
Recommended
More Related Content
Similar to Discussion assignment & Instructions Below I need a mi.docx
Similar to Discussion assignment & Instructions Below I need a mi.docx (20)
More from elinoraudley582231
More from elinoraudley582231 (20)
Recently uploaded
Recently uploaded (20)
Discussion assignment & Instructions Below I need a mi.docx
- 1. Discussion assignment & Instructions Below I need a minimum 100- word initial response to the Assignment question. Then, I need a minimum of 50-word responses to TWO peers per their comments to the question below. Required a minimum of 2 scholarly reference, one is the eBook attached. If you use any outside reference, cite APA format. No plagiarism and 100% original work. Assignment question: Describe and differentiate the roles of hospitals and nursing homes in providing long- term care? Minimum 100- word initial response Peer#1 Minimum of 50 words Nursing homes are facilities that are licensed to provide that of short and long-term care to patients." They are facilities that are specialized in caring for people that are not able to care for themselves such as basic personal hygiene on there own, as well as Medicare pays substantially more for these services." (Green, 2015, p. 27). Nursing homes usually specialize in caring for the elderly but there are cases when a younger age group is cared for within a nursing home. A nursing home has nurses that are there to treat the patients on a round the clock basis but doctors do not make rounds everyday in a nursing home." Long-term care hospitals are facilities that patients are usually transferred to from a critical care or an intensive care unit." (Green, 2015, p.30). These hospitals
- 2. specialize in treating people who usually have more than one or more serious conditions or that they need a hospital level of care for an extended time but that the patient is expected to improve within a period of time are will be able to then return home. "Also a requirement for Medicare reimbursement in a long-term hospital the impatient length of stay has to be greater than that of 25 days but the average length of stay is right around 30 days." (Competty & Rosenberg, 2016, p.12). References: Competty, Brad & Rosenberg, Jessica (2016). A Guide To Care Facilities. Retrieved from: https://www.a- guide-to-care-facilities.com Green, L.E. (2015). Nursing Home vs Long-Term Care. Retrieved from: https://www.lingtermcarelink.net Peer#2 Minimum of 50 words Hospitals may provide a wide variety of long-term care, ranging from skilled nursing and rehabilitation services to less intensive long-term care. Hospital’s main focus has been acute care and health education. Skilled nursing care involves medical and skilled nursing care, therapy, and social services under the supervision of a licensed registered nurse on a 24- hour basis. Physical rehabilitation services encompass a comprehensive array of restoration services for the disabled and all support services necessary to help patients attain their maximum functional capacity. However, various types of hospital specialize in long-term care, including categories of psychiatric,
- 3. rehabilitation. Chronic disease, orthopedics, and long term defined as an average length of stay of 23 days or more (Williams & Torrens, 2008). Reference: Williams, S. J., & Torrens, P. R. (2008). Introduction to Health Services (Seventh ed.) https://www.a-guide-to-care-facilities.com/ https://www.a-guide-to-care-facilities.com/ https://www.lingtermcarelink.net/ CHAPTER TOPICS History of the Hospital The Scope of the Industry Structure of Hospitals and Health Systems Hospital Organization The Hospital and Medical Staff Key Issues Facing the Hospital Industry LEARNING OBJECTIVES Upon completing this chapter, the reader should be able to
- 4. 1. Understand the role of the hospital in today’s health care system. 2. Appreciate the historical trends that have shaped the hospital industry. 3. Understand the types of hospitals, ownership patterns, and differentiating characteristics of various hospitals. 4. Comprehend the development of health systems and the role of hospitals in such systems. 5. Follow the impact of competitive pressures and other developments on the structure and operation of hospitals and health systems. 6. Understand the internal organizational structure of hospitals. 182 CHAPTER 8 Hospitals and Health Systems Stephen J. Williams and Paul R. Torrens 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 182 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part.
- 5. T U R N E R - H O W A R D , T O N I - C L Y S A 5 9 4 0 B U CHAPTER 8 Hospitals and Health Systems 183
- 6. The hospital’s role in the nation’s health care sys- tem has changed dramatically over the years. The hospital originated as an institution for the poor, of- fering little in the way of therapy, and then evolved into the center of the system and the primary tech- nology focus of health care. Now the hospital is a provider of highly specialized services and the hub of an assortment of other activities. The traditional independence of each hospital has been dramati- cally altered by horizontal and vertical integration within the health care system such that today few hospitals are truly freestanding entities. The technol- ogy to manage hospitals has likewise changed with an information systems focus and the application of complex parameters of performance measurement. Expectations of consumers, providers, and pay- ers have also changed dramatically over the years with the anticipation of more effective interventions at more efficient and competitive pricing. Finally, as has always been the case in the past, the hospital in- dustry continues to face immense challenges, op- portunities, and expectations for the future. The hospital has also changed from an island of care to an institutional octopus, with tentacles springing out throughout the community, affiliat- ing with other institutions and providers, and pro- viding outreach services for consumers. On the inpatient side, hospitals are increasingly providing the most complex of care to the most critically ill patients. On the outpatient side, most hospitals are broadening the array of services that they offer to better compete.
- 7. Hospitals face the challenges of sick and dying patients, demanding payers, government officials seeking accountability, physicians demanding the availability of the latest equipment and support, and many other crosscurrents. Some hospitals are for-profit entities, while others are not-for-profit. Some hospitals are highly specialized while others offer a broad range of services. Hospitals are often major employers in their communities and many provide the bulk of indigent care for low-income and disenfranchised citizens. Through it all, the backbone of hospital management has increasingly adopted the managerial principles of commercial industry, seeking to provide services in an efficient, but cost-effective manner, and to offer competitive pricing to third-party and governmental payers. The challenges of this industry are immense and un- likely to recede in the decades that follow. HISTORY OF THE HOSPITAL Although the hospital today is in the forefront of technology and clinical medicine, the history of the nation’s hospitals actually began as facilities for housing the poor and the ill. These institutional warehouses for human suffering were the alms- houses, the pest houses, the poor houses, and the workhouses that sheltered the homeless, the poor, the mentally ill, those with serious degenerative dis- eases, and others for whom there was little to offer in the era before modern medicine. Isolation of in- dividuals during epidemics of cholera and typhoid, among other diseases, also led to the utilization of these institutions. Little medical knowledge was available and few individuals received any signifi-
- 8. cant treatment. The middle class avoided these institutions and received their care at home. Not until the 1700s and 1800s did hospitals emerge with a mission of providing some form of clinical medical care. Many of these early hospitals were supported by philan- thropic efforts and religious organizations. Also during this period, many public hospitals were es- tablished in various cities to provide for the social needs of local populations, laying the groundwork for our modern acceptance of local government as the provider of last resort. Finally, by the early 1900s, with the introduction of scientific method in medical practice and the recognition that hospitals and clinical medicine must adhere to a stricter formulation of practice fo- cused on scientific discovery, was the era of the truly modern hospital established. Throughout the twentieth century, the escalating advance of knowledge accelerated the focus of the 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 183 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R -
- 9. H O W A R D , T O N I - C L Y S A 5 9 4 0 B U hospital as a center for medical technology. After World War II, the hospital’s role as a center of tech- nology and innovation became firmly established. At this point, the practice of medicine itself was in- creasingly dependent on scientifically valid knowl- edge and training. Finally, over the past 30 years the degree of rigor of clinical practice and the scope of scientific knowledge has escalated greatly, and
- 10. the hospital has become a center of high standards, scientific applications, and advanced technological capability. At the same time, the increasing shift of services to an ambulatory care arena facilitated by technological advancement itself has left the hospital with an ever- more complex base of patient care, higher acuity, and higher costs. In addition, pressure from payers, as noted previously, has escalated greatly as has the expectation of providers and consumers alike. Indus- try consolidation, vertical and horizontal integra- tion, public policy concerns, and quality assessment and assurance have placed the operation of the na- tion’s hospitals under tremendous scrutiny. Yet, through it all, the nation’s hospitals have risen to the challenge of providing superlative care overall in a high-intensity, stressful atmosphere that has signifi- cantly contributed to our improved health status and well-being. This is a remarkable achievement in light of countervailing financial and political pressures that have always buffeted the hospital industry. We owe a great debt of gratitude to the nation’s hospitals and to those dedicated individuals who work within these institutional walls for achieving so much in an environment that started as a warehouse for the poor and sick, left to die without care and concern. THE SCOPE OF THE INDUSTRY Although the hospital industry has seen its share of the nation’s health care dollar decline some- what, hospital systems are still immense segments of the industry and of our nation’s economy. (See Table 8.1.)
