UKZN INSPIRING GREATNESS
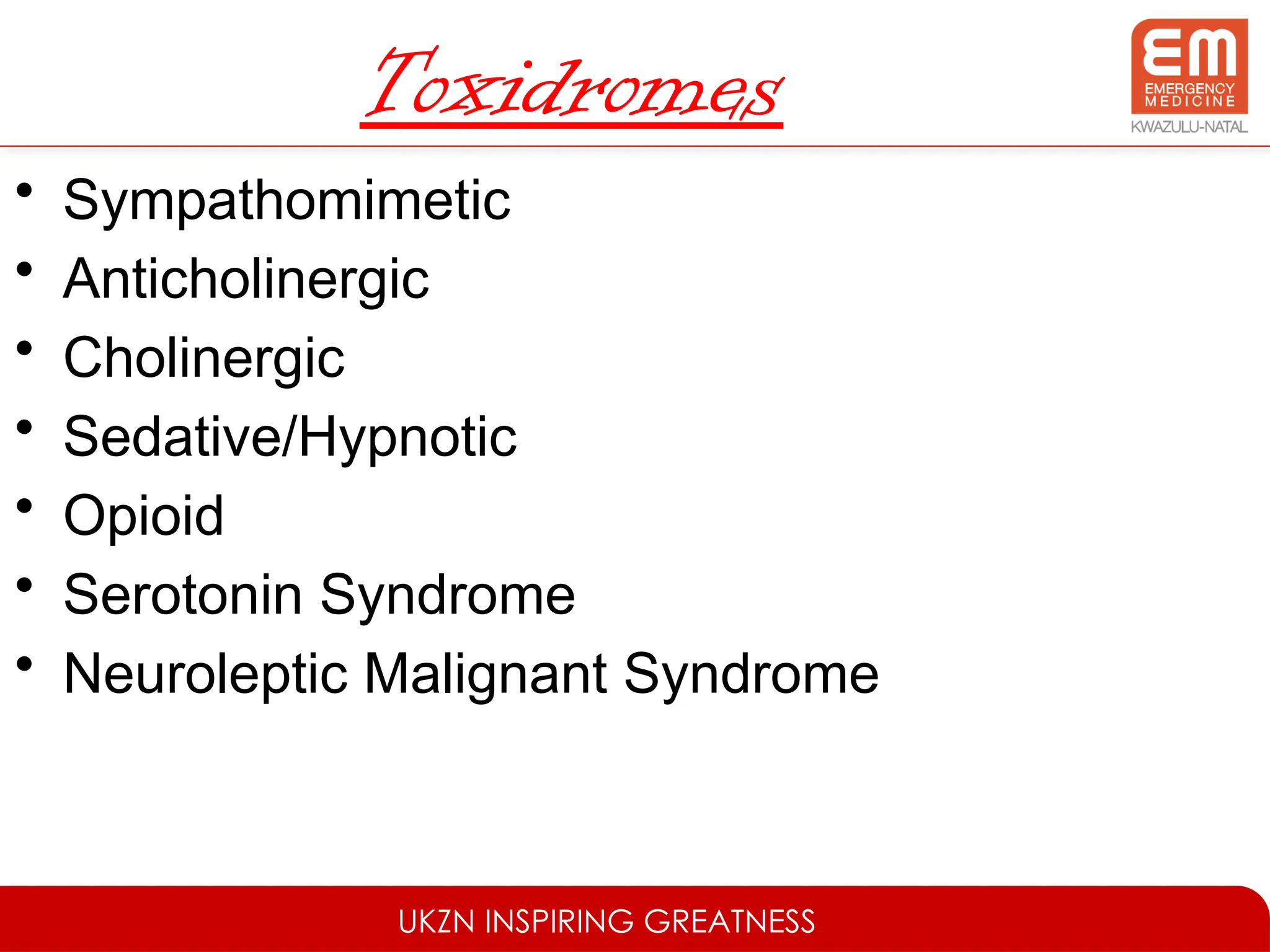
Anti-cholinergicToxidrome
Mad as a Hatter - Confusion
Red as a beet - Flushed
Hot as a Hare - Hyperthermia
Blind as a Bat - Mydiasis
Dry as a Bone – Dry skin
http://www.thegasmanhandbook.co.uk/toxidromes.html
UKZN INSPIRING GREATNESS
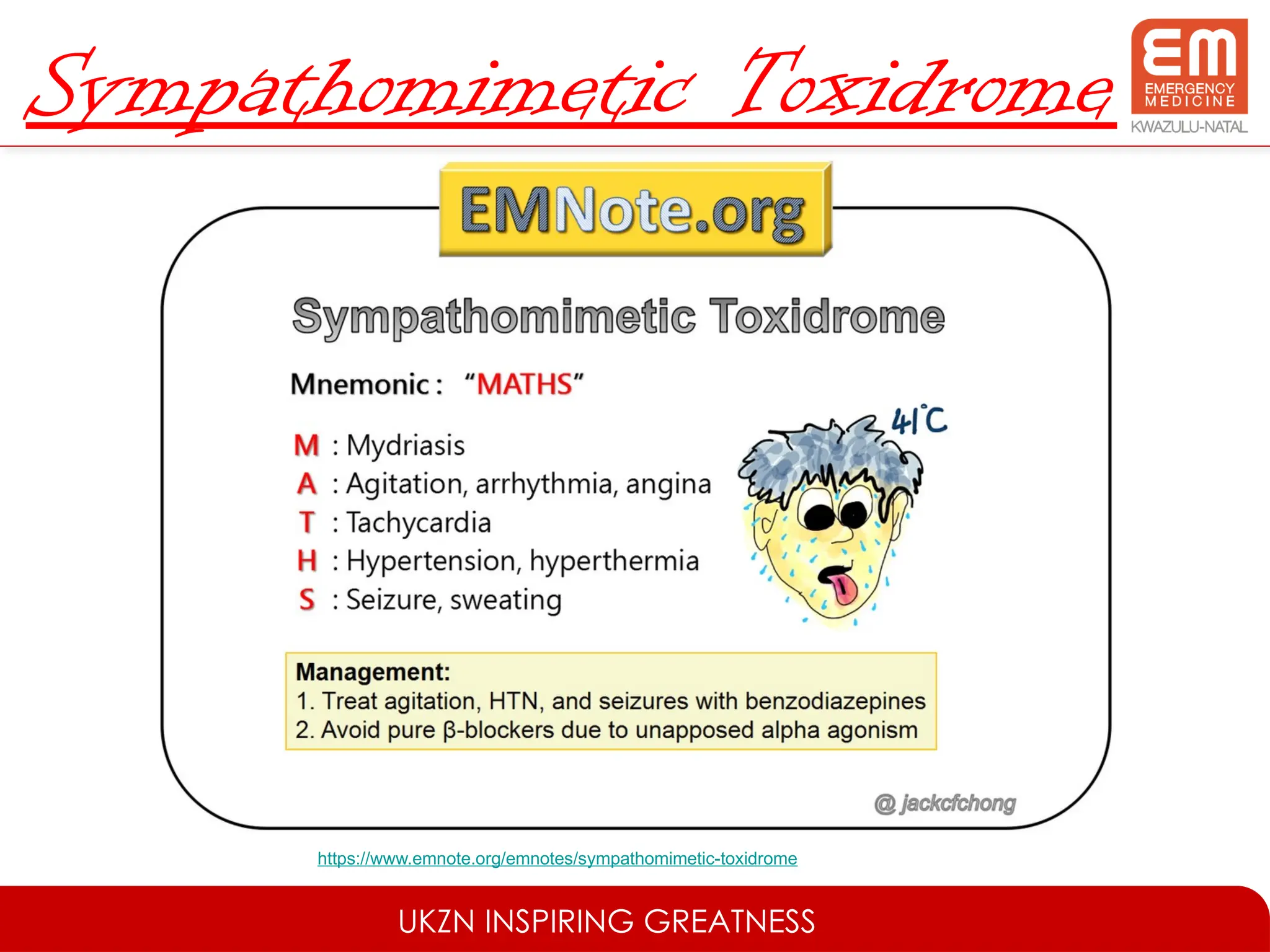
SerotoninSyndrome
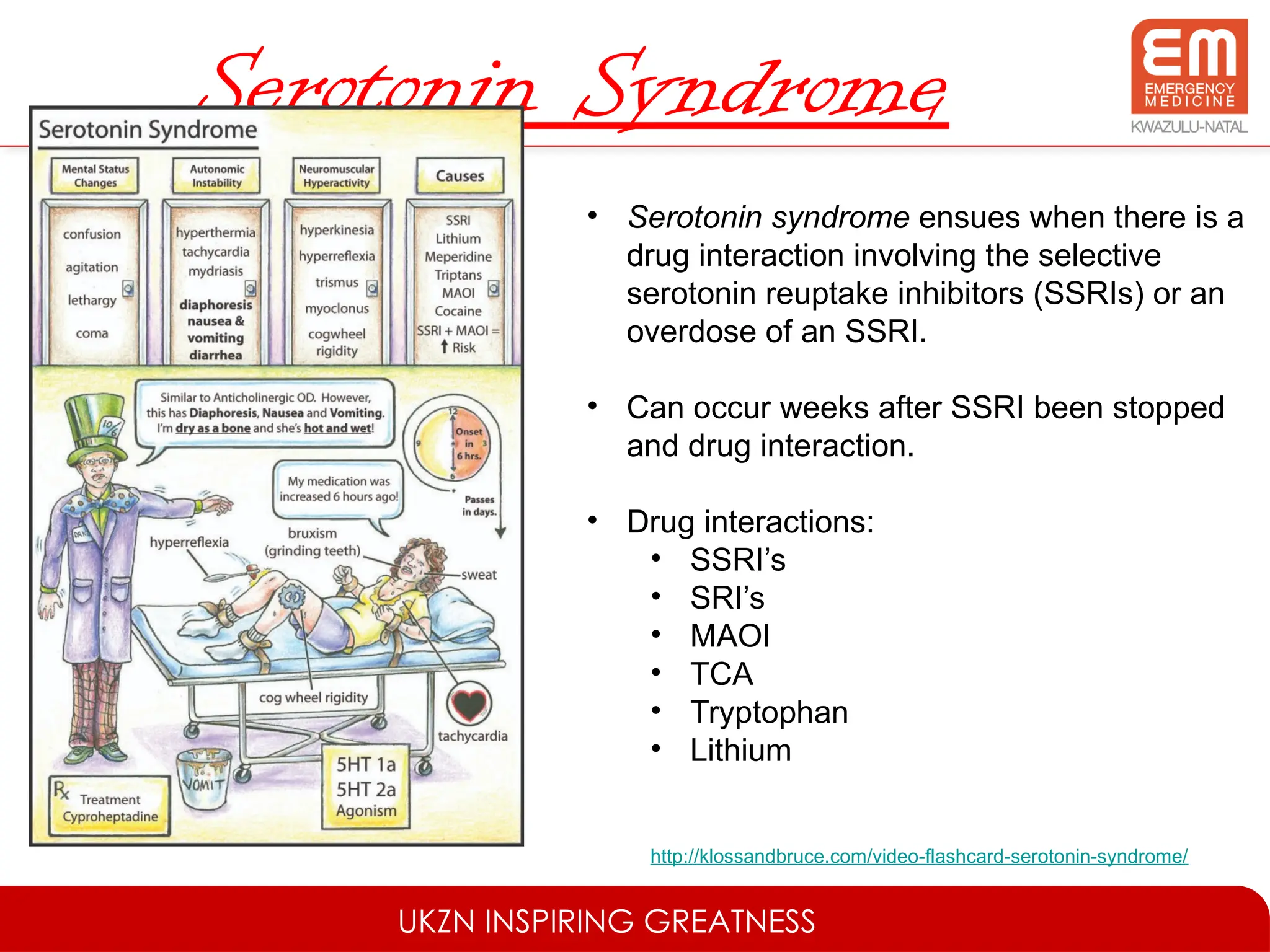
• Serotonin syndrome ensues when there is a
drug interaction involving the selective
serotonin reuptake inhibitors (SSRIs) or an
overdose of an SSRI.
• Can occur weeks after SSRI been stopped
and drug interaction.
• Drug interactions:
• SSRI’s
• SRI’s
• MAOI
• TCA
• Tryptophan
• Lithium
