.
1971 Jul 16;173(3993):251-2. [PubMed]
8) Pretorius E, Olumuyiwa-Akeredolu OO, Mbotwe S, Bester J. Erythrocytes and their
role as health indicator: Using structure in a patient-orientated precision
medicine approach. Blood Rev. 2016 Jul;30(4):263-74. [PubMed]
9) Azar S, Wong TE. Sickle Cell Disease: A Brief Update. Med Clin North Am. 2017
Mar;101(2):375-393. [PubMed]
10)Lynch EC. Peripheral Blood Smear. In: Walker HK, Hall WD, Hurst JW, editors.
Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd ed.
Butterworths; Boston: 1990. [PubMed]](https://image.slidesharecdn.com/asimkumarjanarbcroll21seca-250903135230-159c1544/85/ASIM-KUMAR-JANA-RBC-bbbbbbbbb-SEC-A-pptx-12-320.jpg)















































