Model Call Girl in Subhash Nagar Delhi reach out to us at 🔝9953056974🔝
Eliminate Avoidable Blindness by 2020
1. 20
200
2000
20000
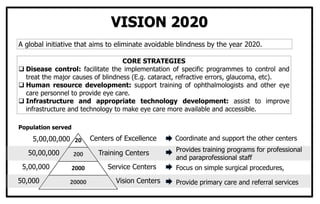
VISION 2020
A global initiative that aims to eliminate avoidable blindness by the year 2020.
CORE STRATEGIES
Disease control: facilitate the implementation of specific programmes to control and
treat the major causes of blindness (E.g. cataract, refractive errors, glaucoma, etc).
Human resource development: support training of ophthalmologists and other eye
care personnel to provide eye care.
Infrastructure and appropriate technology development: assist to improve
infrastructure and technology to make eye care more available and accessible.
Centers of Excellence
Training Centers
Service Centers
Vision Centers
50,000
5,00,000
50,00,000
5,00,00,000 Coordinate and support the other centers
Provides training programs for professional
and paraprofessional staff
Focus on simple surgical procedures,
Provide primary care and referral services
Population served
2. FEATURES
• Cash assistance linked to institutional delivery
• Encourages Small Family Norms
• Encourages Pregnant Women to Undergo
Tubectomy
• Trained TBA (ASHA) is the Effective Link Between
Field Level Health Functionary & the BPL Woman
• Payment Of Incentive to Dai/ASHA
• Fund Released Through State SCOVAS/State
Dept of Family Welfare
JANANI SURAKSHA YOJNA
Category of states
Rural Area Urban area
Assistance
package to
mother
Package for
the accredited
worker
Total
Assistance
package to
mother
Package for
the
accredited
worker
Total
Low performing states* Rs. 700 Rs. 600 Rs. 1300 Rs. 600 Rs. 200 Rs. 800
High performing states Rs. 700 Nil Rs. 700 - - -
Vision
To reduce over all Maternal Mortality Ratio
and Infant mortality Rate (IMR)
To increase institutional deliveries in BPL
families.
Target Group
All pregnant women belonging to the BPL
households and of the age of 19 years or
above
Up to two live births.
*- Uttar Pradesh, Uttaranchal, Bihar, Jharkhand, Madhya Pradesh, Chhattisgarh, Assam, Rajasthan, Orissa & Jammu & Kashmir
Source: http://nrhm.nic.in
3. Vaccine Age
Birth 6 wks 10 wks 14 wks 9-12 months
Primary Vaccination
BCG
OPV
DPT
Hepatitis B
Measles
Booster doses
DPT +OPV 16 to 24 months
DT 5 years
TT At 10 years and again at 16 years
Vitamin A 9, 18, 24, 30 and 36 months
Antenatal
2 doses of TT (1st dose of TT at the time of
registration and the 2nd dose 1 month later)
Age
Less than
5 years
More than
5 yrs
1st visit
BCG,
OPV,DPT,
Hepatitis B
TT
Hepatitis B
2nd visit
(1 month later)
OPV, DPT,
Hepatitis B
TT
Hepatitis B
3rd visit
(1 month later)
OPV, DPT
1 yr later
OPV, DPT,
Hepatitis B
Hepatitis B
BCG - Bacille Calmette Guerin
DPT - Diphtheria, Pertussis & Tetanus
OPV - Oral Polio vaccine
TT - Tetanus toxoid
4. HEALTH & BEHAVIOUR RELATED PROBLEMS
AMONG ADOLESCENTS
Specific to Adolescents
• Disorders of secondary sexual development
• Difficulties in psychosocial development
• Suboptimal adolescent growth spurt
Affecting Adolescents
Disproportionately
• Maternal mortality & morbidity
• STD ( including HIV)
• Tuberculosis
• Schishtosomiasis
• Intestinal helminths
• Mental disorders
Affecting Adolescents less than
children; but more than adults
• Malnutrition
• Malaria
• Gastroenteritis
• Acute respiratory infections
Manifested in adolescence originating
in childhood
• Chagas disease
• Rheumatic heart disease
• Poliomyelitis
With major implication for Future
health
• STD (including HIV)
• Leprosy
• Dental
Behavioural
• Alcohol abuse
• Other substance abuse
• Injuries