- 11. In 2003, the hospital industry alone accounted for more than $500 billion of expenditures. In 1960, the industry counted for only $9.2 billion of eco- nomic activity annually. The growth of private health insurance and gov- ernment entitlement programs, particularly Medi- care, has shifted the burden of paying for hospital care to third parties. In 1960, more than 20 percent of the hospital bill was paid by people out of their own pockets; by 2003, this percentage had dropped to 3.2 percent. Private health insurance now accounts for a little more than one-third of all hospital expenditures while government programs account for nearly 60 percent. Medicare alone counts for nearly a third of all hospital expendi- tures; in many facilities the Medicare program pays about half the bill overall. Certainly, for the nation’s seniors, Medicare is a critical source of support for paying for the enormous costs of hospitalization. The number of hospitals in the United States has decreased dramatically. Table 8.2 illustrates this de- cline with the total number of hospital in 1975 at 7,156 dropping by 2003 to 5,764. A small number of the nation’s hospitals are owned and operated by the federal government. These include the Vet- eran’s Administration Hospitals and military facili- ties. The vast majority of hospitals are nonfederal and are nonprofit, for-profit, or owned by state and local governments. The information in this table 184 PART THREE Providers of Health Services Table 8.1. Hospital Expenditures by Source of
- 12. Funds: United States, Selected Years Source of Funds 1960 1990 2003 Amount in billions Hospital care expenditures $9.2 $253.9 $515.9 Percent Distribution All sources of funds 100.0 100.0 100.0 Out-of-pocket payments 20.8 4.4 3.2 Private health insurance 35.8 38.3 34.4 Other private funds 1.2 4.1 4.1 Government 42.2 53.2 58.3 Medicaid — 10.9 16.9 Medicare — 26.7 30.3 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 184 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H O W A R D ,
- 13. T O N I - C L Y S A 5 9 4 0 B U CHAPTER 8 Hospitals and Health Systems 185 Table 8.2. Hospital and Beds by Ownership and Hospital Size: United States, Selected Years Type of Ownership and Size of Hospital 1975 1995 2003 Hospitals Number All hospitals 7,156 6,291 5,764 Federal 382 299 239 Nonfederal 6,774 5,992 5,525 Community 5,875 5,194 4,895 Nonprofit 3,339 3,092 2,984 For profit 775 752 790
- 14. State-local government 1,761 1,350 1,121 Bed size 6–24 beds 299 278 327 25–49 beds 1,155 922 965 50–99 beds 1,481 1,139 1,031 100–199 beds 1,363 1,324 1,168 200–299 beds 678 718 624 300–399 beds 378 354 349 400–499 beds 230 195 172 500 beds or more 291 264 256 reflects hospital ownership, and it should be noted that some hospitals, while owned by one type of entity, may be operated under contract by another entity, such as a hospital management company. The largest grouping of hospitals in the nation are nonprofit community hospitals. Although their numbers have declined overall, they remain the pri- mary source of hospital care for most Americans. These hospitals are owned by nonprofit entities, although they are sometimes operated under con- tract by for-profit or other nonprofit corporations that specialize in managing hospitals and health systems. Nonprofit entities, including hospitals, function under special provisions of corporation law in each state, and under federal and state tax provisions that recognize their community service function. The na- tion has approximately 1 million nonprofit entities of various sorts and hospitals have long been a tra- ditional service provider in the nonprofit sector. Nonprofit entities serve a community service
- 15. and have special recognition under the law due to their role in our society. Nonprofit entities do not have owners and are governed by a community- based board that has ultimate authority for opera- tion of the entity. Nonprofit entities are generally exempt from most taxes at the federal, state, and local levels including income and property taxes. Many nonprofit entities have tax exempt status under Section 501C(3) of the federal tax code, al- lowing individuals to make potentially tax deductible donations to these organizations. Nonprofit enti- ties are able to raise funds through donations, re- tained earnings, and debt obligations, often on fa- vorable terms. Nonprofit entities may be “sponsored” by vari- ous types of organizations. Many hospitals have traditions of religious sponsorship. However, they are not owned by such sponsors. Nonprofit entities may also affiliate with each other through various organizational arrangements. Most nonprofit hos- pitals operate in a manner similar to other types of hospitals by employing modern management tech- niques, sophisticated information systems, and other 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 185 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E
- 16. R - H O W A R D , T O N I - C L Y S A 5 9 4 0 B U principles of twenty-first-century management. Non- profit entities are generally expected to provide some indigent care and serve the community in a variety of ways as well. A much smaller percentage of the nation’s hos-
- 17. pitals are operated as for-profit businesses. For- profit entities have owners and issue stock to those owners to reflect their equity position. For-profit en- tities, including hospitals, may be publicly or pri- vately held. Publicly held for-profit entities have stock that is available for purchase by anyone, typi- cally through the nation’s various stock exchanges. A variety of accountability and registration rules and regulations affect publicly owned for-profit entities, generally administered by the Securities and Exchange Commission at the federal level and similar entities at the state level. Privately held for-profit entities also issue stock, but that stock is not available to the general public for purchase. Accountability and other regulatory oversight are much less for privately held entities. For-profit hospitals may be independent and his- torically in this country and throughout the world today many for-profit hospitals have been owned by the physicians who practiced in them. Today, however, due to the tremendous capital costs of building, maintaining, and operating a hospital, most hospitals in the United States that are for profit are part of large multihospital chains, most of which are publicly traded. For-profit hospitals are not just accountable to the community but must also provide a return on investment to the share- holders; therefore they expect to generate a profit to pay a return to the equity investors for their cap- ital. For-profit hospital companies may also man- age not-for-profit and governmental hospitals as a separate line of business. The third category of ownership in Table 8.2 is state and local government hospitals. These are
- 18. hospitals that are owned by state or local govern- ments, but again, may be managed under contract by other entities, either for-profit or not-for-profit management companies. Many local government hospitals are owned by counties or other local gov- ernment units. They are often the providers of last resort, bearing the burden of indigent care in their communities. In the western United States, hospital districts were created much like water districts to provide in- frastructure for communities as populations moved West. These local taxing districts were responsible for the construction and operation of hospitals for their communities. In recent years the taxing au- thority of these districts has accounted for a very small percentage of total hospital operational costs. As reflected in Table 8.2, the majority of the nation’s hospitals are relatively modest in size as measured by licensed hospital beds. The very large institutions are typically teaching hospitals, often associated with medical schools, and have a range of residency programs for postgraduate medical ed- ucation. The small hospitals are typically in rural areas, raising particularly complex issues regarding financial viability. Broadly speaking, large hospitals are more prevalent in the East as the trend over time has been to build smaller rather than larger facilities. Significant numbers of smaller hospitals, particu- larly in urban areas, have closed over the past 25 years due to financial and competitive pressures, and to the difficulty of efficiently operating a small
- 19. number of hospital beds. Specifying the optimal side of a hospital is particularly difficult given the complexity of services now offered on an inpatient basis. Most likely, the very small and very large hos- pitals are the least efficient. As reflected in Table 8.3, the total number of hospital beds has dropped from just under 1.5 mil- lion to just less than 1 million since 1975. This trend reflects a combination of closures and reduc- tions in operating licensed beds among those hos- pitals still in operation. Large hospitals, because of their size, account for a disproportionate share of the total number of hospital beds. About 70 per- cent of the nation’s hospital beds are in nonprofit facilities. As reflected in Table 8.4, there are approximately 36 million admissions to the nation’s hospitals every year, of which 25 million are to nonprofit hospitals. The number of admissions has been remarkably 186 PART THREE Providers of Health Services 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 186 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R -
- 20. H O W A R D , T O N I - C L Y S A 5 9 4 0 B U CHAPTER 8 Hospitals and Health Systems 187 Table 8.3. Hospital Beds by Ownership and Hospital Size: United States, Selected Years Type of Ownership and Size of Hospital 1975 1995 2003 Beds by Ownership Number
- 21. All hospitals 1,465,828 1,080,601 965,256 Federal 131,946 77,079 47,456 Nonfederal 1,333,882 1,003,522 917,800 Community 941,844 872,736 813,307 Nonprofit 658,195 609,729 574,587 For profit 73,495 105,737 109,671 State-local government 210,154 157,270 129,049 Bed size 6–24 beds 5,615 5,085 5,635 25–49 beds 41,783 34,352 33,613 50–99 beds 106,776 82,024 74,025 100–199 beds 192,438 187,381 167,451 200–299 beds 164,405 175,240 152,487 300–399 beds 127,728 121,136 119,903 400–499 beds 101,278 86,459 76,333 500 beds or more 201,821 181,059 183,860 Table 8.4. Hospital Admissions by Ownership and Hospital Size: United States, Selected Years Type of Ownership and Size of Hospital 1975 1995 2003 Beds by Ownership Number in thousands All hospitals 36,157 33,282 36,611 Federal 1,913 1,559 973 Nonfederal 34,243 31,723 35,637 Community 33,435 30,945 34,783 Nonprofit 23,722 22,557 25,668 For profit 2,646 3,428 4,481 State-local government 7,067 4,961 4,634
- 22. By hospital bed size 6–24 beds 174 124 162 25–49 beds 1,431 944 1,098 50–99 beds 3,675 2,299 2,464 100–199 beds 7,017 6,288 6,817 200–299 beds 6,174 6,495 6,887 300–399 beds 4,739 4,693 5,590 400–499 beds 3,689 3,413 3,591 500 beds or more 6,537 6,690 8,174 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 187 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H O W A R D , T O N I - C
- 23. L Y S A 5 9 4 0 B U stable over the years, but the total number of hos- pital days has declined dramatically due to sharp reductions in the average length of stay. A relatively small proportion of admissions to hospitals are ac- counted for by the smaller hospitals. Examining hospital utilization based on popu- lation data illustrates a significant decline in dis- charges per thousand U.S. population as reflected in Table 8.5. Overall explanation of this trend lies in changes in the number of Americans, which 188 PART THREE Providers of Health Services Table 8.5. Discharges and Days of Care, Nonfederal Short-Stay Hospitals: United States, Selected Years Characteristic 1980 2003 Discharges per 1,000 population Total 173.4 119.5
- 24. Age Under 18 years 75.6 43.6 18–44 years 155.3 91.3 45–54 years 174.8 99.5 55–64 years 215.4 145.7 65 years and over 383.7 367.9 Sex Male 153.2 104.4 Female 195.0 135.1 Geographic Region Northeast 162.0 127.6 Midwest 192.1 117.1 South 179.7 125.8 West 150.5 103.9 Days of care per 1,000 population Total 1,297.0 574.6 Age Under 18 years 341.4 195.5 18–44 years 818.6 339.7 45–54 years 1,314.9 477.2 55–64 years 1,889.4 735.9 65 years and over 4,098.3 2,088.3 Sex Male 1,239.7 546.7 Female 1,365.2 605.2 Geographic Region Northeast 1,400.6 694.4 Midwest 1,484.8 507.9 South 1,262.3 609.8 West 956.9 476.4
- 25. 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 188 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H O W A R D , T O N I - C L Y S A 5 9 4 0