http://klossandbruce.com/video-flashcard-serotonin-syndrome/
UKZN INSPIRING GREATNESS
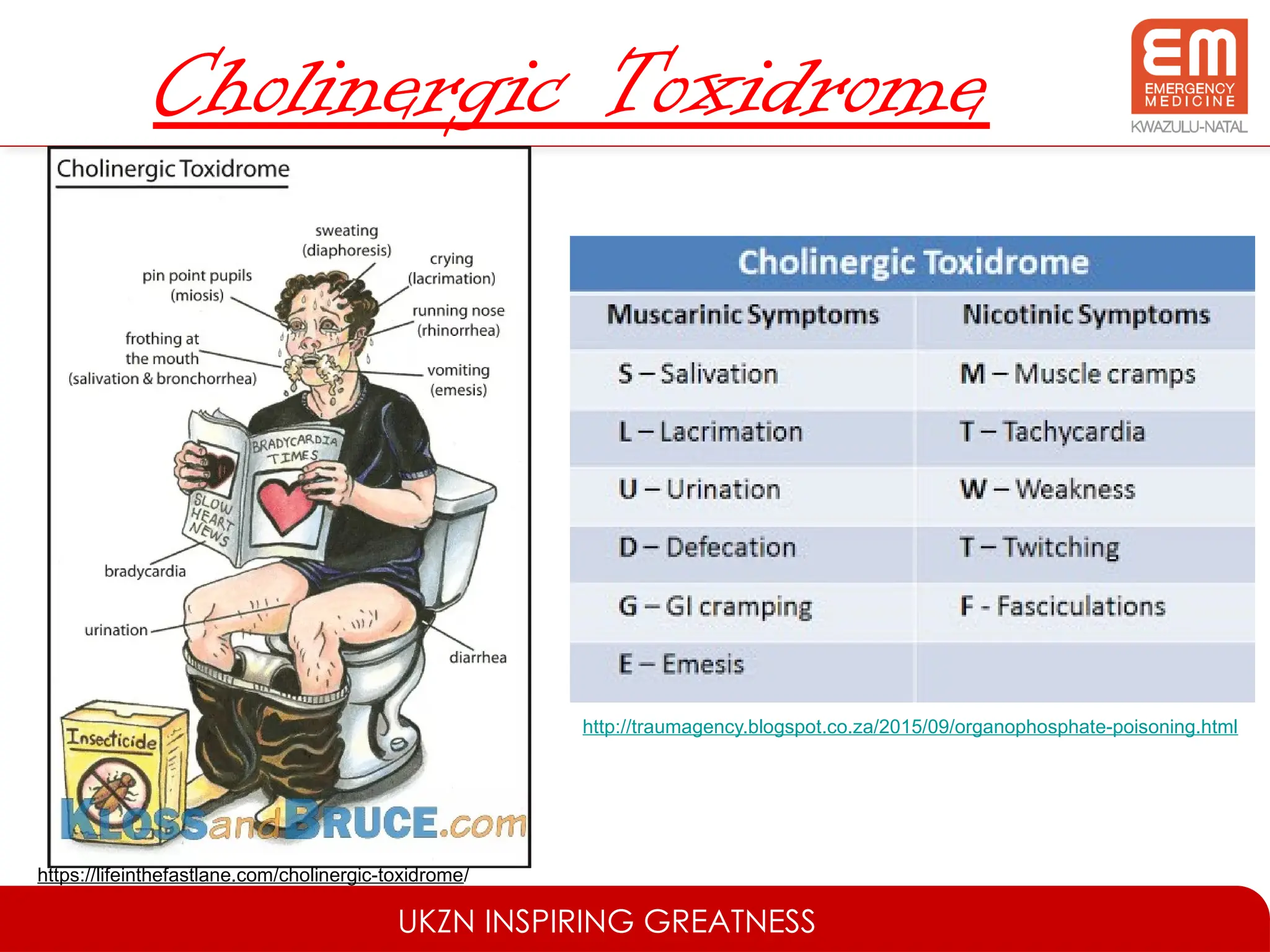
RiskAssessment
• A distinct cognitive step that is quantitative in
nature and takes into account:
– Agent(s)
– Dose(s)
– Time since ingestion
– Current clinical status
– Patient factors
https://www.cartoonstock.com/directory/d/dieting_pill.asp
UKZN INSPIRING GREATNESS
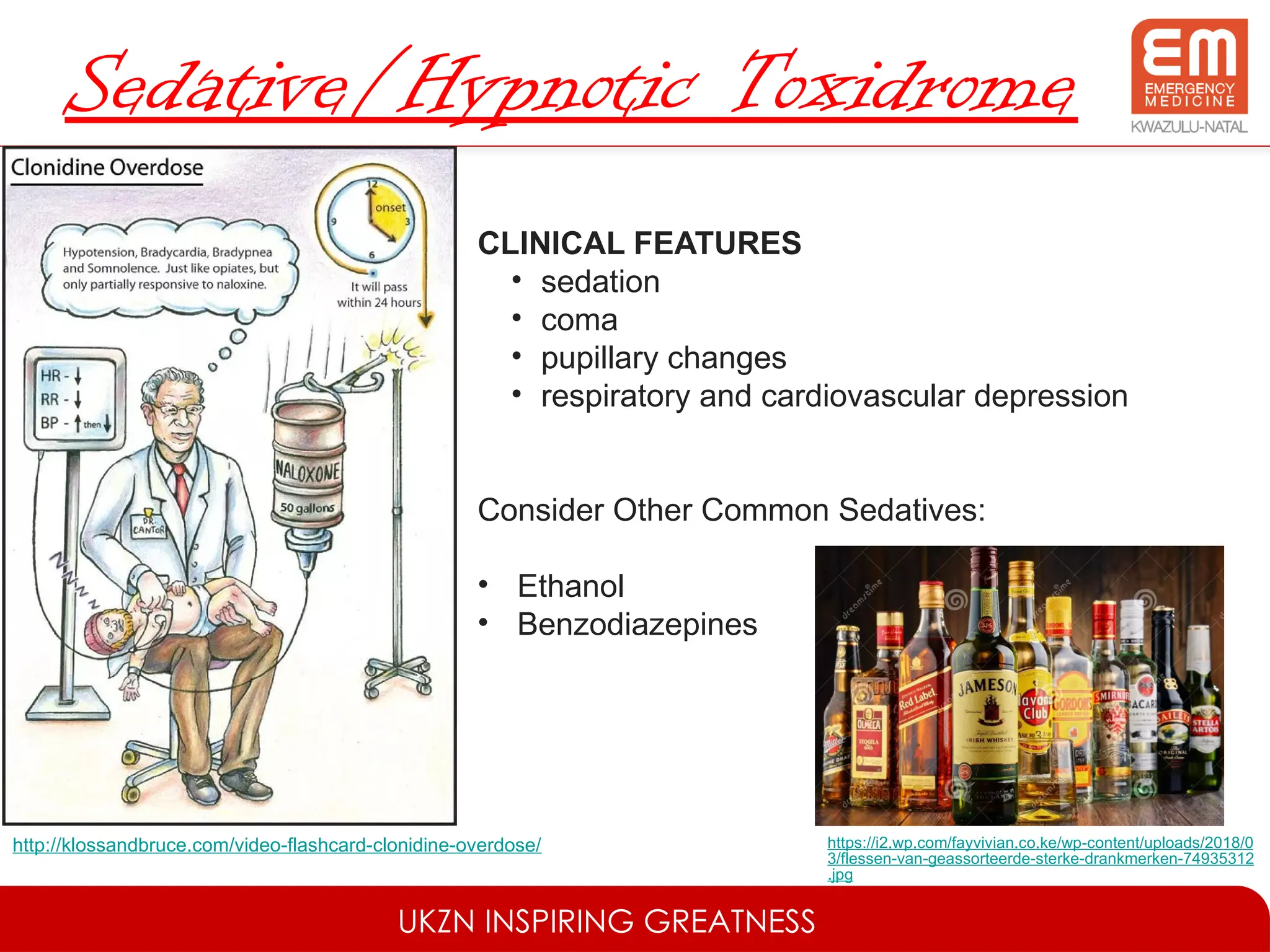
SupportiveCare & Monitoring
• FAST HUGS IN BED Please
• Fluid therapy and feeding
• Analgesia, antiemetics
• Sedation and Spontaneous breathing trial
• Thromboprophylaxis
• Head up position (30 degrees) if intubated
• Ulcer prophylaxis
• Glucose control
• Skin/ eye care and suctioning
17.
UKZN INSPIRING GREATNESS
SupportiveCare & Monitoring
• Indwelling catheter
• Nasogastric tube
• Bowel cares
• Environment (e.g. temperature control, appropriate surroundings in delirium)
• De-escalation (e.g. end of life issues, treatments no longer needed)
• Psychosocial support (for patient, family and staff)
http://www.movingbrands.com/work/red-cross
UKZN INSPIRING GREATNESS
Decontamination
•Decontamination is the process of preventing
systemic absorption into the body.
– Ocular & Dermal exposure = irrigate with water.
– Syrup of Ipecac – inducing emesis
– Gastric Lavage
– Whole Bowel Irrigation
http://bryanking.net/syrup-of-ipecac/
23.
