Cáncer gástrico
•
2 likes•756 views

Presentación realizada en el marco de la I Jornada de actualización e innovación en Oncología que tuvo lugar en el CIBA en enero de 2015.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cáncer gástrico
Similar to Cáncer gástrico (20)
More from Instituto Aragonés de Ciencias de la Salud - IACS
More from Instituto Aragonés de Ciencias de la Salud - IACS (20)
Recently uploaded
Recently uploaded (20)
Cáncer gástrico
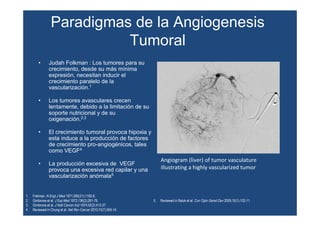
- 1. Paradigmas de la Angiogenesis Tumoral • Judah Folkman : Los tumores para su crecimiento, desde su más mínima expresión, necesitan inducir el crecimiento paralelo de la vascularización.1 • Los tumores avasculares crecen lentamente, debido a la limitación de su soporte nutricional y de su oxigenación.2,3 • El crecimiento tumoral provoca hipoxia y esta induce a la producción de factores de crecimiento pro-angiogénicos, tales como VEGF4 • La producción excesiva de VEGF provoca una excesiva red capilar y una vascularización anómala5 1. Folkman. N Engl J Med 1971;285(21):1182-6. 2. Gimbrone et al. J Exp Med 1972;136(2);261-76. 3. Gimbrone et al. J Natl Cancer Inst 1974;52(2):413-27. 4. Reviewed in Chung et al. Nat Rev Cancer 2010;10(7):505-14. Angiogram (liver) of tumor vasculature illustrating a highly vascularized tumor 5. Reviewed in Baluk et al. Curr Opin Genet Dev 2005;15(1):102-11.
- 2. Tumor Angiogenesis Overview Reviewed in Tugues et al. Mol Aspects Med 2011;32(2):88-111.
- 3. Tumor Hypoxia and Angiogenesis • Hypoxia: low local oxygen concentration • Tumor hypoxia is the primary stimulus for VEGF production1,2 • Excessive VEGF initiates the tumor angiogenic process2 1. Reviewed in Chung et al. Nat Rev Cancer 2010;10(7):505-14. 2. Reviewed in Papetti and Herman. Am J Physiol Cell Physiol 2002;282(5):C947-70.
- 4. The VEGF Family of Ligands and Receptors in Tumor Angiogenesis and Lymphangiogenesis 1. Reviewed in Adams and Alitalo. Nat Rev Mol Cell Biol 2007;8(6):464-78. 2. Reviewed in Hicklin and Ellis. J Clin Oncol 2005;23(5):1011-27.
- 5. VEGF Overexpression Associated with Poor Prognosis in Cancer Patients • Colorectal cancer1,2 • Gastric cancer3,4 • Pancreatic cancer5,6 • Breast cancer7,8 • Prostate cancer9 • Lung cancer10 • Melanoma11 • Hepatocellular carcinoma12 • Ovarian cancer13 1. Lee et al. Eur J Cancer 2000;36(6):748-53. 2. Takahashi et al. Cancer Res 1995;55(18):3964-8. 3. Takahashi et al. Clin Cancer Res 1996;2(10):1679-84. 4. Maeda et al. Cancer 1996;77(5):858-63. 5. Fujimoto et al. Eur J Cancer 1998;34(9):1439-47. 6. Ikeda et al. Br J Cancer 1999;79(9-10):1553-63. 7.Berns et al. Clin Cancer Res 2003;9(4):1253-8. 8.Manders et al. Br J Cancer 2002;87(7):772-8. 9.George et al. Clin Cancer Res 2001;7(7):1932-6. Survival rate in gastric cancer after potentially curative resection (by tumor VEGF expression [immunohistochemistry]) 10. Fontanini et al. J Natl Cancer Inst 1997;89(12):881-6. 11. Gorski et al. J Am Coll Surg 2003;197(3):408-18. 12. Poon et al. Br J Surg 2004;91(10):1354-60. 13. Yu et al. Gynecol Oncol 2013;128(2):391-6. This image was manually created from the original source Months after Surgery VEGF negative (n = 61) VEGF positive (n = 34) p<.05
