
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Lecture 1 Pathology: Cervix pdf
Similar to Lecture 1 Pathology: Cervix pdf (20)
Recently uploaded
Recently uploaded (20)
Lecture 1 Pathology: Cervix pdf
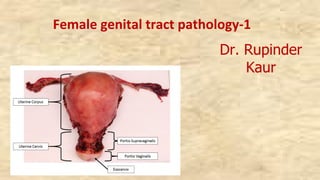
- 1. Female genital tract pathology-1 Dr. Rupinder Kaur
- 2. At the end of this session medical student should be able to: ►Discuss the etiology and morphological features of cervicitis. ► Discuss the epidemiology of carcinoma cervix ► Enumerate the etiological factors for the development of carcinoma cervix. ►Describe the pathogenesis of carcinoma cervix. ►Describe the progression of carcinoma cervix. ►Discuss the pathological features of carcinoma cervix ►Discuss the methods of diagnosis of carcinoma of cervix. ►Enumerate and discuss various screening methods and programs for early detection of carcinoma cervix
- 5. v The endocervix is lined by a simple columnar epithelium that secretes mucus. v Mucinous columnar epithelium lines the surface and the underlying glands v The ectocervix is covered by non-keratinizing, stratified squamous epithelium, either native or metaplastic in continuity with the vaginal epithelium. v The squamous epithelium is composed by multiple layers: basal, parabasal, intermediate and superficial layer
- 6. Cervix ►It is both a sentinel for potentially serious upper genital tract infections and a target for viruses and other carcinogens, which may lead to invasive carcinoma ►Regular Pap smears have proved beneficial in detecting cancer at the early stage with increase in the survival ►Pathology v Metaplasia, Inflammatory (Cervicitis) v Cervical neoplasia: Benign ( Polyps, Microglandular hyperplasia) ; Malignant
- 7. Cervicitis ►Inflammation commonly due to constant exposure to vaginal bacteria ►Found in almost all reproductive as well as post menopausal females ►Etiological agent: Streptococcus, HSV-2, staphylococcus, Chlamydia trachomatis (50- 75%), Neisseria gonorrhea ►May be associated with endometritis, salpingitis, pelvic inflammatory disease (PID) or chorioamnionitis ► Can be acute and chronic (most common)
- 8. Cervicitis ►Morphology: Gross- Eversion of ectocervix with hyperemia, edema and granular surface Nabothian(retention cysts) may be grossly visible as pearly grey vesicles. Histopathology : - Inflammation of cervical mucosa with increased lymphocytes, plasma cells, neutrophils ( acute) and tingible body macrophages, - Columnar cell proliferation (micro- glandular change) - Nabothian cysts/ follicles (due to occlusion of cervical gland ducts ) & - Squamous metaplasia
- 12. Cervical neoplasia ►Most common gynecologic malignancy world wide ►Ranks 3rd among all malignancies among females ►Incidence has reduced to almost 80% with regular PAP screening ►HPV has been implicated as one of the most common and highly oncogenic etiological agent ►In India –most common malignancy; along with breast it forms almost 40% of cancer of all sites ►Incidence varies from 21%-50% ►Occurs in the transformation zone as intraepithelial neoplasia progressing on to invasive carcinoma through carcinoma in situ(CIS)
- 13. Cervical neoplasia Transformation Zone ►Continuous change in ecto & endocervical lining ►Before puberty squamo-columnar junction (SCJ) situated in internal os ►At the onset of puberty, after pregnancy the columnar epithelium extends towards ectocervix beyond external os ►This columnar epithelium in ectocervical region gets exposed to low pH of vaginal mucus which in time undergoes squamous metaplasia(SM) ►The epithelium between the changing SCJ’s are the most labile and prone to premalignant and malignant change- Transformation Zone
- 15. v The squamocolumnar junction (SCJ): Junction between the squamous epithelium and the columnar epithelium. v Its location on the cervix is variable. v The SCJ is the result of a continuous remodeling process resulting from uterine growth, cervical enlargement and hormonal status. v During this process the original SCJ everts along with large portions of columnar epithelium from their initial position onto the ectocervix.