UKZN INSPIRING GREATNESS
Decontamination
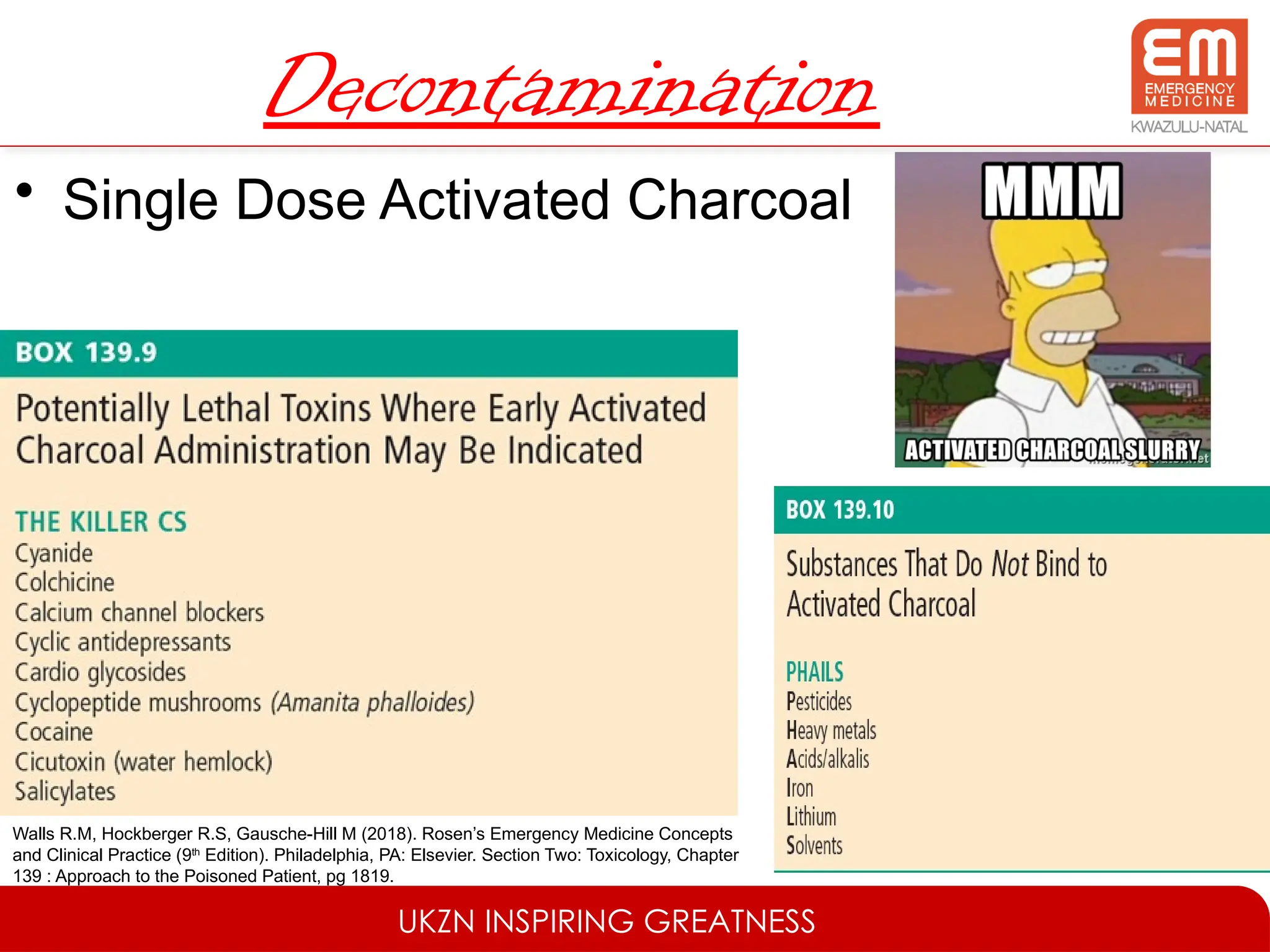
•Single Dose Activated Charcoal
Walls R.M, Hockberger R.S, Gausche-Hill M (2018). Rosen’s Emergency Medicine Concepts
and Clinical Practice (9th
Edition). Philadelphia, PA: Elsevier. Section Two: Toxicology, Chapter
139 : Approach to the Poisoned Patient, pg 1819.
UKZN INSPIRING GREATNESS
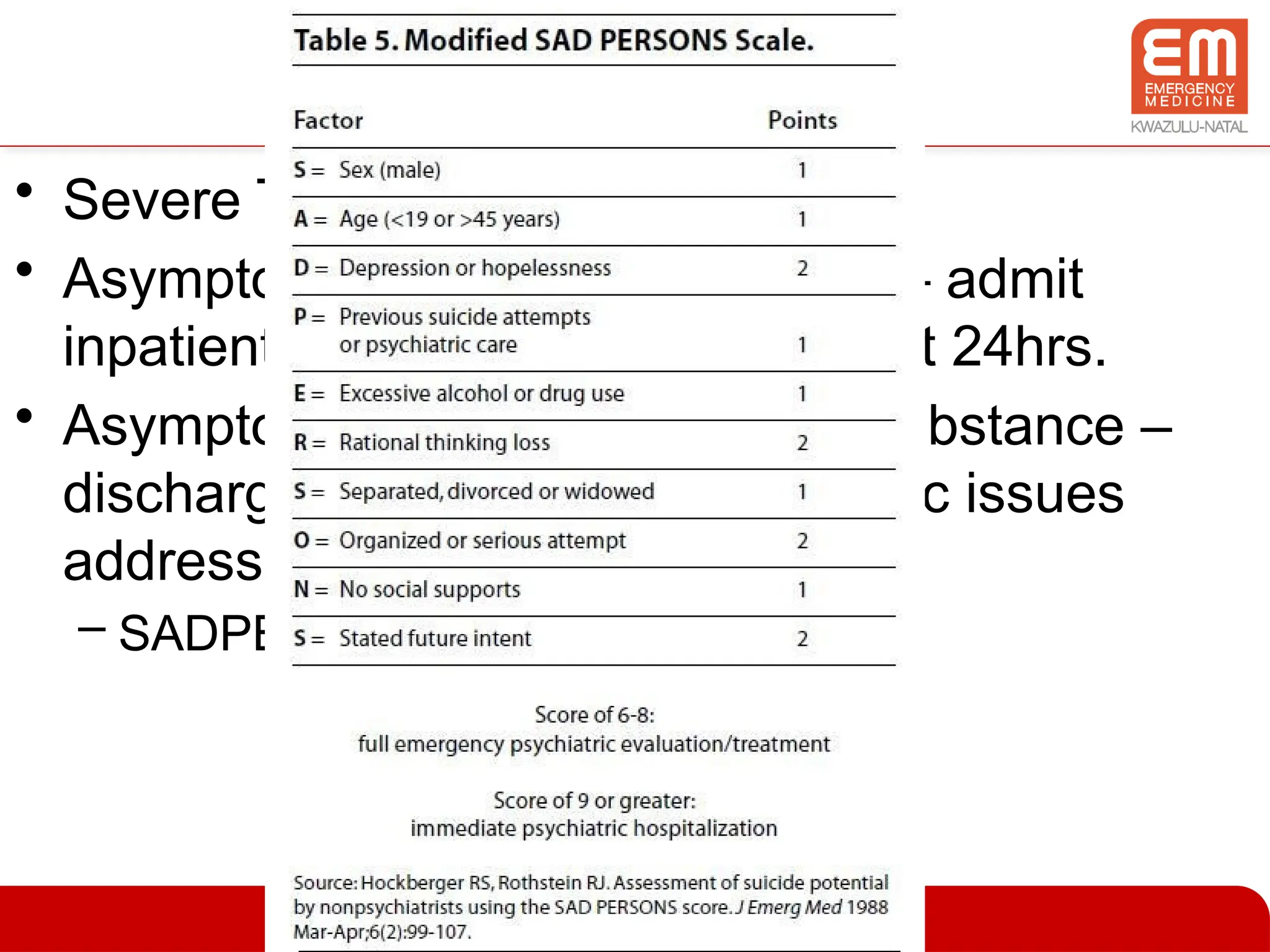
Disposition
•Severe Toxicity – ICU/High Care
• Asymptomatic but toxic ingestion – admit
inpatient setting or observation unit 24hrs.