- 6. Fundamentos del Tratamiento Anti-angiogénico • Los tumores colorectales con actividad angiogénica elevada se corresponden con fenotipos agresivos y peor pronóstico.1 • La neo vascularización es un indicador pronóstico significativo en cánceres de mama y de ovario.2 • Se han objetivado asociación entre la densidad de micro vasos, la expresión de VEGF y el pronóstico de los pacientes con cáncer de mama 2, de ovario 2, hepatocarcinoma3,4, NSCLC5 y cáncer gástrico6. • En el cáncer gástrico, existe una correlación entre la densidad de los vasos sanguíneos y la incidencia de metastatización. 6,7 1. Giatromanolaki et al. Am J Clin Oncol 2006;29(4):408-17. 2. Delli Carpini et al. Angiogenesis 2010;13(1):43-58. 3. Zhu et al. Nat Rev Clin Oncol 2011;8(5):292-301. 4. Yang et al. Gut 2010;59(7):953-62. 5. Salgia. Cancer 2011;117(17):3889-99. 6. Maeda et al. Cancer 1996;77(5):858-63. 7. Tanigawa et al. J Clin Oncol 1997;15(2):826-32.
- 7. VEGFR-2 Is a Critical Mediator of Angiogenesis 1. Holmes et al. Cell Signal. 2007;19:2003-2012 2. Youssoufian et al. Clin Cancer Res. 2007;13 (suppl 18):5544s-5548s.
- 8. Strategies for Blocking the VEGF Receptor Pathways Antibody to VEGFR-2 • Blocks ligand binding • Blocks receptor activation and signaling Ramucirumab Tyrosine kinase inhibitor to VEGFR-2 • Blocks receptor kinase activity and signaling Sorafenib Sunitinib Pazopanib Vandetanib Axitinib Inhibition of VEGF ligand • Blocks VEGF binding • Inhibits signaling due to VEGF(s) Bevacizumab Aflibercept Ziv-aflibercept Neovastat Reviewed in Tugues et al. Mol Aspects Med 2011;32(2):88-111. Cediranib Brivanib alaninate Motesanib Linifanib Tivozanib
- 9. Ramucirumab (IMC-1121B): A Fully Human VEGF Receptor-2 Antagonist • Isolated from phage display library of human Fab fragments from non-immunized donors1 • Fully human anti-VEGFR-2 IgG1 monoclonal antibody1 – High affinity (KD = 50 pM)1 – Blocks VEGF binding to VEGFR-2 • (IC50 = 0.8 nM)1 1. Lu D et al. J Biol Chem.2003;278(44):43496-43507. 2. Miao H-Q et al. Biochem Biophys Res Commun.2006;345:438-445. . 3.Zhu Z et al. Leukemia. 2003;17:604-611. • Biochemical and anti-tumor effects – Inhibits ligand-dependent VEGFR-2 activation and signaling1 – Inhibits proliferation and migration of human endothelial cells2 – Direct anti-tumor effect in NOD-SCID mice inoculated with VEGFR-2+ HL60 leukemic cells3
- 10. Ramucirumab Phase 3 Program Breast Cancer ROSE First-Line (N = 1113) 2:1 Ramucirumab (10 mg/kg) +/- Docetaxel (75mg/m2) q 3 weeks Enrollment complete (n = 1144) Gastric GEJ Cancer REGARD Second-Line (N = 348) 2:1 Ramucirumab (8 mg/kg) q 2 weeks vs. Placebo Enrollment complete (n = 355) RAINBOW Second-Line (N = 663) Ramucirumab (8 mg/kg) +/- Paclitaxel (80mg/m2) q 2 weeks Enrollment complete (n=663) Hepatacellular Carcinoma REACH Second-Line, post-Sorafenib (N = 544) Ramucirumab (8mg/kg) q 2 weeks vs. Placebo >380 pts (Child Pugh A) rand. as of Sept 2012 Colorectal Carcinoma RAISE Second-Line, FOLFOX/ Bev Res (N = 1050) Ramucirumab (8mg/kg) +/- FOLFIRI q 2 weeks >580 pts rand. as of Sept 2012 Lung Cancer REVEL Second-Line (n = 1242) Ramucirumab (10mg/kg) +/- Docetaxel (75mg/m2) (60mg/m2 Korea/Taiwan) q 3 weeks >900 pts rand. as of Sept 2012