- 26. B U CHAPTER 8 Hospitals and Health Systems 189 has led to a larger denominator. Declines in dis- charges are much more moderate for higher-age individuals. Overall, changes in technological innovation combined with financial pressures from payers has led to an increasing proportion of medical care being provided on an ambulatory basis, and to much shorter lengths of stay for equivalent diag- noses for those patients who are admitted to the hospital. The impact of these trends is to yield a much higher intensity or complexity of care for hospitalized patients. Table 8.6 presents hospital occupancy rates since 1975 for the nation’s hospitals. Even with shorter lengths of stay, the closure of many hospi- tals, and an overall reduction in the number of hos- pital beds, occupancy rates remain on the decline. On average, today, only about two-thirds of the nation’s hospital beds are filled with patients each night. This trend is evident in virtually every cate- gory of hospital ownership. In the days since September 11, 2001, and more recently since various epidemics and natural disas- ters, the issue of ideal targets for hospital occu- pancy rates has become much more complex. How
- 27. much capacity should be maintained for potential utilization in emergency situations is a complex policy issue. Maintaining unused capacity costs money. As a result, the industry has some reluc- tance to do so. On the other hand, operating at a more efficient level of occupancy, say 85 or 90 per- cent, not only restrains the ability to respond to normal fluctuations in utilization but also signifi- cantly impacts the ability of hospitals to respond to a critical community emergency situation. Al- ternatives for providing reserve back-up capacity for community-based emergencies have become an important priority as communities prepare for Table 8.6. Hospital Occupancy Rates by Ownership and Hospital Size: United States, Selected Years Type of Ownership and Size of Hospital 1975 1995 2003 Occupancy Rates by Ownership Percent All hospitals 76.7 65.7 68.1 Federal 80.7 72.6 64.8 Nonfederal 76.3 65.1 68.3 Community 75.0 62.8 66.2 Nonprofit 77.5 64.5 67.7 For profit 65.9 51.8 59.6 State-local government 70.4 63.7 65.3 By hospital size 6–24 beds 48.0 36.9 31.9 25–49 beds 56.7 42.6 44.6 50–99 beds 64.7 54.1 57.2 100–199 beds 71.2 58.8 62.6 200–299 beds 77.1 63.1 67.0
- 28. 300–399 beds 79.7 64.8 68.5 400–499 beds 81.1 68.1 70.7 500 beds or more 80.9 71.4 74.2 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 189 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H O W A R D , T O N I - C L Y S A 5
- 29. 9 4 0 B U unforeseen events without significantly impacting hospital cost structures. STRUCTURE OF HOSPITAL AND HEALTH SYSTEMS Although technological advancement and reim- bursement policy are among the key factors affect- ing the development of the hospital industry over the past half century, other dramatic changes in the corporate environment of health care and particu- larly of the hospital sector have served a prominent role in affecting hospital management. Horizontal and vertical integration and the affiliation of hospi- tals with each other and with other sectors of the health care system have been extremely important developments in the organizational structure in governance and in the operational management of the hospital industry. These changes in the legal and organizational environment have profoundly affected how the hospital industry is structured and lines of accountability. The introduction of an in- creasingly typical corporate environment for the hospital industry has, to an extent, changed the roles for the key players, affected the organizational design, and facilitated other related changes within the industry such as closures and consolidations.
- 30. Horizontal and Vertical Integration The development of organizational and financial efficiency in the hospital industry has been most ac- celerated by both vertical and horizontal integra- tion. Because both of these forms of integration have been occurring, it is certainly fair to say that this is an industry in transition still seeking a level of equilibrium that can respond to changes in the health care marketplace and pricing as well as pro- viding an adequate response to the invested com- munity. Along with horizontal and vertical integra- tion, the industry has experienced a tremendous phase of closures and consolidations, particularly affecting smaller institutions. The dramatic changes in the number of operating hospital beds and hospitals in the United States are a result of this process as the industry seeks to provide more competitive products and pricing, an increasingly market-driven health care economy dictated by such payers as the government programs and vari- ous forms of managed care. Both horizontal and vertical integration have ex- perienced ebbs and flows over the past decades. The objectives of integration of resources have also varied depending on the participants involved and local market conditions. National integration of various types, particularly for horizontal integra- tion, has also been driven in part by the behavior of for-profit entities. To this day, the success of both vertical and horizontal integration varies tremen- dously across the country, and changing economic and market conditions suggest that such integra-
- 31. tion is a dynamic rather than static process with players possibly assessing their assets and adding and subtracting from their portfolios. In horizontal integration, similar units of produc- tion affiliate with each other. For example, for-profit and not-for-profit chains of hospitals under com- mon ownership operating in different geographic locations all providing similar hospital-based ser- vices would be a horizontally integrated system. Horizontal integration occurs in the for-profit and not-for-profit sectors and can involve various levels of organizational affiliation from direct ownership to looser affiliation arrangements. Horizontal inte- gration, designed to provide an enhanced level of ef- ficiency of scale across multiple institutions and in related geographic areas, may serve to reduce dupli- cation of services and marketplace competition. In a form of horizontal integration associated with re- gionalization of health services, smaller hospitals may feed into larger tertiary care facilities. Horizon- tal integration may also facilitate operational effi- ciency such as purchasing, information systems, quality assurance, and management capacity. Hori- zontally integrated multihospital networks may es- tablish contractual arrangements with other types of 190 PART THREE Providers of Health Services 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 190 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U
- 32. R N E R - H O W A R D , T O N I - C L Y S A 5 9 4 0 B U CHAPTER 8 Hospitals and Health Systems 191 health care providers and participate in larger health
- 33. care delivery systems. Vertical integration implies the establishment of integrated health care delivery systems that incor- porate all or most aspects of the health care pro- cess. In this form of integration, inpatient hospital services, ambulatory care services, mental health, long-term care services, and other related health care products are incorporated into a comprehen- sive delivery system. Vertical integration, in many respects, is more complicated than horizontal inte- gration because it involves a range of highly diverse and not always easily integrated services.Vertical in- tegration was prompted by the objective of negoti- ating with insurers and managed-care providers such that the full range of services could be pro- vided in a contractual arrangement. In addition, vertical integration provides for feeding patient flows into hospital inpatient services and other crit- ical delivery components to ensure the financial viability of these institutions. Vertical integration al- lows for greater capture of patients within inte- grated systems and a more established institution- ally based relationship with physicians. Vertically integrated systems in managed-care settings typi- cally contract for a broad range of services rather than just for inpatient or other discrete care. Verti- cally integrated services provide a delivery chain for a range of health services rather than specializing in only one product. Vertically integrated systems have greater capture of premium dollars but at the same time, assume a greater degree of financial risk. This increased risk has represented a significant chal- lenge in recent years. Some vertically integrated sys- tems have also established their own health plans independently or in conjunction with insurance en-
- 34. tities. However, this trend has faced significant challenges from financial and legal perspectives and they increase the risk to the institutional provider. Both horizontally and vertically integrated sys- tems of care need to align physician interests with institutional objectives. This has always been a chal- lenge in health care and continues to be so, partic- ularly with today’s more competitive markets and pricing pressures. Vertically integrated systems may have a greater likelihood of success in this regard because they can control a broader range of delivery systems and capture more of the health care dollar. Physician ownership initiatives such as for ambula- tory, surgery centers, or even specialty hospitals are an additional threat to hospital delivery systems. HOSPITAL ORGANIZATION The traditional organization of hospitals is cen- tered around three sources of power. These are the governing entity, the medical staff, and the administration. Traditional hospital governance was predicated on independent institutions each with its own corporate-style board. Legally and structurally, the governing body has ultimate authority for all activ- ities and decision making within the organization, delegating certain tasks among administration and the medical staff. Among nonprofit entities, these boards were historically composed of well-to-do individuals who could provide a platform for fund- raising. Over time demands for accountability re-
- 35. sulted in substantially ramped-up professional rep- resentation on these governing bodies. Physicians, accountants, attorneys, and others with a knowl- edge base relevant to institutional governance were elected to membership. Although frequently a volunteer activity with minimal, at least by corpo- rate standards, pay and fringe benefits, public ser- vice was the key motivation. For-profit entities have typically been components of larger corporations with advisory rather than legally binding governing boards. Hospital governing entities have delegated day- to-day management of the institution to hospital administration and the clinical medical affairs to the medical staff, which itself is typically formally organized with by-laws, elected officials, and spe- cific duties and responsibilities. 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 191 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H O W A R
- 36. D , T O N I - C L Y S A 5 9 4 0 B U In recent years, considerable effort has been directed toward educating members of governing entities and hospitals to better understand the prin- cipals and legal responsibilities of hospital manage- ment and to more critically assess decision-making activities, particularly pertaining to large capital investments, organizational mission, the role and management of medical staff, and contractual ar- rangements with other entities. With both horizontal and vertical integration, the ultimate governance responsibility is typically shifted to the highest level of organizational struc-
- 37. ture. Depending on corporation status of compo- nents within the larger organization separate boards may exist with statutory authority or may serve primarily in an advisory capacity. In the for- profit sector, a parent organization governing board serves a corporate role analogous to that of any public or privately held for-profit corporation. In the publicly held environment, the corporate board has an additional legal responsibility at- tributable to securities; regulation and corporate governance are defined by state and federal laws. For all governing entities, specific duties and re- sponsibilities are specified in the legal charter or other documents creating the organization and defining the duties, responsibilities, and member- ship of the board. With increased accountability for individual and collective acts of governance, board members must assume that they do have personal and professional liability to perform their corporate duties in an appropriate fiduciary manner. Hospital administration has also changed appre- ciably over the years moving toward a more tradi- tional corporate operational approach. In addition, hospital management increasingly incorporates the delegation of responsibility to an array of other managers including, on the front lines, depart- mental administrators. Specific technical expertise is typically incorporated into the management structure in such areas as information systems, fi- nance, legal environment, quality assurance, mar- keting, and contracting. Traditional roles such as patient care, including the hotel function, physical plant, admissions, discharge, other operational