• Tobacco use
• Poor diet
• Lack of exercise
• Unsafe sexual practices
Source: Adolescent Care 2000 and beyond
5. ADULTERATION OF FOOD
Food Material Common Adulterants
Cereals such as
wheat, rice Mud, grit, Soapstone bits
Dals Coaltar dyes, Khesari dal
Haldi (Turmeric)
powder Lead chromate powder
Dhania powder Starch, Cow dung or
horse dung powder
Black pepper Dried seeds of papaya
Chilli powder Saw dust, Brick powder
Tea dust/
Leaves
Black gram husk,
Tamarind seed powder,
Saw dust, Used Tea dust
Coffee powder Date husk, Tamarind
husk, Chicory
Food Material Common Adulterants
Asafoetida (Hing) Sand, Grit, Resins, Gums
Mustard seeds Seeds of prickly poppy –
Argemone
Edible oils Mineral oils, Argemone
oil
Butter Starch, Animal fat
Ice cream Cellulose, Starch, Non
permitted colours
Sweet meats Non permitted colours
Fresh green peas
in packing Green dye
Milk Extraction of fat, Addition
of starch & water
Ghee Vanaspati
6. THE UN CONVENTION ON THE RIGHTS OF THE CHILD
Non Discrimination
• Civil Rights & Freedom
• Name & Nationality
• Identity
• Freedom of Expression
• Freedom of Thought,
Conscience & Religion
• Freedom of Association
• Protection of Privacy
Best Interests of the child
• Family, Environment &
Alternative care
• Parental guidance &
Responsibilities
• Separation from Parents
• Protection of children
without families
• Adoption
• Protection from Abuse &
Neglect
• Education, Leisure &
Cultural Activities
• Standard of Living
Source: Child Rights and Health, WHO
Rights to Survival &
Development
• Armed Conflict
• Refugees
• Child Labour
• Drug Abuse
• Discrimination
• Children of Minorities
• Sexual & Other
Exploitation
• Sale, Trafficking &
Abduction
• Torture & Deprivation of
Liberty
• Juvenile Justice
• Rehabilitative Care
Views of the Child
• Basic Health & Welfare
• Survival & Development
• Health & Health services
• Handicapped Children
• Social Security
7. THE BABY FRIENDLY HOSPITAL INITIATIVE
1. Have a Written Breastfeeding Policy
2. Train All Health Staff to implement this policy
3. Inform all Pregnant women about the benefits of Breastfeeding
4. Help Mothers Initiate Breastfeeding within half an hour of birth
5. Show Mothers the Best Way to Breastfeed
6. Give Newborn Infants No Food or Drink other than Breast milk unless
medically indicated
7. Practice ‘Rooming In’ by allowing mothers and babies to Remain Together
24 hours a day
8. Encourage Breastfeeding ‘On Demand’
9. Give No Artificial Teats, Pacifiers, Dummies or Soothers
10. Help Start Breastfeeding Support Groups and Refer mothers to them
8. CYCLE OF INTERGENERATIONAL INFLUENCE OF
NUTRITION
Nutritional Status of
Women of Child Bearing Age
Nutritional Status of
Lactating Woman
Nutritional Status of
Neonates and Infants
Girl’s s nutritional
status
Nutritional status
at puberty
Nutritional Status of
Pregnant Woman
9. CANCER CERVIX- HPV VACCINE
1. It is the most common cancer in
Indian women.
2. Over 90% of these cancers are
diagnosed at advanced stages..
3. Human Papilloma virus (HPV )
infection is the primary risk
factor
4. HPV types 16 and 18 cause
70% of cervical cancers and HPV
6 and 11 cause 90% of the
warts.
5. A quadrivalent HPV vaccine is
currently available
6. CDC recommendation: All
females age 11–12 years (or
13-26 yrs if not previously
vaccinate) be vaccinated with
3 doses of HPV vaccine.
7. Following the first dose, the
vaccine is administered at two
and six months
8. Efficacy: 100% for five years,
in preventing cervical
precancers, vulvar and vaginal
precancers, and genital warts
caused by the four vaccine
types.