- 11. Ramucirumab Monotherapy for Previously Treated Advanced Gastric or Gastro-esophageal Junction Adenocarcinoma (REGARD) An International, Multicenter, Placebo- controlled, Phase 3 Trial
- 12. Gastric Cancer Overview1 • Fourth most common malignancy and second leading cause of cancer mortality worldwide1 − Two-thirds of patients present with advanced or metastatic disease at diagnosis • Less common in the United States, where gastric cancer ranks 13th in cancer mortality2,3 • Cytotoxic chemotherapies are typically used as standard first-line therapy1 (platinos, pirimidinas fluoradas) • No second-line therapy is currently approved by the USFDA, EMA, or most other governmental drug regulatory agencies1 (taxanos, CPT-11) 1. Fuchs et al. Lancet 2013;[Epub Ahead of print]. 2. Parkin et al. CA Cancer J Clin 2005;55(2):74-108. 3. Siegel et al. CA Cancer J Clin 2013;63(1):11-30.
- 13. Ramucirumab: Rationale for Therapy • VEGFR-2 and its ligands are important mediators of angiogenesis and likely important therapeutic targets in gastric cancer1 − VEGFR-2 inhibition has been associated with reduced tumor growth and vascularity in animal models of gastric adenocarcinoma2 − Circulating and tumoral VEGF levels are associated with increased tumor aggressiveness and reduced survival in patients with gastric cancer3,4 • Ramucirumab, a human IgG1 monoclonal antibody VEGFR-2 antagonist, prevents ligand binding to the receptor, which blocks activation of receptor-mediated pathways in endothelial cells5-9 1. Yousouffian et al. Clin Cancer Res 2007;13(18 Pt 2):5544s-8s. 2. Jung et al. Eur J Cancer 2002;38(8):1133-40. 3. Tanigawa et al. J Clin Oncol 1997;15(2):826-32. 4. Yoshikawa et al. Cancer Lett 2000;153(1-2):7-12. 5. Lu et al. J Biol Chem 2003;278(44):43496-507. 6. Tvorogov et al. Cancer Cell 2010;18(6):630-40. 7. Goldman et al. FASEB J 2007;21(4):1003-12(Updated 8: p 1942). 8. Miao et al. Biochem Biophys Res Commun 2006;345(1):438-45. 9. Zhu et al. Leukemia 2003;17(3):604-11.
- 14. REGARD: Study Design Study locations: Europe; North, South, and Central America; Asia, Africa, Australia/New Zealand Primary endpoint: Overall survival Secondary endpoints: Progression-free survival, objective response rate, duration of response, safety, patient- reported outcomes, immunogenicity Until progression Every 2 weeks • Gastric or GEJ adenocarcinoma (metastatic or locally advanced and unresectable) • Prior platinum and/or fluoropyrimidine • ECOG PS 0-1 • No brain or CNS metastases • Measurable or evaluable disease (defined by RECIST version 1.0) Stratify •Geographic region •Weight loss (≥≥≥≥10% vs. <10%) over the prior 3 months •Location of primary tumor (gastric vs. GEJ) RANDOMIZE 2:1 Ramucirumab 8 mg/kg + Best supportive care Placebo + Best supportive care N = 355 Fuchs et al. Lancet 2013;[Epub Ahead of print].