- 38. responsibilities, and various other key functions, are also represented. Today’s hospital administrators are often de- fined by traditional corporate titles and attractive pay packages. In the not-for-profit sector, senior- level hospital managers typically earn from the $100,000s to more than $500,000 per year. In the for-profit sector, these managers may also receive stock and stock options and other equity-related benefits. In both nonprofit and for-profit sectors, managers typically receive valuable benefit pack- ages and in some instances, pay for performance and other types of bonuses. Hospital administra- tors usually have a management-related back- ground or have clinical training and have worked their way into a management position or some combination of both. Hospital managers, like their employees, work in a relatively high-stress and de- manding environment, answering not only to their formal bosses, but also to the public, consumers, physicians, and other constituencies. THE HOSPITAL AND MEDICAL STAFF With authority delegated from the governing entity, the hospital medical staff has specific responsibili- ties related to the clinical care provided in the facil- ity and regulation of those individuals who practice clinically. Hospital and medical staffs are typically organized with elected officials, various commit- tees, and with a leadership role represented by the president of the medical staff. State medical practice laws generally prohibit di-
- 39. rect employment of physicians by hospitals. As a consequence, and due to historical independence of physician practices, physicians and other health care professionals have affiliated with institutions such as hospitals in a variety of other ways. Histor- ically, these affiliations have primarily been through membership in hospital medical staffs. More re- cently, hospitals and physicians have affiliated 192 PART THREE Providers of Health Services 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 192 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H O W A R D , T O N I -
- 40. C L Y S A 5 9 4 0 B U CHAPTER 8 Hospitals and Health Systems 193 through joint ventures such as physician/hospital organizations, indirect employment of practitioners in other contractual arrangements, hospital pur- chases of group practices, and a variety of other models. Hospital medical staff membership has generally followed a model whereby physicians apply for hospital privileges in their area of specialty and are vetted by a committee of the hospital medical staff supported by administration. If found to be of good character and having a reputable clinical rep- utation, physicians are granted privileges, which is, in essence, the ability to admit and discharge pa- tients, provide care within the hospital facilities, and serve as a participating member of the medical staff. Although the governing entity is ultimately re- sponsible for granting privileges, this responsibility is usually delegated to the medical staff in recogni-
- 41. tion of their knowledge of clinical practice and abil- ity to assess professional skills. The evaluation of individuals for the granting of privileges is one of the key and most important roles of the medical staff. Physicians, for example, are evaluated on their medical and specialty residency training, their track record of clinical care as reflected in medical malpractice and other quality assurance indicators, and their reputation in other respects. When a physician is granted privileges, he or she remains subject to surveillance by the medical staff to ensure continued maintenance of a minimum level of quality of care. This surveillance typically consists of monitoring cases to assess any instances for patterns of poor quality of care as well as other indicators of difficulty such as being associated with a physician impaired with alcohol or drug or other abuse. Hospitals and their medical staffs also serve a regulatory role in reporting violations of clinical practice standards by physicians and other practitioners to state licensing agencies and other entities. Physicians, as members of the medical staff, may participate in various committee assignments and historically were expected to provide some level of indigent care although this requirement in many in- stances has largely dissipated. In most hospitals physicians are also expected to utilize their clinical privileges only in those areas in which they have proper training and credentialing. Physicians and other professionals who are less frequently utilizing a specific hospital may be
- 42. granted a separate category of privileges for occa- sional use with less expected participation and fewer responsibilities. Physicians who are inter- ested in clinical leadership positions may assume responsibility for medical staff committees or seek to be a leader in the medical staff hierarchy. In- creasingly, physicians who are interested in man- agerial roles may also be employed for that purpose by the hospital on the administration side, typically a position such as vice president for medical affairs. In addition to credentialing physicians for hos- pital privileges, the medical staff is typically re- sponsible for ensuring the quality of care provided in the hospital under delegated authority from the governing entity. Various committees may be formed for this purpose, including a quality assur- ance committee or other peer review committee. The medical staff will seek to provide feedback to physicians and other clinicians who are not meet- ing expected standards of the quality of care in their clinical practices within the institution. This feedback can take many forms, including quantita- tive data assessment comparing each individual to the norms of other practitioners in their specialties, or even informal feedback from the medical staff president or a clinical department chief. Ultimately, hospital privileges may be revoked in extreme situ- ations where clinical standards are clearly not met. In this instance, appropriate due process must be followed utilizing specified procedures as outlined in the medical staff bylaws. The increasing utilization of computerized infor- mation systems and a more interested younger gen- eration of clinicians have greatly accelerated the at-
- 43. tention to data-based assessments of quality of care. National voluntary organizations have worked hard to promote these efforts so as to elevate the overall quality of care provided in the nation’s hospitals. Voluntary accrediting agencies, in partic- ular, have also increasingly pressured institutional 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 193 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H O W A R D , T O N I - C L Y S
- 44. A 5 9 4 0 B U providers to incorporate quality assurance mecha- nisms in their ongoing production methods. Many types of approaches have been developed in this re- gard, including a range of processes designed to en- courage the use of clinical approaches that are vali- dated from scientific and evidence-based research. Many clinical quality assurance and quality im- provement techniques have been adapted from the corporate environment, particularly industrial set- tings as well. Payers are also demanding enhanced quality surveillance and improvement. In contrast to a typical corporate environment, hospitals do not directly employ most physicians, who are key decision makers and decide resource allocation and utilization. Thus, the medical staff serves an important role in aligning physician be- havior and objectives with institutional needs. Medical leadership is particularly important in today’s complex environment to facilitate this rela- tionship. Ultimately, the traditional hospital struc- ture, particularly with regard to the medical staff, is inconsistent with managing an organization that faces numerous competitive and pricing pressures. Some medical staff organizations, such as those
- 45. in group practice, model HMOs that directly own all resources in their systems, and certain govern- mental entities such as the military and veteran’s administration hospitals, have more direct control over the medical staff. KEY ISSUES FACING THE HOSPITAL INDUSTRY The hospital industry almost continuously faces key critical issues that challenge its structure, viability, and roles in health care. This section discusses many of these issues. Specialty Hospitals In recent years, the development of highly special- ized hospitals has gained considerable traction. Although not a new concept by any means, the more rapid recent development of these specialty hospitals poses a threat to community general hos- pitals to a much greater extent than in past years. The new specialty hospitals include those focused on cancer and heart disease and other highly dis- crete areas of practice in lucrative fields such as or- thopedic surgery. To further complicate the controversy over spe- cialty hospitals, these institutions are increasingly partially owned by the physicians who practice within them. Ironically, in the early days of the modern development of hospitals, physician own- ership was not unusual. However, the popularity of physician-owned proprietary hospitals today has been challenged by two ramifications. The first is
- 46. that these hospitals draw profitable patients from community hospitals, and the second potential conflict of interest is represented by physicians ad- mitting patients to hospitals in which they have an ownership interest. Of course, our quality of care data suggest that high volumes of discrete services can enhance qual- ity. From some perspectives, highly specialized in- stitutions may in fact provide the best care. On the other hand, many of these specialty hospitals may siphon off insured and relatively healthier patients, leaving the less profitable and more complicated cases to community general hospitals. Physician ownership of specialty hospitals raises concerns that financial incentives will affect the treatment decisions, such as the use of specialty and diagnostic services. In addition to providing care to the less complex and more profitable cases, these hospitals may also leave the uninsured and underinsured to community and public hospitals for treatment. The combination of adverse selection and less private insurance and public coverage for community general hospitals and government facil- ities does raise significant policy concerns. Federal policy development has been slow to respond to this trend. Medicare has complex rules regarding physician ownership of health care re- sources and potential conflicts of interest. And both the Medicare and Medicaid programs have a valid 194 PART THREE Providers of Health Services 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 194
- 47. Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H O W A R D , T O N I - C L Y S A 5 9 4 0 B U
- 48. CHAPTER 8 Hospitals and Health Systems 195 concern with respect to the distribution of health care costs across all facilities and patient groups. The impact of specialty hospitals on community general hospitals and governmental hospitals has yet to be fully assessed, but this development is po- tentially significant clinically and financially. Changes in Technology The hospital industry is all about technology. Al- though the hotel function of a hospital is in a way primary to its purpose, it is the provision of tech- nology that is its true mission. Technology has shaped the physical and operational structures of hospitals, has affected the lives of patients and fam- ilies, and has provided a delivery vehicle for physi- cians in clinical practice. From its earliest days as a modern institution, the availability of technological resources has defined the services provided in hospitals. The discovery of anesthesia and of antisepsis clearly established the early stages of the provision of surgical care. The vast array of imaging technologies has had tremen- dous impact on effective intervention for patients seeking care in the hospital setting. Laboratory, di- agnostic, and other technological innovations have also greatly facilitated clinical medicine. Successful intervention is dependent on the technology of in- novative therapies including pharmacological inter- ventions and surgical techniques.