• Asymptomatic & minimally toxic substance –
discharge from ED once psychiatric issues
addressed.
– SADPERSONS score
34.
UKZN INSPIRING GREATNESS
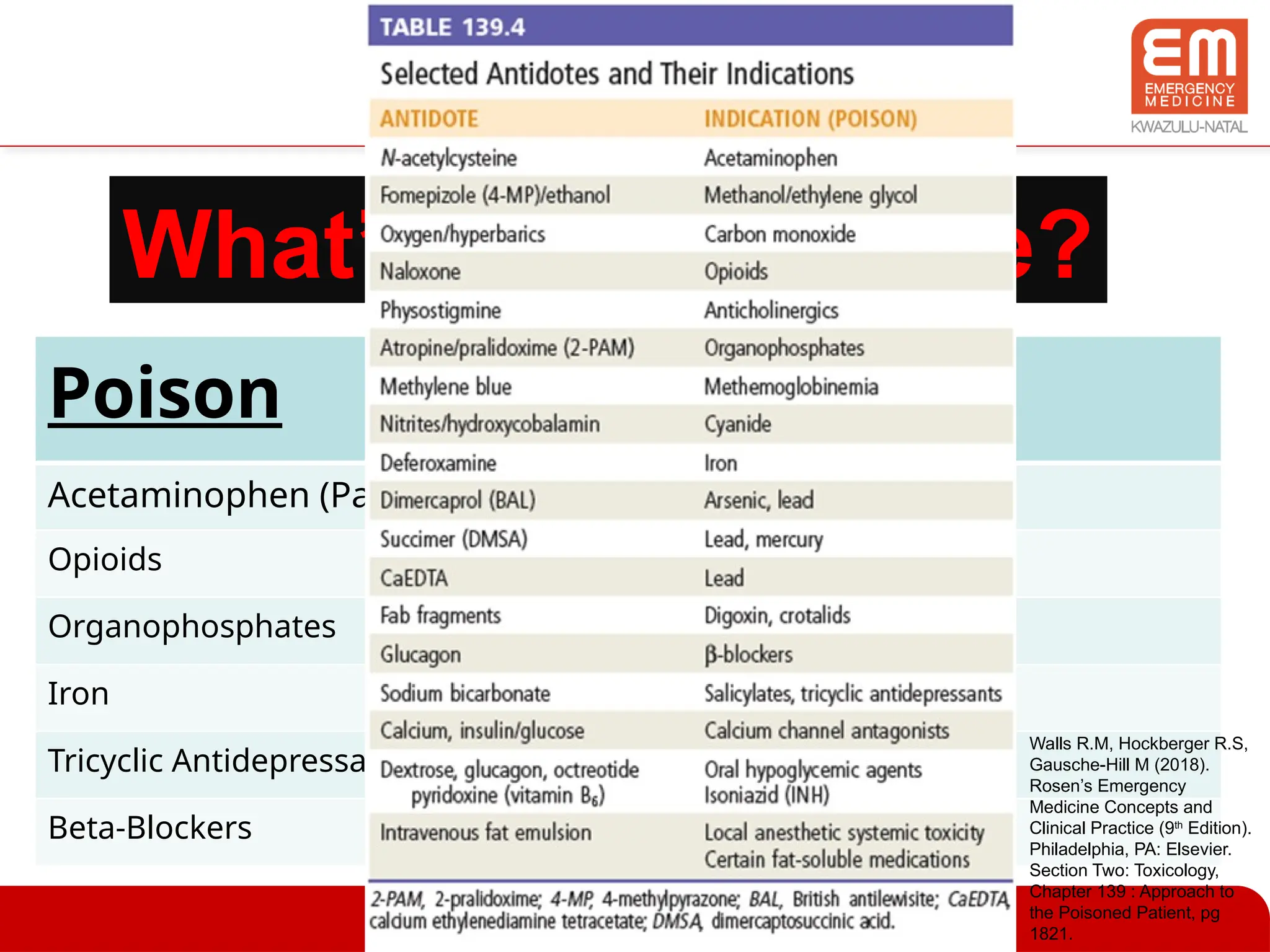
References
•Walls R.M, Hockberger R.S, Gausche-Hill M (2018). Rosen’s
Emergency Medicine Concepts and Clinical Practice (9th
Edition). Philadelphia, PA: Elsevier. Section Two: Toxicology,
Chapter 139 : Approach to the Poisoned Patient, pg 1813-1822.
• Chris Nickson. Approach to Acute Poisoning. Life in the Fast
Lane. May 2016. Available from URL:
https://lifeinthefastlane.com/ccc/approach-to-acute-poisoning/
• Images Referenced on Slides
Editor's Notes
#4 Personal and Protective equipment.
Decontamination if on-going exposure to toxin.
#7 Parkinson's medications.
diphenhydramine (Benadryl)
trihexyphenidyl
benztropine mesylate
biperiden (Akineton)
antipsychotics.