- 15. REGARD: Key Inclusion Criteria • Metastatic or unresectable, locally recurrent, histologically or cytologically confirmed gastric or GEJ adenocarcinoma • Disease progression − During or within 4 months after the last dose of first-line therapy for metastatic disease, or − During or within 6 months after the last dose of adjuvant therapy • Measurable or evaluable disease (defined by RECIST version 1.0) • ECOG PS score 0-1 • Adequate hepatic, hematologic, coagulation, and renal function Fuchs et al. Lancet 2013;[Epub Ahead of print].
- 16. REGARD: Overall Survival HR (95% CI) = 0.776 (0.603, 0.998) Log-rank p-value (stratified) = .047 Placebo Ramucirumab Patients/events 117/99 238/179 Median OS, mos (95% CI) 3.8 (2.8, 4.7) 5.2 (4.4, 5.7) 6-month OS, % 32 42 12-month OS, % 12 18 Ramucirumab Placebo Number at Risk 238 154 92 49 17 7 3 0 0 117 66 34 20 7 4 2 1 0 Time Since Randomization, Months OverallSurvival,% Fuchs et al. Lancet 2013;[Epub Ahead of print]. Placebo Ramucirumab Censored
- 17. REGARD: Progression-free Survival HR (95% CI) = 0.483 (0.376, 0.620) Log-rank p-value (stratified) <.0001 Placebo Ramucirumab Patients/events 117/108 238/199 Median PFS, mos (95% CI) 1.3 (1.3, 1.4) 2.1 (1.5, 2.7) 12-week PFS, % 16 40 Progression-freeSurvival,% Time Since Randomization, Months Ramucirumab Placebo Number at Risk 238 213 113 65 61 45 30 18 18 11 5 4 2 1 1 1 1 117 92 27 11 7 4 2 2 2 2 2 1 1 0 0 0 0 Fuchs et al. Lancet 2013;[Epub Ahead of print]. Placebo Ramucirumab Censored 0 0
- 18. REGARD: Adverse Events of Special Interest Placebo (n = 115)a Ramucirumab (n = 236)a AE of special interest, n (%) Any Event Grade ≥3 Any Event Grade ≥3 Hypertensionb,c 9 8% 3 3% 38 16% 18 8% Bleeding/hemorrhageb 13 11% 3 3% 30 13% 8 3% Arterial thromboembolismb 0 - 0 - 4 2% 3 1% Venous thromboembolism 8 7% 5 4% 9 4% 3 1% Proteinuria 3 3% 0 - 7 3% 1 <1% Gastrointestinal perforation 1 <1% 1 <1% 2 <1% 2 <1% Fistula formation 1 <1% 1 <1% 1 <1% 1 <1% Infusion-related reaction 2 2% 0 - 1 <1% 0 - Cardiac failure 0 - 0 - 1 <1% 0 - a2 patients in each group did not receive treatment; bConsolidated term; cNo Grade 4 hypertension was observed Fuchs et al. Lancet 2013;[Epub Ahead of print].
- 19. REGARD: Key Findings1 • Compared to placebo, ramucirumab significantly prolonged OS (HR = 0.776, p = .047) and PFS (HR = 0.483, p<.0001) in patients with metastatic gastric or GEJ adenocarcinoma following progression on prior chemotherapies − Risk of death from any cause was reduced by 22% compared to placebo − Risk of disease progression was reduced by 52% • Survival benefit appeared consistently across virtually all subgroups and remained unchanged after multivariable adjustment for other prognostic factors • Ramucirumab appeared to be well tolerated, with similar rates for most adverse events between the ramucirumab and placebo groups – Hypertension was more common in the ramucirumab group, although Grade 3 hypertension was observed in only 7.6% of ramucirumab-treated patients 1. Fuchs et al. Lancet 2013;[Epub Ahead of print].