- 49. More recently, the huge range of technological advancements that have vaulted to the forefront of the tertiary care role of inpatient services within hospitals have included organ transplantation, a vast array of minimally invasive surgical technolo- gies, advanced cardiac treatments, primarily through a variety of surgical interventions, an impressive range of successes in advanced emergency and trauma care, and vast improvements in the underly- ing technologies related to information systems, medical records, and other aspects of hospital and health care operations to facilitate the delivery of services to patients. Technological advances have af- fected obstetric patients, pediatric care needs, pa- tients with terminal illnesses, and a range of other problems that present to the inpatient side of hos- pital operations. Technological advancement has led to the devel- opment of increased specialization and clinical practice, expansion of specialized services, new medical and surgical specialties, and treatments for many diseases for which little curative or other care could be provided in the past. Advanced technolo- gies including the many applications of lasers, the use of ultrasonic technology for treatment, and more recently, the development of automated surgi- cal assistant or robot technologies have all been revolutionary. Hospitals operate in competitive markets and the pressure to provide a full range of technology, and to keep that technology current, yields signifi- cant cost pressures and even potential conflicts
- 50. with medical staff members. Insurers and employ- ers as well as government entities seek to pay for the latest technologies, but at efficient pricing. The continuing advancement of technology is a double-edged sword providing us with tremen- dous new capabilities, but at the same time, many challenges. The hospital, perhaps more than any other sector of the health care system, faces these opportunities and challenges in the most dramatic ways. And, ultimately, it is their customers, their patients, and their physicians who utilize these hospitals and health care systems, who have the highest expectations and often the least sensitivity about costs. Clinical Practice Patterns Hospital design and operations are significantly af- fected by accepted clinical patterns of practice. The increasing attention to best practices and practice norms of various types, particularly under quality assurance programs, requires institutional adher- ence to various protocols and guidelines. Informa- tion systems and other operational requirements must also be compliant with the need to provide evaluative information to assess and report on physician clinical patterns of practice. Medicare and many managed-care contracts require such 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 195 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T
- 51. U R N E R - H O W A R D , T O N I - C L Y S A 5 9 4 0 B U reporting. Accreditation by the Joint Commission for Accreditation of Health Care Organizations and
- 52. other specialty accreditation bodies also requires the availability and interpretation of data. In addition to the availability of appropriate information to monitor and evaluate clinical proto- cols and practice guidelines, institutions are in- creasingly expected to offer a governance structure that assigns responsibility for these activities. Typi- cally, in most community hospitals, that responsi- bility is delegated from the governing body to the medical staff. The governing board and institutional administration, however, retain responsibility for successful compliance with these requirements. Individual practitioners are likewise increasingly being held accountable for their practice patterns and behavior through a variety of monitoring and feedback mechanisms. The complexity of integrating all the require- ments pertaining to clinical practice is of itself a sig- nificant burden on institutional operations. Legal and ethical expectations, combined with reporting requirements contained in various contractual ar- rangements, further enhance the depth and com- plexity of this obligation. Physician independence has been significantly weakened by the introduc- tion of various external regulatory requirements. Reimbursement Mechanisms Hospitals and hospital systems are heavily con- strained by the reimbursement mechanisms that pay their bills. The most significant source of funds for most hospitals is the federal Medicare program. As discussed elsewhere in detail in this book, financial mechanisms for reimbursement
- 53. under the Medicare program have become in- creasingly complex. Medicare has moved to reward efficiency and specialization while increas- ingly squeezing institutional cash flow. Medicare, being a federal program, also has significant regu- latory and force of law powers unknown to third- party insurers in the private sector. Medicare has imposed an array of requirements to reduce fraud and abuse, but these efforts have had secondary effects in complicating organizational administra- tion and financial arrangements. Nongovernmental sources of payment, primarily from managed-care organizations, have themselves become fraught with complexity and cost pres- sures. Most payers now seek a competitive market advantage in pricing in an attempt to drive down the cost of health care, while at the same time shift- ing an increased burden of cost to the consumer. The negotiated per diem rates are heavily dis- counted and many insurers exclude a range of re- imbursements for various specific services. Many third parties also require reporting from institutional providers on utilization patterns, use of resources and services, and other parameters of the care process. Hospitals are generally expected by payers to provide extensive oversight of practi- tioners through aggressive credentialing efforts and other responsibilities. All these developments have resulted in pressure to improve efficiency, reduce waste and duplication, and provide care as quickly as possible and at the lowest possible cost.
- 54. While payers are increasingly squeezing pay- ments to all providers, hospitals in particular are susceptible to financial pressures. Hospitals pro- vide services that require a high degree of capital in- vestment, have limited control over the cost of many of their products due to such considerations as shortages of nursing and other specialized per- sonnel and the high cost of innovative products, and finally, the expectations on the part of both consumers and individual practitioners for reason- able ambience and excellent outcomes. Academic Medical Centers Academic medical centers typically consist of med- ical schools and their primary teaching hospitals. Academic medical centers provide tertiary, sec- ondary, and primary care but have a principal focus on biomedical research, teaching of medical resi- dents and medical students, and often an array of other professional training, research, and service ac- tivities. These organizations are highly complex 196 PART THREE Providers of Health Services 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 196 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R
- 55. - H O W A R D , T O N I - C L Y S A 5 9 4 0 B U CHAPTER 8 Hospitals and Health Systems 197 with a multitude of power structures, funding sources, and sometimes conflicting missions. Hospitals that are part of academic medical cen- ters are operationally constrained by the demands
- 56. of the teaching mission, particularly with regard to medical students and postgraduate medical educa- tion, and a mandate to conduct both basic biomed- ical and applied clinical research. Financial effi- ciency and consumer satisfaction are not typically the top priorities. Physicians and researchers place considerable demands on these organizations to provide the latest technology and staffing and to allow for teaching and clinical investigation. The success of academic medical centers in achieving their missions should be a national pri- ority. The long-term strengths and successes of our health care system depend on this. Although not necessarily widely acknowledged, financial effi- ciency in fact should probably not be a top priority from a national health policy perspective. Unfortu- nately reimbursement policies by Medicare and other government and private payers typically do not overtly allow enough latitude for academic med- ical centers. In addition, academic medical centers are frequently the providers of last resort, further re- straining cash flows and viability. Local government and, to an extent, private insurers through cost shifting, pick up part of the tab. A lot of attention has been directed toward academic medical centers in recent years. The chal- lenge is to reconcile the needs for medical education and research with the fiscal realities of available resources in a manner that will meet our nation’s educational and clinical needs. This remains a huge challenge for the nation’s health care system. SUMMARY
- 57. The hospital industry has faced numerous chal- lenges over the years and will continue to do so in the future. Markets have changed, pricing pres- sures have increased, and consumer and payer expectations have evolved. Yet, through it all, our nation’s hospitals have continued to provide the best hospital-based care in the world, delivering a technology that is second to none with top-notch staff dedicated to patient care. REVIEW QUESTIONS 1. Describe the historical development of hospitals in the United States. 2. Describe the differences between nonprofit and for-profit hospitals. 3. List the major trends that have occurred within the hospital sector. 4. What is horizontal integration, and why is it used? 5. What is vertical integration, and why is it used? 6. Describe the internal organization of community hospitals. 7. Describe the key issues facing the hospital industry. REFERENCES & ADDITIONAL READINGS
- 58. Birkmeyer, J. D., Siewers, A. E., Finlayson, E. V. A., Stukel, T. A., Lucas, F. L., Batista, I., Welch, H. G., & Wennberg, D. E. (2002). Hospital volume and surgical mortality in the United States. New England Journal of Medicine, 346, 1137–1144. Davis, M., & Heineke, J. (2003). Managing services: Using technology to create value. Boston: McGraw- Hill/Irwin. Gapenski, L. (2004). Healthcare finance: An introduction to accounting and financial management (3rd ed.). Chicago: AUPHA Press/Health Administration Press. Halm, E. A., Lee, C., & Chassin, M. R. (2000). How is volume related to quality in health care? A systematic review of the research literature. Prepared for National Academy of Sciences, Interpreting the volume-outcome relationship in the context of health care quality workshop. Washington, DC. Kelly, D. L. (2003). Applying quality management in healthcare: A process for Improvement. Chicago: AUPHA/Health Administration Press. Martin, L. L., & Sage, R. (Eds.). (1993). Total quality management in human service organizations. New York: Sage Publications. 12890_08_ch08_p182-197.qxd 8/10/07 12:12 PM Page 197 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T
- 60. Definition of Long-Term Care Clients of Long-Term Care How Long-Term Care Is Organized Service Categories Integrating Mechanisms Long-Term Care Policy LEARNING OBJECTIVES Upon completing this chapter, the reader should be able to 1. Describe who uses long-term care and under what circumstances. 2. Explain the role and scope of services included in long-term care. 3. Articulate how long-term care services are organized, operated, financed, and integrated. 4. Evaluate model delivery system approaches to long-term care for the future. 5. Articulate national policy issues pertinent to long-term care. 198 CHAPTER 9
- 61. The Continuum of Long-Term Care Connie J. Evashwick 12890_09_ch09_p198-219.qxd 8/14/07 12:13 PM Page 198 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H O W A R D , T O N I - C L Y S A
- 62. 5 9 4 0 B U WHAT IS LONG-TERM CARE? ■ A child with cerebral palsy attends a special needs classroom in a public school, with ther- apy available on-site, and her parents care for her when she is at home. ■ An 85-year old recovering from a broken hip receives meals on wheels during the week and relies on her daughter for meals over the weekend. ■ A young man with schizophrenia lives in shel- tered housing, with financial assistance provided through a public housing voucher program and medication or counseling assistance available from an on-site staff when needed. ■ An elderly couple, one of whom is blind from advanced glaucoma and one of whom is crippled with severe arthritis, uses a money- management service from a local community agency to pay their bills, since neither can write a check. ■ A middle-aged woman with multiple sclerosis has a live-in attendant to assist her with the
- 63. activities of daily living. All these are examples of long-term care pro- vided by formal or informal sources. Long-term care is defined as health, mental health, residen- tial or social support provided to a person with functional disabilities on an informal or formal basis over an extended period of time with the goal of maximizing the person’s independence. Services change over time as the person’s and caregivers’ needs change. The goal of long-term care is to help people achieve functional independence, in contrast to the goal of acute care, which is to cure. People of all ages and a wide range of clinical diagnoses need long-term care. The vast majority of long-term care (80 to 90 percent) is provided by friends and fam- ily. However, formal services are essential to enable the informal system to be sustained. The formal ser- vices that provide long-term care are described in this chapter using a conceptual framework referred to as “the continuum of long-term care.” The ideal is an integrated set of services that provides continu- ity of care over time and across settings. In reality, services are highly fragmented due to financial drivers, local community variation, and a lack of uniform federal and state policies. This chapter pro- vides an overview of the ideal continuum of care juxtaposed with the reality of existing services, structure, and policies. WHO NEEDS LONG-TERM CARE?