clomipramine
chlorpromazine
Atropine
Other common manifestations include:
urinary retention,
sinus tachycardia,
reduced GI motility,
tremor,
hypertension
#8 Organophosphates
carbamate insecticides
Physostigmine
Edrophonium
Mushrooms
sarin nerve gas
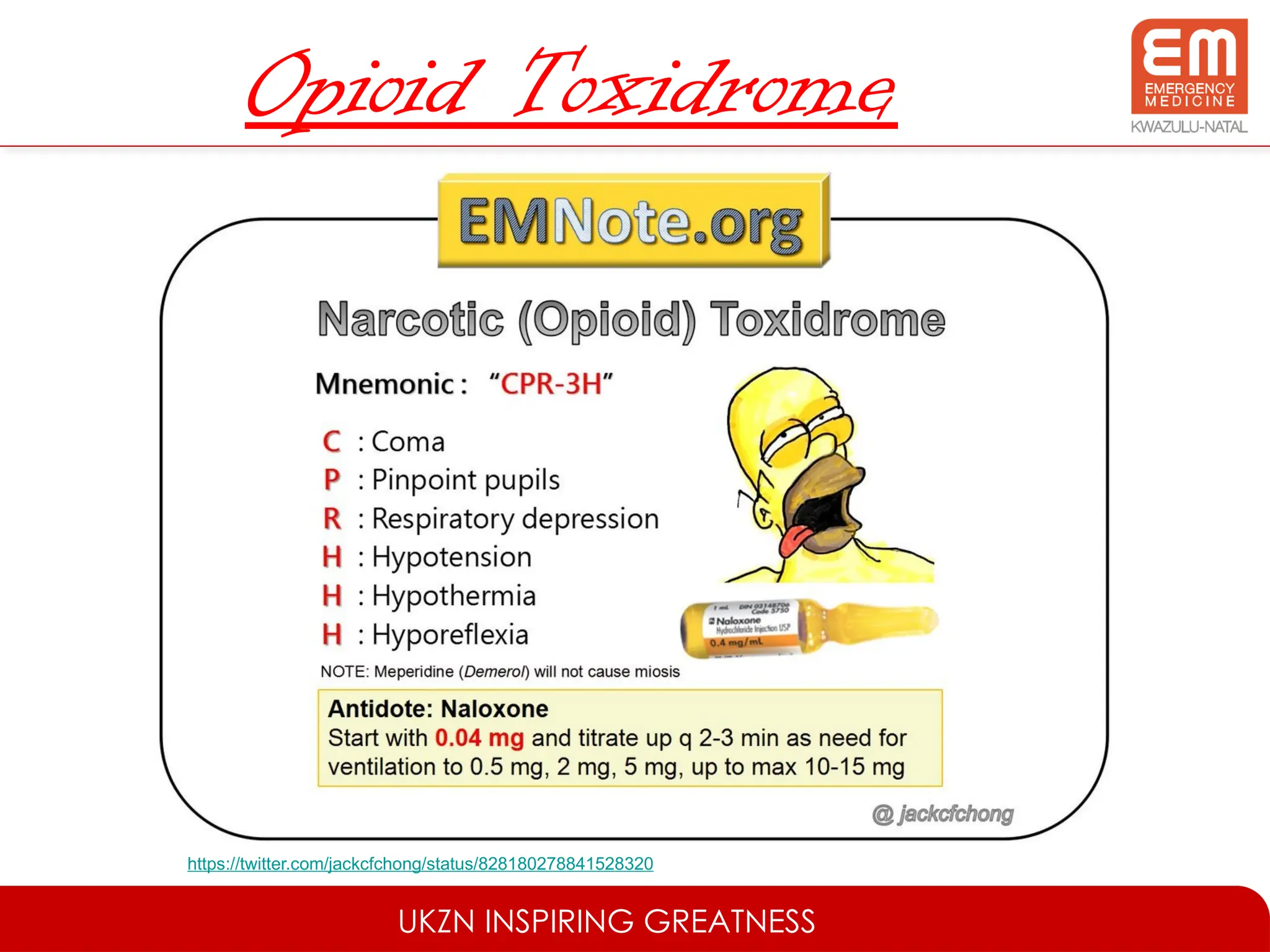
#9 Opioids
Benzodiazepines
Barbiturates
baclofen (may mimic brain death, suspect in MS patients)
clonidine (mimics opioid toxidrome with marked bradycardia and hypotension)
#11 Serotonin syndrome ensues when there is a drug interaction involving the selective serotonin reuptake inhibitors (SSRIs) or an overdose of an SSRI.
Fluoxetine (Prozac),
Sertraline (Zoloft),
paroxetine (Paxil),
fluvoxamine (Luvox),
and citalopram (Celexa) are commonly used SSRIs.
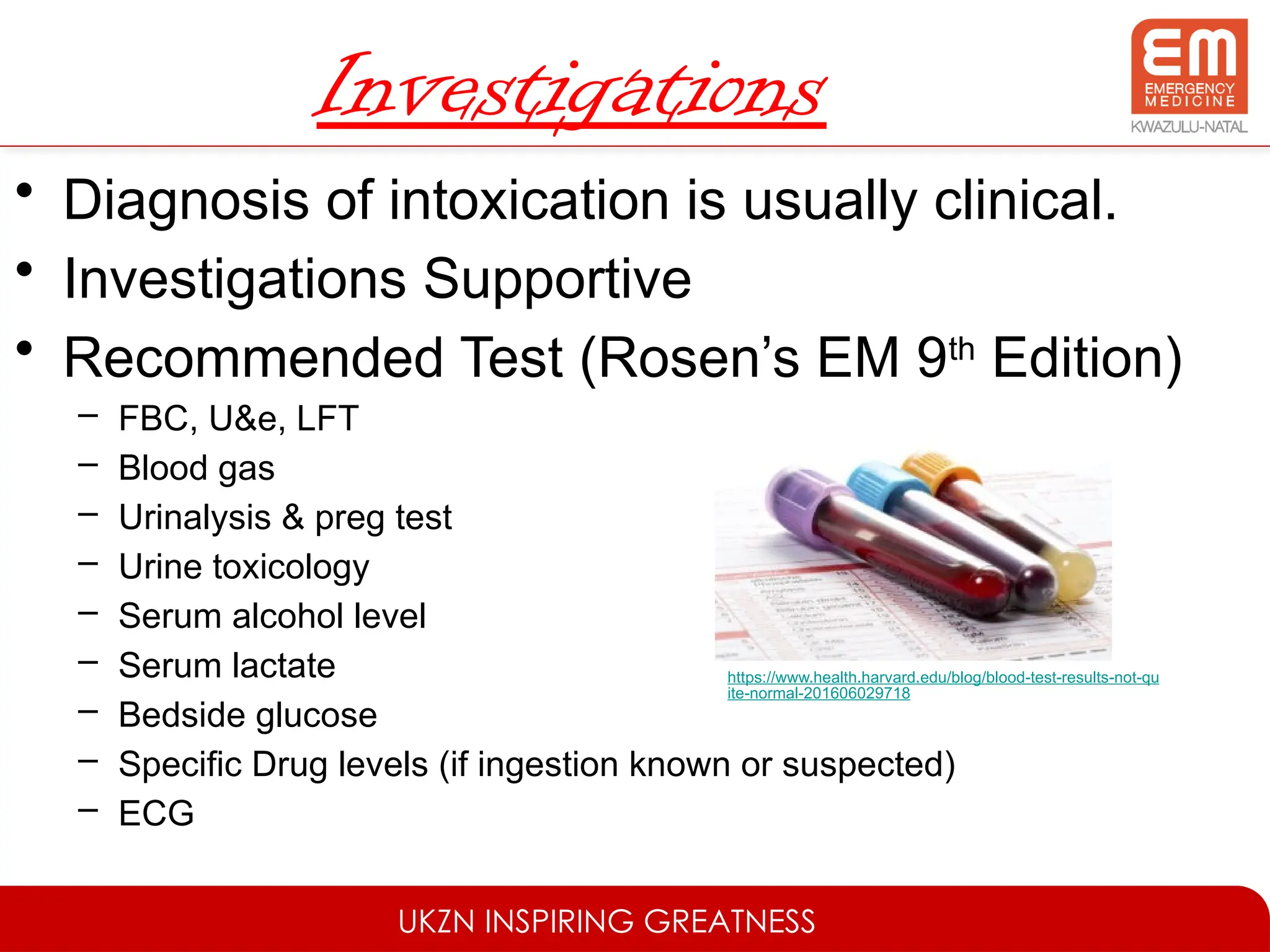
#19 Understand Limitations of Toxicology Screens
Serum Toxicology screens can give false negatives, if drug short half life and blood not taken early enough.