- 20. RAINBOW Phase 3, Randomized, Double-Blind Trial Ramucirumab and Paclitaxel (PTX) Versus Placebo and PTX Metastatic Gastric or Gastroesophageal Junction (GEJ) Adenocarcinoma Following Disease Progression on First-Line Platinum- and Fluoropyrimidine-Containing Combination Therapy
- 21. Treat until disease progression or intolerable toxicity • Important inclusion criteria: - Metastatic or loc. adv. unresectable gastric or GEJ* adenocarcinoma - Progression after 1st line platinum/fluoropyrimidine based chemotherapy •Stratification factors: - Geographic region, - Measurable vs non-measurable disease, - Time to progression on 1st line therapy (< 6 mos vs. ≥ 6 mos) Ramucirumab 8 mg/kg day 1&15 + Paclitaxel 80 mg/m2 day 1,8 &15 of a 28-day cycle N = 330 Placebo day 1&15 + Paclitaxel 80 mg/m2 day 1,8 &15 N = 335 S C R E E N R A N D O M I Z E Survival and safety follow-up RAINBOW: Study Design * GEJ= gastroesophageal junction; gastric and GEJ will be summarized under the term GC 1:1
- 22. RAINBOW: Geographic Regions Region 3: N=223 Hong Kong (3), Japan (140), Korea (45), Singapore (5), Taiwan (30)Region 2: N=44 Argentina (1), Brazil (35), Chile (4), Mexico (4) Region 1: N=398 Australia (41), Austria (6), Belgium (26), Bulgaria (12), Estonia (10), France (34 ), Germany (40), Great Britain (15), Hungary (29), Israel (30), Italy (28), Lithuania (12), Poland (33), Portugal (2), Romania (14), Russia (21), Spain (21), USA (24) Global: 170 study centers in 27 countries (Region 1 (18); Region 2 (4); Region 3 (5))
- 23. RAINBOW: Study Endpoints Primary endpoint ♦ Overall survival (OS) Secondary endpoints ♦ Progression-free survival (PFS) ♦ Time to progression (TTP) ♦ Objective response rate (ORR) ♦ Safety assessment ♦ Quality of life (Assessed by EORTC-QLQ-C30 & EQ-5D) ♦ Pharmacodynamic and immunogenicity profile ♦ Pharmacokinetics
- 24. RAINBOW: Baseline Tumor Characteristics RAM + PTX N=330 PBO + PTX N=335 n % n % TTP on 1st line < 6 months During 1st line 250 227 75.8 68.7 256 217 76.4 64.7 Primary tumor Gastric GEJ Present 264 66 209 80.0 20.0 63.3 264 71 209 78.8 21.2 62.4 Measurable disease Yes 267 80.9 273 81.5 Histologic subtype (Lauren classif.) Intestinal Diffuse 145 115 43.9 34.8 135 133 40.3 39.7 Metastases ≤ 2 Sites > 2 Sites Peritoneal Mets Ascites 209 121 163 130 63.3 36.7 49.4 39.3 232 103 152 107 69.3 30.7 45.4 31.9
- 25. RAINBOW: Overall Survival HR (95% CI) = 0.807 (0.678, 0.962) Stratified log rank p-value = 0.0169 RAM + PTX PBO + PTX Patients / Events 330 / 256 335 / 260 Median(mos) (95% CI) 9.63 (8.48, 10.81) 7.36 (6.31, 8.38) 6-month OS 72% 57% 12-month OS 40% 30% RAM + PTX 330 308 267 228 185 148 116 78 60 41 24 13 6 1 0 PBO + PTX 335 294 241 180 143 109 81 64 47 30 22 13 5 2 0 No. at risk Censored Δ mOS = 2.3 months