- 64. The clients of long-term care are growing rapidly. They represent a mosaic of population segments of those with functional disabilities. Three intersecting concepts warrant explanation to understand the users of long-term care. The fundamental reason that a person needs long-term care is because they suffer from one or more functional disabilities. Functional ability is a person’s ability to perform the basic activities of daily living (ADLs) or instrumental activities of daily living (IADLs). ADLs include the ability to bathe, dress, perform personal care and grooming, walk, transfer from bed to chair, maintain bowel and bladder continence, and eat. ADLs were initially de- fined by Katz and colleagues through research (Katz et al., 1963), and years of study have produced com- monly accepted measures and scales of functioning. ADLs tend to involve large motor skills, and they are lost in a predictable order. IADLs are more loosely defined (Lawton & Brody, 1969) but typically involve cognitive reasoning and finer motor skills. IADLs include telephoning, managing money, tak- ing medications, grocery shopping, housekeeping, doing chores, and using transportation. The conditions that underlie the need for long- term care may be physical health, mental health, CHAPTER 9 The Continuum of Long-Term Care 199 12890_09_ch09_p198-219.qxd 8/14/07 12:13 PM Page 199 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part.
- 65. T U R N E R - H O W A R D , T O N I - C L Y S A 5 9 4 0 B U or a combination, as well as family situation and
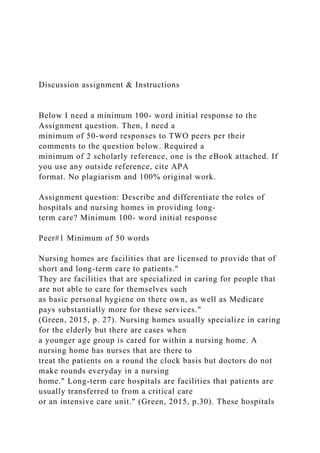
- 66. environmental context. Of the 288 million people in the United States in 2005, more than 12 percent, or more than 35 million people suffered from some type of disability that limited their ability to per- form basic activities of daily living (National Center for Health Statistics, 2005). Limitations in func- tional ability affect people of all ages but increase with age and the concomitant chronic conditions that accumulate with aging. Figure 9.1 shows the estimated number of people with disabilities. How a person manages a functional disability depends on several factors, including other health condi- tions, age, family and social support, economic sta- tus, housing, and personal preference. Chronic is defined by the National Health Inter- view Survey as any condition that lasts 3 months (or 90 days) or more (National Center for Health Statistics, 2007). Chronic conditions may derive from physical or mental conditions. Over the progression of a disease, both may occur. Chronic conditions may be as life-threatening as coronary artery disease or as harmless as mild arthritis. In 2005, an estimated 133 million people had some type of chronic condition (Hoffman, Rice, & Sung, 1996). Chronic conditions often (although not al- ways) result in functional disabilities. An impairment as used by the National Health Interview Survey is defined as “a chronic or perma- nent defect, usually static in nature, that results from disease, injury, or congenital malformation. It often represents a decrease in or loss of ability to perform various functions.” Permanent impair- ments, such as limb amputation or blindness, may
- 67. require an initial adjustment and are then more or less stable. People may attain a level of indepen- dence by learning special skills to overcome the dis- ability or by using adaptive devices. For example, a person with myopia can have their vision corrected by wearing glasses or contact lenses and thus suffer 200 PART THREE Providers of Health Services 0 20 40 60 80 Under 15 25– 44 55– 64 70 –74 80� 57.6% 38% 57.7% 28.3% 46.6% 30.7% 44.9% 24.2% 35.7% 13.9% 22.6%
- 68. 8.1% 13.4% 5.3% 10.7% 3.8% 7.8% 73.6% Severe Disability Any Disability Figure 9.1. DDiissaabbiilliittyy PPrreevvaalleennccee bbyy AAggee,, 11999977 SOURCE: From Health, United States, 2005 (Special Excerpt), Trend Tables on 65 and Older Population (DHHS Pub. No. 2006-0152) (Table 58, p. 243), National Center for Health Statistics. 12890_09_ch09_p198-219.qxd 8/14/07 12:13 PM Page 200 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H
- 69. O W A R D , T O N I - C L Y S A 5 9 4 0 B U no disability as a result of their impairment. Nonetheless, impairments are closely associated with functional disability. Impairment, chronic condition, and functional ability are intertwined. For example, a person who is blind, who lives with a supportive family, learns Braille, and masters the immediate environment, may achieve a fair degree of independence on a
- 70. daily basis. However, if that person ages and be- comes cognitively diminished, he or she may no longer be able to remember the environment, and without the ability to use the visual clues (or just simple notes or lists) that a person with sight can use to help overcome cognitive weaknesses, is less able to function independently. If that person then slips and breaks a hip, suffers a permanent impair- ment, and has to use a walker, they will lose more functional ability than a sighted person or a person without cognitive impairment who is able to un- derstand rehabilitation routines. In addition to a person’s health and mental health, social situation, finances, housing, and community context all affect the extent to which a person can perform ADLs and IADLs indepen- dently and the type of assistance they may need. Contrast a male veteran in a wheelchair who lives with a spouse, can afford a personal caregiver, re- sides in a one-story home, and lives in a large urban community served by a community-based agency coordinating services for the disabled and a Veterans Affairs hospital that provides a full range of health care for people with disabilities with an elderly widow who breaks her hip, has no family nearby, has no income except Social Secu- rity, resides in a two-story walk-up in a small rural town, and must travel 30 miles to reach a hospital with an orthopedic service. The man will main- tain his independence by working with a multi- faceted support system; the older woman will most likely end up moving to a relative’s home or an assisted living facility for those with low income and be forced to move away from her friendship network.
- 71. The United States makes no single, constant, routine count of people needing long-term care that factors in all the variables that determine if, what type, and how much care a person needs to perform ADLs and IADLs. Rather, subsets are counted, and each subset of the total population has a segment that may require long-term care at some point from formal or informal sources. Pop- ulation segments at high risk of needing long- term care are growing steadily. They include the aged (especially those age 75 and older), those with certain chronic conditions (such as stroke, mental illness, degenerative neurological condi- tions, Alzheimer’s disease), people positive for HIV/AIDS, and children with special health care needs, to mention just a few. For each group, and each individual, the care needed will vary and will be some combination of informal care provided by family and friends and formal care provided by external organizations. The rationale for structur- ing the long-term care system for specific seg- ments of the population rather than a single en- compassing system is based on the differing needs of each segment and the multiple factors that shape service delivery, particularly financing. Users of long-term care services are called by dif- fering terms, depending on the service. Table 9.1 shows the terms used by various services. CHAPTER 9 The Continuum of Long-Term Care 201 Table 9.1. TTee rrmmiinnoollooggyy ffoorr UUsseerrss ooff SSeelleecctt SSeerrvv ii cc ee ss
- 72. SS ee rrvv ii cc ee TTee rrmm ffoorr CClliieennttss Nursing homes Residents Hospitals Patients Adult day services Participants Home care Clients Hospice Patients Outreach Consumers Wellness programs Clients Disease management programs Enrollees Durable medical equipment Customers Assisted living Residents 12890_09_ch09_p198-219.qxd 8/14/07 12:13 PM Page 201 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H O W A R D , T O
- 73. N I - C L Y S A 5 9 4 0 B U HOW IS LONG-TERM CARE ORGANIZED? One of the greatest challenges of long-term care is that there is no single organized formal delivery sys- tem. As noted earlier, the vast majority of long-term care is provided by friends and family. Care is orchestrated around the unique needs of each indi- vidual and family, as well as the resources of the par- ticular community. A person may require multiple services, provided in a range of settings, and by pro- fessionals representing a broad spectrum of disci- plines. Moreover, services can be expected to change over time as the client’s and family’s needs change or as new technologies arise. Thus patterns of care vary, for population segments as well as individuals. To analyze long-term care service delivery, the
- 74. conceptual framework of an ideal continuum of long-term care is used. The continuum of care is defined as A client-oriented system composed of both services and integrating mechanisms that guides and tracks clients over time through a comprehensive array of health, mental health, and social services spanning all lev- els of intensity of care. (Evashwick, 1987) The ideal continuum of care is the formal care system that complements the informal services pro- vided by friends and family. The ideal continuum of care is a comprehensive, coordinated system of care designed to meet the multifaceted needs of persons with complex and/or ongoing problems efficiently and effectively. A continuum is more than a collec- tion of fragmented services. It includes mechanisms for organizing those services and operating them as an integrated system. The purpose is to facilitate the client’s access to the appropriate services at the appropriate time, quickly and efficiently. Ideally, a continuum of care does the following: ■ Matches resources to the client’s health and fam- ily circumstance. ■ Monitors the client’s condition and changes ser- vices as needs change. ■ Coordinates the care of many professionals and disciplines.