Urine toxicology screens more reliable – longer period detection – qualitative and not quantitative therefore can have false positives.
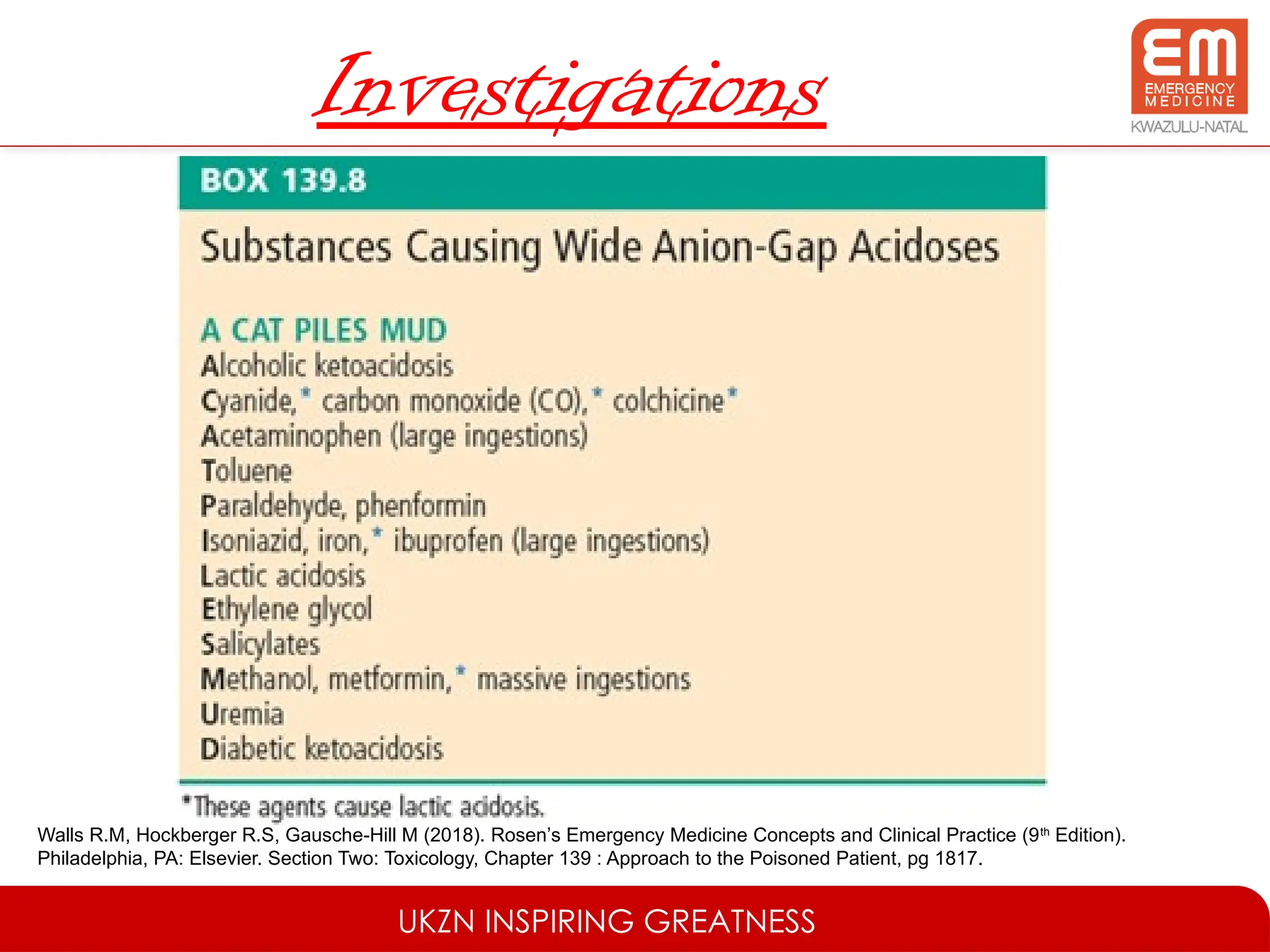
#20 Blood gas can aid in the differential diagnosis, especially with calculating the anion gap.
#22 Ocular & Dermal exposure = removal of contaminated clothes and irrigate with water.
Syrup of Ipecac – inducing emesis – Not indicated in the treatment of the poisoned patient in the ED
Gastric Lavage – only if within 1 hour of ingestion and only if no antidote exists for ingested drug, so poor prognosis if drug absorped.
Whole Bowel Irrigation with Polyethylene Glycol indicated only in certain conditions, extended release preparations, illicit drug packets or metals (iron and lead)
#23 Single dose activated charcoal
Administer within 1 hour of ingestion toxin
Awake and alert patient
Toxin ingested – high toxicity or massive amounts ingested
Not recommended use due to lack of evidence in clinical benefit (very few appropriate designed trials)
Risk Aspiration – low risk but if occurs poor prognosis.
Bowel Obstruction - Contraindicated
Activated charcoal historically has most often been given in a dose of 25 to 100 grams (10 to 25 grams or 0.5 to 1.0 gram/kilogram in young children).
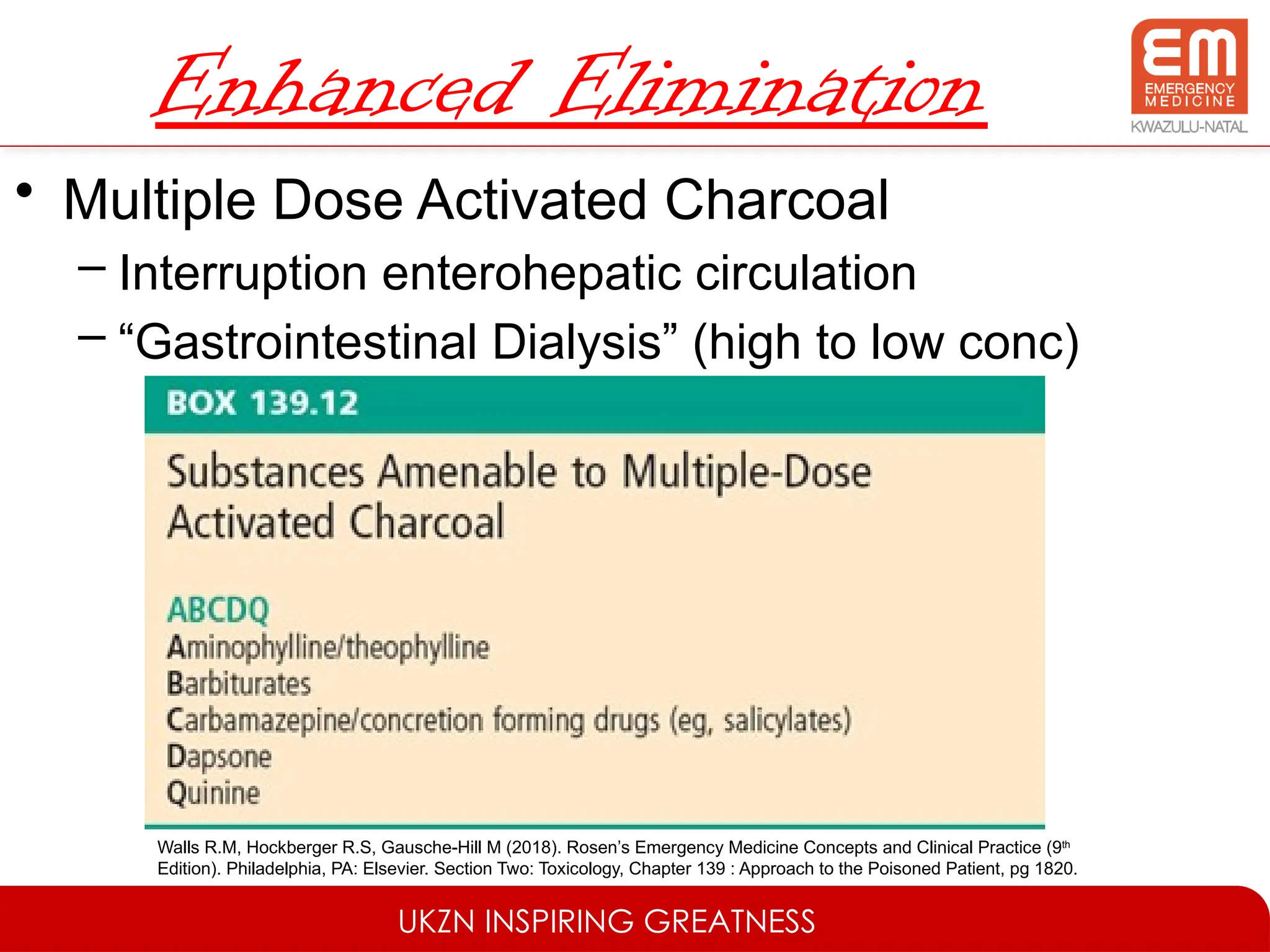
#26 MDAC facilitates removal toxin that already absorbed – interruption of enterohepatic circulation & Gastrointestinal dialysis (High concentration of drug in the gut wall microcirculation and low concentration in gut lumen filled with charcoal and therefore drug moves down concentration gradient).