- 26. Category Subgroup N (RAM+PTX) N (PBO+PTX) HR Overall 330 335 0.807 Combined Geo. Regiona Region 1+2 221 221 0.732 Region 3 109 114 0.986 Time to PD on 1st-line Therapy < 6 months 250 256 0.871 ≥ 6 months 80 79 0.615 Disease Measurability Non-measurable 63 62 1.101 Measurable 267 273 0.750 Gender Male 229 243 0.814 Female 101 92 0.672 Age Group (yrs) < 65 204 212 0.753 ≥ 65 126 123 0.861 ECOG PS 0 117 144 0.778 1 213 191 0.771 Histologic Subtype Intestinal 145 135 0.705 Diffuse 115 133 0.856 Mix/Miss./Unk. 70 67 0.955 Number of Metastatic Sites ≤ 2 209 232 0.749 > 2 121 103 0.815 Primary Tumor Location Gastric 264 264 0.899 GEJ 66 71 0.521 Prior Gastrectomy Yes 133 126 0.939 No 197 209 0.753 Peritoneal Metastases Yes 163 152 0.807 No 167 183 0.758 Forest Plot of Overall Survival by Subgroups - Stratified Analysis a Region 1: Europe, United States, and Australia; Region 2: Brazil, Chile, Mexico, and Argentina; Region 3: Japan, South Korea, Hong Kong, Taiwan, and Singapore. Favors RAM+PTX Favors PBO+PTX 0.5 1 20.2
- 27. RAINBOW: Post-discontinuation Treatment RAM + PTX (N=330) PBO + PTX (N=335) n (%) n % Patients with any PDT* 158 47.9 154 46.0 Chemotherapy 158 47.9 152 45.4 Targeted Antibody 23 7.0 18 5.4 Targeted Small Molecule 1 0.3 5 1.5 Other 0 0.8 2 0.6 *Patients may have received more than one regimen. PDT = Post-discontinuation Treatment
- 28. HR (95% CI) = 0.635 (0.536, 0.752) Stratified log rank p-value < 0.0001 RAM + PTX PBO + PTX Patients / Events 330 / 279 335 / 296 Median(mos) (95% CI) 4.40 (4.24, 5.32) 2.86 (2.79, 3.02) 6-Month PFS 36% 17% 9-Month PFS 22% 10% Response Rate 28% 16% p = 0.0001 Disease Control Rate 80% 64% p < 0.0001 RAM + PTX 330 259 188 104 70 43 28 15 11 7 3 1 PBO + PTX 335 214 124 50 34 21 12 8 5 3 3 3 No. at risk Censored RAINBOW: Progression-free Survival & Response Rates
- 29. Category Subgroup N (RAM+PTX) N (PBO+PTX) HR Overall 330 335 0.635 Combined Geo. Regiona Region 1+2 221 221 0.639 Region 3 109 114 0.628 Time to PD on 1st-line Therapy < 6 months 250 256 0.676 ≥ 6 months 80 79 0.512 Disease Measurability Non-measurable 63 62 0.833 Measurable 267 273 0.599 Gender Male 229 243 0.592 Female 101 92 0.670 Age Group (yrs) < 65 204 212 0.572 ≥ 65 126 123 0.673 ECOG PS 0 117 144 0.663 1 213 191 0.568 Histologic Subtype Intestinal 145 135 0.531 Diffuse 115 133 0.695 Mix/Miss./Unk. 70 67 0.734 Number of Metastatic Sites ≤ 2 209 232 0.639 > 2 121 103 0.577 Primary Tumor Location Gastric 264 264 0.694 GEJ 66 71 0.387 Prior Gastrectomy Yes 133 126 0.624 No 197 209 0.641 Peritoneal Metastases Yes 163 152 0.726 No 167 183 0.526 Forest Plot of Progression-Free Survival by Subgroups - Stratified Analysis Favors RAM+PTX Favors PBO+PTXa Region 1: Europe, United States, and Australia; Region 2: Brazil, Chile, Mexico, and Argentina; Region 3: Japan, South Korea, Hong Kong, Taiwan, and Singapore. 0.5 1 20.2