- 75. ■ Integrates care provided in a range of settings. ■ Enhances efficiency, reduces duplication, and streamlines client flow. ■ Pools or otherwise arranges financing so that services are based on need rather than narrow eligibility criteria. ■ Maintains a comprehensive record incorporating clinical, financial, and utilization data. A true continuum should serve three major goals: (1) Provide the health and related support services that foster independence, for the client as well as the family, (2) achieve cost-effectiveness by maximizing the use of resources, and (3) enhance quality through appropriateness and continuity of care. Some clients may use only select components of the system and may remain involved with the or- ganized system of care for a relatively short period of time; others may use only a limited and stable set of services over a prolonged period of time. Continuum Overview More than 60 distinct services can be identified in the complete continuum of care. For simplicity, the services are grouped into seven categories, as shown in the schematic and in Table 9.2. The seven categories represent the basic types of health care and related services that a person could need over time, through periods of both wellness and illness. Table 9.2 lists select services within each category but should not be interpreted as the complete list of all health and mental health services. The table
- 76. does not include social support services, which also comprise a lengthy list. By definition, the continuum of care is more than a collection of fragmented services; it is an in- tegrated system of care. The United States health care delivery system has evolved historically as highly fragmented. Integration of services does not happen automatically. For providers, payers, and clients to gain the system benefits of efficiencies of 202 PART THREE Providers of Health Services 12890_09_ch09_p198-219.qxd 8/14/07 12:13 PM Page 202 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H O W A R D , T O N
- 77. I - C L Y S A 5 9 4 0 B U CHAPTER 9 The Continuum of Long-Term Care 203 Table 9.2. CCaatteeggoorriieess aanndd SSeerrvviicceess ooff tthhee CCoonnttiinnuuuumm ooff CCaarree** Extended Skilled nursing facility Step-down unit Swing bed Nursing home follow-up Intermediate care facility for the mentally retarded Long-term care hospital Psychiatric hospital (residential model) Acute Medical/surgical inpatient services Psychiatric acute inpatient services Rehabilitation short-term inpatient services Interdisciplinary assessment team
- 78. Consultation service Ambulatory Physician’s office Outpatient clinics ■ Primary care ■ Specialty medical care ■ Rehabilitation ■ Mental health ■ Surgery Psychological counseling Day hospital Adult day services Home Care Home health—Medicare Home health—Private Hospice High-technology home therapy Durable medical equipment Home visitors Homemaker and personal care In-home caregiver Outreach and Linkage Screening Information and referral Telephone contact Emergency response system Transportation Senior services program Meals on Wheels Mail order pharmacy Wellness and Health Promotion Educational programs
- 79. Exercise programs Recreational and social groups Senior volunteers Congregate meals Support groups Disease management Housing Continuing care retirement community Independent senior housing Assisted living Congregate care facility Adult family home Group home Board and care facility Alcohol and substance abused facility *Lists of services within each category are not exhaustive. From “Definition of the Continuum of Care,” by C. Evashwick, 2005, in The Continuum of Long-Term Care, C. Evashwick (Ed.), Albany, NY: Delmar. 12890_09_ch09_p198-219.qxd 8/14/07 12:13 PM Page 203 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H
- 80. O W A R D , T O N I - C L Y S A 5 9 4 0 B U operation, smooth client flow, and quality of ser- vice, formal structural integrating mechanisms are essential. Four integrating management systems are required: inter-entity structure and management, care coordination, integrated information systems, and integrated financing (Figure 9.2). SERVICE CATEGORIES
- 81. This section briefly describes each of the seven ser- vice categories and presents data, when available, on major or select services within each category. Not every client will use every service. However, the ideal is that the services are available and accessible if a person should need them. There is no set order for the services, since each client will use ones ap- propriate for his or her individual and unique needs. A significant aspect of the services is that each has its own operating characteristics, even within the same category. Services vary according to inten- sity of care offered, professional and support staffing, predominant financing, licensing, certifica- tion, accreditation, equipment, space, and signifi- cant other management dimensions. This variation poses a challenge to managers trying to coordinate services, as well as to payers and clients who are trying to achieve continuity of care. Extended Inpatient Care Extended inpatient care is for people who are so sick or functionally disabled that they require on- going nursing and support services provided in a formal health care institution, but who are not so acutely ill that they require the technological and professional intensity of a hospital. The majority of extended inpatient care facilities are referred to “nursing facilities” or “nursing homes,” although this is a broad term that includes many levels and types of programs. Specialty facilities range from subacute units in hospitals to intermediate care fa- cilities for the mentally retarded or developmentally
- 82. 204 PART THREE Providers of Health Services INTER-ENTITY STRUCTURE AND MANAGEMENT CARE COORDINATION INTEGRATED INFORMATION SYSTEMS INTEGRATED FINANCING AMBULATORY ACUTE HOME OUTREACH WELLNESS HOUSING EXTENDED Figure 9.2. SS ee rrvviicceess aanndd IInntteeggrraattiinngg MMeecchhaanniissmmss ooff tthhee CCoonnttiinnuuuumm ooff CCaarree SOURCE: From “Definition of the Continuum of Care.” by C.
- 83. Evashwick, 1987, in Managing the Continuum of Care, by C. Evashwick and L. Weiss (Eds.), Gaithersburg, MD: Aspen Publishers. 12890_09_ch09_p198-219.qxd 8/14/07 12:13 PM Page 204 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H O W A R D , T O N I - C L Y S A 5
- 84. 9 4 0 B U disabled to psychiatric hospitals caring for the severely mentally ill on an indefinite basis. Nursing facilities in the nation number about 16,100, with about 1.4 million residents at any given time (American Association of Homes and Services for the Aging, 2007). The cost of a nursing facility ranges from $4,000–7,000 per month, depending on location and scope of services rendered. Medicaid pays for about 47 percent of all nursing facility care, and residents and their families pay for about one-third (Center for Medicare and Medicaid Services, 2007). The lifetime probability of ever being admitted to a nursing home (under the present U.S. standard of care) is about 50 percent. However, average length of stay has decreased dramatically over the past 30 years, just as likelihood of admission has increased. Both reflect the trend for nursing facili- ties to become technologically more sophisticated and to function as short-term stopping places in be- tween home and hospital rather than as permanent residential settings. Nursing facilities can be accredited by the Joint Commission and can be certified by Medicare and Medicaid to participate as providers to those en-
- 85. rolled in these government programs. Two excellent sources of information about nurs- ing home are the trade associations that represent for-profit and not-for-profit nursing homes, respec- tively: http://www.ahca.org, http://www.aahsa.org, and the Federal Centers for Medicare and Medicaid Services, http://cms.nhs.gov Hospitals The nation’s hospitals are a broad array of institu- tions that provide care for those with acute prob- lems and emergencies, but that also care for many people with chronic conditions and long-term health problems. The most current information can be found on the website of the American Hospital Association at http://www.aha.org. Community general hospitals are the most preva- lent type, numbering about 4,936 of the 5,756 total U.S. hospitals existing in 2005 (American Hospital Association, 2007a). However, various types of hospitals specialize in long-term care, in- cluding categories of psychiatric, rehabilitation, chronic disease, orthopedics, and long-term (de- fined as average length of stay of 23 days or more). Hospitals also provide extensive outpatient services, including many used by those needing long-term care, ranging from rehabilitation to mental health counseling to outpatient surgery. Hospitals have evolved from a focus on strictly acute care to promoting health with disease man- agement and health education programs. Hospitals admit more than 37 million people
- 86. each year, but this number includes those who are readmitted who are those most likely to be long- term care users. Average length of stay is 4 to 5 days for adults under the age of 65 and about 6 days for those age 65 and older. The leading causes of hospital admissions are chronic condi- tions: heart problems, cancer, mental illness, stroke, respiratory conditions, and fractures derived from osteoporosis. Medicare and private insurance are the primary payers for hospital services, with individuals paying relatively little from out-of-pocket. However, hospi- tal costs are the largest single category of expendi- ture for Medicare, other government health pro- grams, and private insurance. Hospitals are accredited by the Joint Commission. Ambulatory Care Ambulatory care services are provided in a formal health care facility, whether a physician’s office or the outpatient clinic of a hospital or an adult day pro- gram. They include a wide spectrum of preventive, maintenance, diagnostic, and recuperative services for people who manifest a variety of conditions— from those who are entirely healthy and simply want an annual checkup to those with major health problems who are recovering from hospitalization to those with chronic conditions who need ongo- ing monitoring. Outpatient visits to hospitals alone numbered nearly 600 million in 2005 (American Hospital Association, 2007b). CHAPTER 9 The Continuum of Long-Term Care 205
- 87. 12890_09_ch09_p198-219.qxd 8/14/07 12:13 PM Page 205 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E R - H O W A R D , T O N I - C L Y S A 5 9 4 0 B