10. PARTICIPATORY LEARNING FOR ACTION (PLA)
FOR COMMUNITY HEALTH DEVELOPMENT
PLA embraces a series of techniques, many of them recently developed in India, for using local
people’s knowledge and skills to learn about local conditions, identifying local development
problems and plan responses to them. - Richard Heaver (1991)
VISUAL TOOLS
Participatory Mapping
Institutional Programming
(Venn Diagram)
Seasonal Diagram
Daily activity Chart
Trend Analysis
Body Mapping
Pair wise Ranking
Force Field Analysis
Causal Impact Diagram
Impact Evaluation
OBSERVATIONAL
TOOLS
Participant Observation
– DIY, taking part in
local activities
Transect Walks
BASKET OF PLA TOOLS
AND TECHNIQUES
DISCUSSION TOOLS
Focus Group Discussion
Semi- Structured
Interviews
BENEFITS OF PLA
1. Generates rapport and forces outsiders to
learn, listen and understand
2. Local people’s knowledge of local conditions
is often greater than had been supposed
3. Plans drawn up in a prescriptive manner by
local people are more likely to work than
plans drawn up by outsiders
4. The participative nature of the process is a “
Development Benefit” in itself, in terms of
empowering people
5. Highly cost-effective
11. RECOMMENDED AND ACTUAL FEEDING PRACTICES
S.NO PRACTICE
LEVEL OF PRACTICE (%)
INDIA TAMIL NADU
1 Initiation of breastfeeding within 1 hour of birth 25 59
2 No pre-lacteal feeding 43 79
3 Exclusive breastfeeding (first 6 months) 46 34
4 No bottle feeding (12-23 months): 86 62
5 Timely complementary feeding (age 6-8 months) 53 81
6
Feed breast milk or milk products, and feed at least a minimum
number of times from at least a minimum number of food
groups (age 6-23 months)
21 29
7
Given vitamin A supplements in last 6 months (children age 12-
35 months)
25 45
8
Universal salt iodization: Percent of children age 6-59 months
living in households using adequately iodized salt:
48 39
Source: National Family Health Survey-3 (2005-06)
12. FACT SHEET ON MATERNAL & CHILD HEALTH
S.No Indicator India Tamil Nadu
1
Mothers who had at least 3 Antenatal visits
for last child birth
50.7% 96.5%
2
Mothers who consumed Iron and folic acid
tablet for 90 days or more when they were
pregnant with last child
22.3% 43.25
3
Births assisted by a Doctor/ Nurse/ LHV/
ANM/ other health personnel
48.3% 93.2%
4 Institutional births 40.7% 90.45%
5
Mothers who received Antenatal care from
a health personnel within 2 days of delivery
for their last birth
36.4% 89.6%
Source: National Family Health Survey-3 (2005-06)
13. STANDARD PRECAUTIONS
PRINCIPLE: Standard precautions
require that health care workers
assume that the blood and body
substances of all patients are
potential sources of infection,
regardless of the diagnosis or
presumed infectious status.
APPLICATION: Standard
precautions are used in the care of
all patients and apply to blood, all
body fluids, secretions and excretions
except sweat, regardless of whether
they contain visible blood.
Standard precautions include the
following-
1. Hand washing and antisepsis
2. Use of personal protective
equipment when handling blood,
body substances, excretions and
secretions
3. Appropriate handling of patient
equipment and soiled linen
4. Prevention of needle-stick / sharp
injuries
5. Management of health care waste
14. NATIONAL HEALTH PROGRAMMES
Maternal & Child Health
1. Reproductive & Child Health
Programme, Phase II (2004-2009)
2. National Rural Health Mission.
3. School health program.
Communicable Diseases
1. National AIDS Control Programme
Phase-III
2. Revised National Tuberculosis Control
Programme, 1993
3. National Vector Borne Diseases
Control Programme.
4. Yaws Eradication Programme, 1996
5. National Leprosy Eradication
Programme
6. Rabies Control Programme
Non Communicable Diseases
1. National Programme for Control of
Blindness, 1976
2. National Mental Health Programme, 1982
3. National Cancer Control Programme,
1975
4. National programme for prevention and
control of Diabetes, Cardiovascular
diseases and Stroke.
5. National Program for Prevention and
Control of Deafness.