- 16. Cervical squamocolumnar junction showing mature, glycogenized (pale) squamous epithelium, immature (dark pink) squamous metaplastic cells, and columnar endocervical glandular epithelium
- 17. Cervical neoplasia- etiopathogenesis ►Multiple etiologic agents v Persistent infection with Human papilloma virus- 16, 18 v Early age of marriage & intercourse v Multiple sexual partners v Dietary deficiency: Vit A, Folic acid v Cigarette smoking: polycyclic aromatic hydrocarbons are carcinogenic and forms damaging DNA adducts in cervical epithelium v Multiparity v Lack of circumcision of male partner: accumulation of smegma which is carcinogenic and might induce malignant transformation v Oral contraceptive usage v Immunosupression
- 18. Cervical neoplasia- etiopathogenesis Human papilloma virus ( HPV): v High risk: subtypes 16,18 (MC), 31,33,35 v Low risk: 6,11,42,44 ( cause condyloma) v HPV exposure occurs through sexual transmission v The epithelial cells get transformed to premalignant change (CIN/ IEN) v In malignant transformation HPV-DNA gets covalently linked and gets incorporated within the host genome v HPV 16& 18 and its gene E 6 produces protein which binds to cancer supressor gene (p53) in the host and causes proteolytic digestion of p53 v Other HPV’s through E7 gene binds to another tumor suppressor gene (Rb) v This destroys the ability of both p53 and Rb gene to suppress carcinogenic transformation by affecting cell cycle regulation v Similar transformation can also occur in endocervical cells leading to adenocarcinoma
- 21. Cervical intraepithelial neoplasia(CIN) ►Spectrum of dysplasia (atypical change) confined within the epithelium (intraepithelial) that begins in basal layers and progressively involves other layers to form carcinoma in situ ►Classification based upon the cellular atypia and involvement of different thickness of the epithelium ►Earlier were classified in 3 grades: CIN I, CIN II, CIN III; Conventionally graded as mild, moderate, & severe dysplasia v CIN I: involvement of basal one third of epithelium (mild) v CIN II: lower two third involvement ( mod. Dysplasia) v CIN III: > than two third but not involving entire thickness (severe dysplasia) v Carcinoma in situ (CIS): involvement of complete thickness of the epithelium with intact basement membrane ►The atypical changes includes: - Increased nuclear size, hyperchromasia and increased mitotic rate, Increased N/C ratio and loss of polarity
- 22. Squamous intrepithelial neoplasia (SIL) ►National Cancer Institute proposed this terminology in Bethesda system for cervical and vaginal cytology reporting ►3 grades (# TIER system)of CIN have been adjusted in 2 grades (2 TIER system)of squamous intraepithelial lesion ►Low grade SIL (LSIL) and High grade SIL (HSIL) ►LSIL corresponds to CIN I; is a flat condyloma with koilocytic atypia, related to HPV 6& 11 infection ►HSIL corresponds to CIN II & III with abnormal pleomorphic atypical squamous cells. HPV 16 & 18 have been implicated in its etiology ► LSIL: 60% of them regress and around 10% progresses to HSIL ►HSIL: 30 % pf the lesion regress and about 10% progresses to invasive carcinoma
- 25. Nuclear atypia in LSIL. : The most significant feature of LSIL is nuclear atypia. This is characterized by nuclear enlargement, hyperchromasia, nuclear irregularity, and variation in nuclear size Koilocytosis in LSIL. : The cytological features of a productive HPV infection include multinucleation and perinuclear cytoplasmic cavitation or halos. The combination of nuclear atypia and cytoplasmic halos is referred to as koilocytosis.
- 26. HSIL with marked variability in nuclear size (anisonucleosis). Anisonucleosis is a variable feature of HSIL HSIL: Undifferentiated neoplastic cells replace 50–70% of the epithelium. The nuclear : cytoplasmic ratio is high, and the cytoplasmic membranes and the basal layer are indistinct
- 27. Detection and screening of premalignant lesions ►Criteria for screening test: Simple, specific, cost effective, acceptable, accurate, repeatable, can be performed by paramedics/ staff ►Benefits of early detection: Improve prognosis ( decrease mortality & morbidity , Increased survival), less radical treatment ►SCREENING: Methods of prevention v Primary : Avoid precipitating/ risk factors, vaccination, counselling v Secondary: Screening, early detection v Tertiary: Treatment or mitigation of damage ►Secondary: Systemic application of a test in an asymptomatic person to detect early lesions; Can be selective ( high risk group) or Mass screening
- 28. Prevention of cervical cancer
- 29. Detection and screening of premalignant lesions ►Methods of cervical screening: v Cytological: Conventional PAP smear, Liquid based cytology; automated cytological screening v HPV testing: v Visual: VIC, Colposcopy, cervicography ►PAP Smear: Named after Dr. George Papanicolaou (1883-1962) ►Usefulness of PAP smear Ø Effective screening method to detect premalignant and malignant lesions Ø Long latent period of 10-15 years between CIN and invasive cancer allows adequate treatment of CIN and prevention of invasive cancer has been proved successful in reducing the incidence of invasive cancer by 80% and the mortality by 70% Ø It is important to detect at early stages as low grade lesions are usually reversible with adequate early treatment