- 30. Region* RAM + PTX PBO+ PTX Delta HRa/ Odds Ratiob 95% CI mOS (mos) Asia 12.1 10.5 1.6 0.99a 0.73, 1.34 EU/NA/AUS + Central/South Am. 8.5 5.9 2.6 0.73a 0.59, 0.91 mPFS (mos) Asia 5.5 2.8 2.7 0.63a 0.47, 0.83 EU/NA/Aus + Central/South Am. 4.2 2.9 1.3 0.64a 0.52, 0.79 RR (%) Asia 33.9% 20.2% 13.7% 2.24b 1.18, 4.24 EU/NA/Aus Central/South Am. 24.9% 14.0% 10.9% 2.09b 1.28, 3.41 RAINBOW: Efficacy by Geographic Region *Accrual: Asia n=223; EU/NA/AUS n=398; Central / South America n=44
- 31. RAM + PTX (N=327) PBO + PTX (N=329) Preferred Term† Any Grade (%) Grade ≥3 (%) Any Grade (%) Grade ≥3 (%) Fatigue† 56.9 11.9 43.8 5.5 Neutropenia† 54.4 40.7 31.0 18.8 Neuropathy† 45.9 8.3 36.2 4.6 Decreased appetite 40.1 3.1 31.9 4.0 Abdominal pain† 36.1 6.1 29.8 3.3 Leukopenia† 33.9 17.4 21.0 6.7 Diarrhea 32.4 3.7 23.1 1.5 Epistaxis 30.6 0 7.0 0 Vomiting 26.9 3.1 20.7 3.6 Hypertension† 25.1 14.7 5.8 2.7 Peripheral Edema 25.1 1.5 13.7 0.6 Treatment-Emergent Adverse Events Occurring in ≥ 20% of Patients and ≥ 5% Higher in the RAM + PTX Arm †Consolidated AE terms are comprised of synonymous MedDRA preferred terms: fatigue includes asthenia; neutropenia includes neutrophil count decreased; neuropathy includes peripheral sensory neuropathy; paraesthesia; neuropathy peripheral, polyneuropathy; hypoasethesia, neuralgia, dysaesthesia; abdominal pain includes abdominal pain upper and abdominal pain lower; leukopenia includes white blood cell decreased; hypertension includes blood pressure increased, hypertensive cardiomyopathy, procedural hypertension, systolic hypertension.
- 32. Adverse Events of Special Interest RAM + PTX (N=327) PBO + PTX (N=329) Category of event† Any Grade (%) Grade ≥3 (%) Any Grade (%) Grade ≥3 (%) Bleeding/Hemorrhage Epistaxis 41.9 30.6 4.3 0 17.9 7.0 2.4 0 Hypertension 25.1 14.7 5.8 2.7 Proteinuria 16.8 1.2 6.1 0 GI hemorrhage 10.1 3.7 6.1 1.5 Renal failure 6.7 1.8 4.3 0.9 Infusion-related reaction 5.8 0.6 3.6 0 Venous thromboembolic 4.0 2.4 5.5 3.3 Cardiac failure 2.4 0.6 1.2 0.6 Arteriothromboembolic 1.8 0.9 1.5 0.9 GI perforation 1.2 1.2 0.3 0 †Each AESI category is comprised of consolidated synonymous MeDRA preferred terms.
- 33. RAINBOW: Results and Conclusions ♦ RAINBOW met the primary endpoint - RAM + PTX conferred a statistically significant and clinically meaningful OS benefit of > 2 months (median); risk reduction of death by 19% - Significant benefits in PFS and ORR were observed ♦ RAINBOW and the recently published REGARD trial demonstrate that ramucirumab is an effective new drug for the treatment of patients with metastatic or locally advanced unresectable gastric and GEJ cancer after prior chemotherapy ♦ This largest gastric cancer 2nd line trial clearly underlines that effective second line therapy improves survival of patients with metastatic or locally advanced unresectable gastric cancer