When MDAC is indicated, the initial loading dose of an activated charcoal–to-xenobiotic ratio of 10 : 1, is followed by subsequent doses of 50% of the initial dose every 4 to 6 hours for up to 24 hours. MDAC may be discontinued when the patient’s measureable serum levels are no longer considered in the toxic range.
MDAC caution aspiration and Bowel Obstruction.
#27 Certain water-soluble ingestants such as salicylates, methotrexate, and phenobarbital will undergo ion-trapping and enhanced urinary elimination if the serum is sufficiently alkalinized.
Salicylates alkalinisation will also prevent crossing of BBB.
Goal serum pH 7.5 and urine pH 8
Combine 150 mEq (3amps) of 8.4% sodium bicarbonate into a litre of dextrose 5% in water (D5W) and add potassium @250ml/hr.
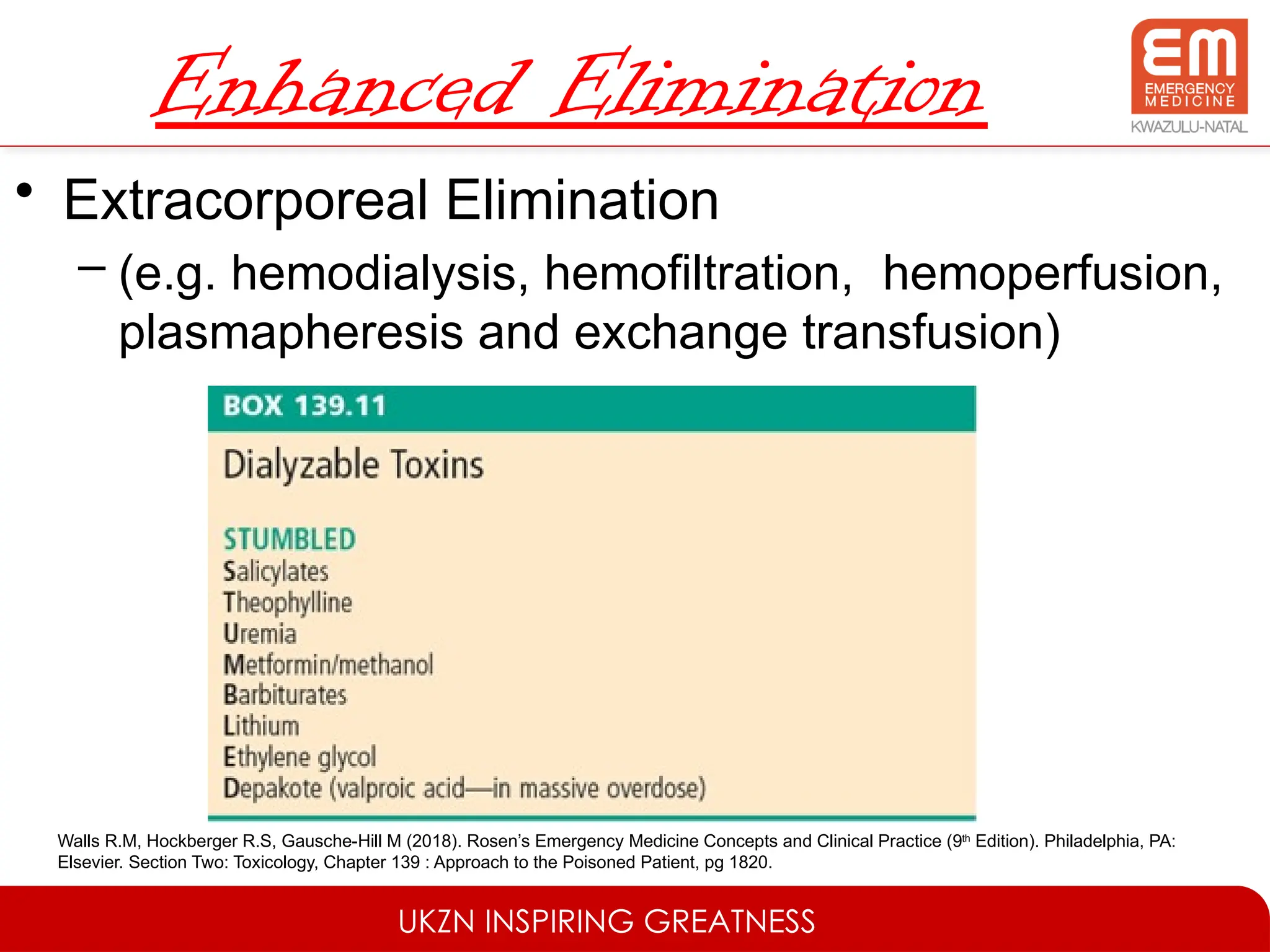
#28 Hemodialysis effectively enhances elimination of any drug that:
is a small molecule
has a small volume of distribution
rapid redistribution from tissues and plasma
slow endogenous elimination.
#29 The lipid sink theory posits that fat-soluble drugs are soaked up and removed from the site of toxicity, effectively increasing the volume of distribution for a fat-soluble drug. This is the predominant theory behind the use of IFE. A second theory involves optimization of cardiac metabolism. The heart under physiologic circumstances prefers free fatty acids; in times of stress, it switches to glucose metabolism for energy. A dose of IFE theoretically provides a large supply of free fatty acids to optimize energy use in the heart. In addition to providing supplemental energy for myocytes, IFE may also enhance activation of cardiac calcium channels.