- 30. Detection and screening of premalignant lesions ► When to screen § Start within 3 years of onset of sexual activity or by age of 21, whichever is first § High risk factors for cervical dysplasia: Early onset of sexual activity ,Multiple sexual partners ,Smoking habits ,Oral contraceptives ,HPV and HIV positive women ►Screening frequency : § Yearly until three consecutive normal pap smears, then may decrease frequency to every 2-3 years § Annual screening for high-risk women is highly recommend. ► When to stop routine screening § Age 70 and “adequate recent screening” § Three consecutive negative pap smears § No abnormal pap smears in last 10 years § Hysterectomy for benign lesion
- 32. Cervical carcinoma ►Classification: - Squamous cell carcinoma: Large cell keratinizing or Non-keratinizing, Small cell and Verrucous - Adenocarcinoma: Endocervical, clear cell, endometrioid, adenoid cystic, adenoma malignum - Mixed: Adenosquamous, glassy cell - Neuroendocrine: large and small - Others: Lymphoma, melanoma and sarcoma
- 33. Cervical carcinoma ►SCC is the most common histologic subtype of cervical cancer, accounting for approximately 80% of cases ►HSIL is an immediate precursor of cervical SCC ►Cervical adenocarcinoma- 2nd most common (15%) followed by adenosquamous & neuroendocrine (<5%) ►Peak age incidence is 45 years ►Etiopathogenesis – same as preinvasive cancers
- 34. Pathogenesis of cervical carcinoma
- 35. Invasive cervical carcinoma- morphology ►GROSS: 3 distinct types: § Fungating, ulcerating and infiltrating § Fungating: cauliflower like growth protruding into the vaginal cavity; most common; can be endophytic ( within the endocervical canal) ►M/E: 4 types § Squamous ( epidermoid) cell carcinoma- most common can be large cell (keratinizing and non keratinizing) & small cell type § Adenocarcinoma ( papillary & glandular pattern) § Adenosquamous § undifferentiated
- 37. Squamous cell carcinoma (SCC) ►Large cell Keratinizing - Large cells with moderate to abundant pink keratinized cytoplasm - Cells are arranged in sheets, clusters - Severe degree of pleomorphism with high mitotic rate and frequent mitosis - At places keratinized epithelium are present in concentric whorls- keratin pearls ►Non –keratinizing- no keratin pearls ( mod diff SCC) ►Small-cell non-keratinizing: small cell with large hyperchromatic nuclei and scant eosinophilic cytoplasm; has poor prognosis
- 38. Squamous cell carcinoma of the cervix. A, Microinvasive squamous cell carcinoma with invasive nest breaking through the basement membrane of HSIL. B, Invasive squamous cell carcinoma
- 41. Adenocarcinoma of the cervix. A, Adenocarcinoma in situ (arrow) showing dark glands adjacent to normal, pale endocervcial glands. B, Invasive adenocarcinoma.
- 42. Staging of cervical cancer
- 43. Spread and clinical staging of cervical carcinoma ► SPREAD: v Direct spread: urinary bladder, peritoneum, ureter, rectum vagina v Lymphatic spread: paracervical lymph nodes, obturator LN’s, external iliac group of LN’s v Hematogenous spread: liver, lung bones ► STAGING: v Stage 0: carcinoma in situ (CIS) v Stage I: carcinoma confined to cervix v Stage II: carcinoma involving parametrium ( but not upto pelvic wall) or upper 2/3rd of vagina v Stage III: carcinoma extending to pelvic wall and or lower 2/3rd of vagina v Stage IV: carcinoma spreading beyond pelvis or involving mucosa of urinary bladder or rectum along with distant metastasis
- 44. Treatment Depends upon the stage of the disease
- 45. Cervical carcinoma: clinical features & complications ►Bleeding per vaginum: irregular, intermenstrual, post coital, post menopausal ►Vaginal discharge; copious, purulent ►Urinary symptoms: dysuria, hematuria, frequency ►Cachexia ►Low back pain ►COMPLICATIONS: Pyometra, vesicovaginal fistula, uretric obstruction leading to hydro- nephrosis, uremia ►D/D: Cervical tuberculosis, Syphilitic cervicitis- Cervical ulcers Polyps: mucus, cervical, fibroid Endometrial carcinoma
- 46. Cervical cancer: Investigations ►Pap smear: if no obvious lesion ►Colposcopy ►Cervical biopsy ( obvious lesions) ►Pretreatment investigations: Routine CBC, RFT,LFT, urine R/E,CXR, abdomen and pelvic U/s , MRI, IVU, PET CT ►Cystoscopy, Proctoscopy ►Molecular testing for CIN: HPV,p 16, p 21, Ki-67 ( proliferative index), pRb & p 53 gene mutational studies
- 47. At the end of this session medical student should be able to: ►Discuss the etiology and morphological features of cervicitis. ► Discuss the epidemiology of carcinoma cervix ► Enumerate the etiological factors for the development of carcinoma cervix. ►Describe the pathogenesis of carcinoma cervix. ►Describe the progression of carcinoma cervix. ►Discuss the pathological features of carcinoma cervix ►Discuss the methods of diagnosis of carcinoma of cervix. ►Enumerate and discuss various screening methods and programs for early detection of carcinoma cervix