- 88. U Adult day services (ADS) are particularly rele- vant to long-term care. ADS represent a daytime program of personal care, therapeutic activities, su- pervision, socialization, assistance with ADLs, midday meals, and perhaps health-related skilled care. ADS enable frail people who cannot be alone in their own homes to remain in the community. By attending adult day services, people who are functionally disabled due to physical or mental dis- orders and/or are moderately ill but not in need of round-the-clock nursing care can remain in their homes at night with their families or friends while receiving the care they need during the day. ADS participants may attend on an indefinite basis or just while recovering from an acute episode of ill- ness. They may attend each day, or just 2 or 3 days per week. The goals are to foster the maximum possible health and independence in functioning for each participant and to provide respite and support for each caregiver and family. For many, ADS programs provide an alternative to nursing home care. ADS programs have grown exponentially since the first formal programs began in the 1970s. Cur- rently, there are about 3,400 ADS programs throughout the nation (Cox, 2006). The average daily census is about 25, but capacity ranges up to 38 or more people, with about three times as many people enrolled as attend on any given day. This means that ADS serve about 85,000 people per day. More than 150,000 people throughout the
- 89. United States are enrolled in ADS at any given time (National Adult Day Services Association, 2007). ADS average daily charges were about $56 per day in 2007, but relatively few programs make a profit. Most depend on donations, grants, and other subsidies. Medicare does not pay for ADS; Medicaid pays in selective states, and many individ- uals pay out-of-pocket. Licensure varies across states. Some states li- cense ADS as a health service; some license it as a social service. ADS can be accredited by the Com- mission on Accreditation of Rehabilitation Facili- ties (CARF). ADS are still gaining recognition by professionals and lay people alike. A key source of information about adult day services is the National Association for Adult Day Services at http://www.aahsa.org/naads. Home Health Home health care is one of the oldest components of the continuum of care. A number of home health agencies across the nation have celebrated their cen- tennials. Home care today consists of several types of services: skilled nursing care and therapies; home- maker/personal care/chore services; high-technology home therapy; durable medical equipment; and hos- pice.The services may all be provided by one agency, or an agency may specialize in only one. Each service has distinct operating characteristics. Home health agencies certified by Medicare must serve people who are homebound, have a progno-
- 90. sis of improvement/recovery; have home care or- dered by a physician; need skilled nursing, physical therapy, or speech-language therapy; require inter- mittent care only; and meet conditions of participa- tion specified by the federal Medicare legislation. These home care agencies offer skilled services pro- vided by registered nurses, physical therapists, oc- cupational therapists, speech therapists, social workers, and home health aides. They do not pro- vide personal care or functional support on an in- definite basis. Nearly 3 million people are served by Medicare-certified home care agencies each year (National Association of Home Care, 2007). Medicare-certified home health agencies num- bered about 7,628 in 2004 (National Association for Home Care, 2007). Home health agencies may be freestanding or owned by hospitals, health de- partments, assisted living complexes, or other com- munity agencies. Nearly one-half are for profit; the others are not-for-profit or government affiliated.The national average payments in 2004 were $129 per visit and $4,050 per patient. Medicare is the largest single payer, although many managed-care and commercial insurers also pay for home care pro- vided by Medicare-certified agencies. Medicare cer- tified home health agencies may be accredited by the Joint Commission or the Community Health 206 PART THREE Providers of Health Services 12890_09_ch09_p198-219.qxd 8/14/07 12:13 PM Page 206 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part.
- 91. T U R N E R - H O W A R D , T O N I - C L Y S A 5 9 4 0 B U Accreditation Program (CHAP). Detailed informa-
- 92. tion can be found from the National Association for Home Care and Hospice at http://www.nahc.org and from Medicare at http://cms.gov. Private home care agencies are not certified by Medicare and are thus not restricted by federal regu- lations. Consequently, they provide a broader spec- trum of home services ranging from highly skilled to basic personal support, homemaker, and chore ser- vices. Private home care agencies bill by the hour or the service. Many individuals pay privately. In addi- tion, private home care agencies may have contracts with managed-care plans, commercial insurers, Medicaid, or other local government agencies. Statistics on private home care agencies are limited. Private agencies are estimated to number more than 12,000 and to care for more than 5 million people per year. The largest association representing both Medicare-certified and private home care agencies is the National Association for Home Care, which can be accessed at http://www.nahc.org. High-tech home therapy refers to specialty care provided in the home that requires sophisticated equipment and pharmaceuticals. Examples are chemotherapy, antibiotic therapy, enteral and par- enteral nutrition, and home dialysis. High-tech home therapy may be provided by a Medicare-certified or private home care agency or by a company that spe- cializes only in high-tech home care. This service is mentioned separately because it has grown expo- nentially over the past 30 years and is expected to continue to do so as therapies are moved from in- patient to outpatient venues. Also, high-tech home care requires additional licenses, personnel, and pay- ment mechanisms from those required of standard
- 93. home care agencies because of the pharmaceuticals and equipment involved, as well as the high level of intensity of illness of the clients. Hospice Hospice is a philosophical approach to care rather than a place. Ideally, hospice care occurs in the per- son’s home, including in a nursing home, assisted living complex, or other group residential setting. Hospice is a concept of comprehensive and pallia- tive care for someone whose death is imminent. The goals are to make the person as comfortable as possible, including using drugs to alleviate pain; achieve emotional acceptance of death by the per- son and the family; and comfort and assist the fam- ily after the person’s death. Hospice uses an inter- disciplinary team, including pastoral care and bereavement counselors. The concept of hospice was developed in Great Britain by Dr. Cicely Saunders. The first hospice in the United States opened in 1971. Hospice can be organized independently or from the base of any health care entity, including home health agencies. Medicare has a special hospice provision. This en- tails detailed regulations for those organizations that seek to be certified Medicare hospice providers, a complex payment system, and certain expectations of and benefits for enrollees. Commercial insurance companies and Medicaid have tended to mirror the Medicare benefit in covering hospice care. For a per- son to enroll in hospice, he or she must be eligible for Medicare and have a projected life expectancy of 180 days or less. Both the Joint Commission and
- 94. CHAP accredit hospice programs. The number of hospices and hospice patients has grown steadily over the past 35 years. In 2007, there were 3,078 hospices certified by Medicare and numerous others that did not seek certification (Hospice Association of America, 2007). The Medi- care hospices served more than 890,000 people in 2005, or more than one-third of all those who die during the year. The median length of stay in hos- pice was less than 21 days in 2006, indicating that many people do not get the benefits of hospice as early as they might. Detailed information about hospice can be found at http://www.nahc.org, http://www.cms .gov, and http://hhpco.org. Durable Medical Equipment Durable medical equipment (DME) is equipment that enables a person to accommodate a disability and maintain independence. DME encompasses a CHAPTER 9 The Continuum of Long-Term Care 207 12890_09_ch09_p198-219.qxd 8/14/07 12:13 PM Page 207 Copyright 2008 Cengage Learning, Inc. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. T U R N E
- 95. R - H O W A R D , T O N I - C L Y S A 5 9 4 0 B U wide range of devices, from simple walkers and canes to sophisticated wheelchairs and beds. DME is paid for by Medicare, Medicaid, and private in- surance under conditions specified by each insurer. It may be rented or purchased, depending on the insurer, the person’s condition, and whether the
- 96. need for the equipment is expected to be short-term or indefinite. Companies that provide DME are dis- tinct from other health care agencies, but home health agencies will often assist in arranging for DME that is needed by a person to remain in his or her own home while receiving home care services. DME is an important component of the continuum of care because it enables people with disabilities who might otherwise be dependent on others for assistance to maintain their independence. Detailed information about Medicare’s DME provisions can be found at http://cms.gov/center/dme.asp. Outreach Outreach programs make health and social services readily available in the community rather than within the formidable walls of a large institution. Health fairs at community events, senior member- ship programs, emergency response systems, nurse practitioners stationed by health care systems in se- nior housing complexes, and vans for transporta- tion to medical appointments are all forms of out- reach. They are targeted at those who are living in the community for the purpose of keeping them connected with the health care system. Many outreach programs are provided at no or low charge to the consumer. They may be paid for by a hospital, medical group, managed care com- pany, or other health care organization as a com- munity benefit or a loss leader to market other ser- vices. Regardless of the purpose, clients identified through outreach activities should ideally be linked back to the organization’s core businesses for pur- poses of continuity of care.
- 97. Wellness Wellness programs span a wide spectrum from ac- tivities provided for those who are basically healthy and want to stay that way by actively engaging in health promotion to disease management for those with chronic illnesses who want to remain as healthy as possible. Wellness programs include health education classes, exercise programs, health screenings, and disease management regimes of- fered at health care sites or to be used at home. Wellness activities may be provided at no or low charge to the client. With a few notable exceptions, wellness activities are not paid for by third-party payers. They tend to be provided free of charge as a public relations tool or because the organization of- fering the activity appreciates that they will save money on providing care if they can help someone stay healthy. Disease management (DM) programs have be- come pervasive and sophisticated in recent years. They are one method for empowering consumers who have diagnosed health problems to control their condition so they do not become severely ill. DM programs may also be structured so that they are a means of facilitating clients with access to the services clients need, when they need them. Health plans and medical groups have been prominent proponents of disease management and often bear the costs. Housing