FDG PET/CT Utility in Gynecologic Malignancies
•
3 likes•1,301 views

A comprehensive review of anatomy, pathways of metastatic spread and scan findings

Recommended
More Related Content
What's hot
What's hot (19)
Similar to FDG PET/CT Utility in Gynecologic Malignancies
Similar to FDG PET/CT Utility in Gynecologic Malignancies (20)
FDG PET/CT Utility in Gynecologic Malignancies
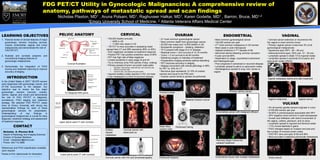
- 1. FDG PET/CT Utility in Gynecologic Malignancies: A comprehensive review of anatomy, pathways of metastatic spread and scan findings Nicholas Plaxton, MD1 , Aruna Polsani, MD1, Raghuveer Halkar, MD1, Karen Godette, MD1 , Barron, Bruce, MD1,2 1Emory University School of Medicine, 2 Atlanta Veterans Affairs Medical Center LEARNING OBJECTIVES PELVIC ANATOMY CERVICAL OVARIAN ENDOMETRIAL VAGINAL Uterine fundus • 150,000 Deaths annually • 2nd most common gynecological cancer 1. Pictorial review of clinical features of major • Most common gynecological cancer • Cervical cancer extension or recurrence into Fallopian tube 4000 in US • Most common death from gynecologic cancer gynecologic cancers including cervical, • 142,000 women per year the vagina is most common tumor ovarian, endometrial, vaginal, and vulvar Infundibulum Fimbria 11,000 new cases in US • 22,000 new cases and 14,000 deaths in US • 4TH most common malignancy in US women • Primary vaginal cancer is less than 3% of all Ovary • PET/CT is more accurate in assessing nodal • Nonspecific symptoms – bloating, distention malignancies and demonstrate the role of Uterine Body • Most cases in post menopause gynecological malignancies Ascending branch of uterine artery spread than CT and MRI (sensitivity 89% vs 39%) • 75 % present with stage III or IV disease FDG PET/CT. Internal iliac • Highest incidence in 7TH decade of life • Squamous type (HPV , 60 – 80 yrs) artery • SUV negatively correlates to treatment response • Residual tumor > 2cm survival of 12-16 months • Abnormal uterine bleeding common symptom • Adenocarcinoma type ( DES use, 12 – 30 yrs) Cervix Uterine artery External Os • Positive PET has positive predictive value of 90% • Tumor < 2 cm survival is 40-45 months 2. Illustrate and correlate anatomic and Vaginal branch of uterine artery • 5 year survival 80% • Lymphatic spread in distal 1/3 to inguinal nodes Vaginal canal • PET has high rate of false negatives • Debulking surgery is mainstay of treatment conventional imaging features of • Dependent on stage, myometrial involvement • Lymphatic spread in proximal 2/3 to pelvic and • Limited sensitivity in early stage IA and IIA • Preoperative imaging achieves optimal debulking gynecologic malignancies. and histological type para-arotic nodes (PALN) • Try to minimize urine FDG activity (Foley, voiding) • PET improves accuracy in staging Coronal Illustration • Poor prognosis in advanced or recurrent disease • Primary spread of tumor via lymph node paths • Staging concordant with clinical pathology in 69% 3. Demonstrate the integration of FIGO 1. obturator, internal iliac, external iliac, and common iliac • Lymphatic spread to pelvic or para-arotic nodes scoring and treatment planning to improve 2. direct to common iliac for PET vs. 53% for CT • Hematogenous spread to lung, liver, bones or accuracy of staging. 3. common iliac, pre-sacral and para-arotic • Mucinous type represents 12-15% of ovarian vagina Perimetrium • Inguinal /axillary nodes reactive in HIV, not mets cancers and usual is not FDG avid INTRODUCTION Myometrium Rectouterine pouch • Liver metastasis in a third of recurrent disease • Ovarian cancer tends to spread via peritoneal Vaginal metastasis before and after treatment Cervix of Douglas In the United States in 2007,* 80,976 women Fundus Endometrium Body were diagnosed with gynecologic cancer, and 27,739 succumbed to the disease. Our Vesicouterine pouch of Meiring objective was to review the five major gynecologic cancers (cervical, ovarian, Primary uterine cancer T2 Weighted MRI pelvis Virchow’s Node uterine, vaginal, and vulvar) and demonstrate the role of FDG PET/CT in diagnosis, surveillance, FIGO staging and treatment Cervical cancer with pyometra Bilateral Ovarian Cancer Vaginal melanoma Vaginal cancer strategy. We selected FDG PET/CT cases done at Emory University with strong key Right ovary with cysts Left ovary VULVAR Internal iliac artery • 4% all women genital cancers originate in vulva Right internal representative findings for each of these iliac artery Left iliacus muscle gynecological cancers for presentation. • 2/100,000 women per year Psoas muscle Endometrial cancer with malignant effusion • 40-60% in premenopause associated with HPV Understanding of key findings in gynecological malignancies is crucial for early • HPV negative more common in post-menopausal diagnosis, treatment strategy and assessment • Growth and infiltration with direct involvement of of treatment response. the vagina, urethra, perineum, and /or anus Upper pelvis axial CT with contrast • Lymphatic spread to inguinal and femoral nodes CONTACT Sister Mary Peritoneal Caking • 1-7% involve Bartholin’s gland Solitary Cervical cancer with Joseph node • FIGO changes based on invasion and size and Nicholas A. Plaxton M.D. hepatic obstructed os the number of involved lymph nodes Depart of Radiology and Imaging Sciences External iliac artery metastasis • FDG PET sens and spec of 80 and 90% Division of Nuclear Medicine • More accurate in detecting extranodal metastases Round ligaments Email: nickplaxton@emory.edu Planning Target Volume for Phone: 404 712 4868 External iliac vein radiation treatment Bladder References and FIGO classification available Uterus upon request. Thanks to Eric Jablonowski for illustration. Lower pelvis axial CT with contrast Poster Design & Printing by Genigraphics® - 800.790.4001 Cervical cancer with HIV and lymphadenapathy Peritoneal Implants Endometrial cancer with multiple metastases Vulvar cancer