6. National Oral Health Program.
7. National Programme for Control &
Treatment of Occupational Diseases,
1998
15. Nutritional Programmes
1. ICDS Scheme, 1975
2. Mid Day Meal Programme, 1962
3. Special Nutrition Programme, 1970-71
4. Balwadi Nutrition Programme, 1970
5. Applied Nutrition Programme, 1973
6. National Nutritional Anemia
Prophylaxis Programme, 1970
7. Programme for Prophylaxis Against
Blindness due to Vitamin –A
Deficiency, 1988-90
8. National Iodine Deficiency Disorders
Control Programme, 1962
Other Programmes
1.India Population Project
2.National Programme for
Rehabilitation of Persons with
Disabilities
3.National Emergency Preparedness
Plan: Disaster Management
4.Basic Minimum Service Programme
5.Poverty Alleviation Programme
6.National Water & Sanitation
Programme
7.National Programme of Improved
Chulha
8.Accelerated Urban Water Supply
Programme, 1993-94
NATIONAL HEALTH PROGRAMMES
16. HEALTH RELATED ACTS & LEGISLATIONS
Medical Education & Services
1. Indian Medical Council Act, 1956 &
Regulations, 2002
2. Indian Nursing Council Act, 1947
3. Indian Dentists Act, 1948
4. Indian Pharmacy Act, 1948
Disabled & Disadvantaged Groups
1. The Mental Health Act, 1987
2. The SCs & STs (Prevention of Atrocities)
Act 1989
Drug Addiction & Substance Abuse
1. The Cigarettes and other Tobacco
products Act 2003
2. The Narcotic Drugs & Psychotropic
Substances Act, 1985
3. The Drugs (Control) Act, 1948
Public Health Problems
1. Epidemic Disease Act, 1897
2. Bio medical waste (Management and
Handling) Rules, 1998
3. Food safety and standards Act 2003
4. The Registration of Births & Deaths Act
1969
5. Tamil Nadu Public Health Act,1939.
To Safeguard Children & Young
1. The Pre-Conception and Prenatal
diagnostic techniques act 1994
2. The Infant Milk Substitutes, Feeding
Bottles & Infant Foods Act, 1992
3. Juvenile Justice (Care and Protection of
children) Act, 2000
4. Child Labour ( Prohibition & Regulation)
Act, 1986
5. Child Marriage Restraint Act, 1929
17. Maternal Health
1. MTP Act, 1971
2. Maternity Benefit Act 1961
3. Dowry Prohibition Act 1961
4. Immoral Traffic (Prevention) Act 1956
5. Pre-Conception & Prenatal Diagnostic
Techniques (Prohibition of Sex Selection)
Act 1994
6. Protection of Women from Domestic
Violence Act 2005
Workers & Social Security
1. Minimum Wages Act 1948
2. Factories Act 1948
3. Mines Act 1952
4. ESI Act 1948 & Regulations 1950
5. Workmen’s Compensation Act 1923
Environmental Health Legislations
1. Environment (Protection) Act 1986
2. Biomedical Waste (Management &
Handling) Rules 1998
3. Municipal Solid Waste (Management &
Handling) Rules 2000
4. National Environment Tribunal Act 1995
5. Public Liability Insurance Act 1991
6. Air (Prevention & Control of Pollution) Act
7. Water (Prevention & Control of Pollution)
Act 1974
8. Atomic Energy Act 1962
9. Insecticides Act 1962; Insecticides Rules
1993
10.Motor Vehicles Act 1988
HEALTH RELATED ACTS & LEGISLATIONS
18. COMMON DISEASES/ CONDITIONS FOR SCREENING
Pregnancy
• Anaemia
• Hypertension, Toxemia
• Rh Status
• Syphilis ( VDRL)
• Diabetes
• Cardiovascular disease
• Neural Tube Defects
• Down’s Syndrome
• HIV
Elderly
• Nutritional Disorders
• Cancer
• Tuberculosis
• Chronic Bronchitis
• Glaucoma
• Cataract
Infancy
• Congenital Dislocation of Hip
• Spina Bifida
• Cerebral Palsy
• Hearing Defects
• Hypothyroidism
• Developmental screening Test
• Haemoglobinopathies
• Sickle cell Anemia
• Undescended testis
Middle Aged Men & Women
• Hypertension
• Cancer
• Diabetes Mellitus
• Serum Cholesterol
• Obesity
19. NATIONAL RURAL HEALTH MISSION
(2005-12)
VISION : To provide effective healthcare to rural population throughout the country with
special focus on 18 states, which have weak public health indicators and/or weak
infrastructure.
• A female Accredited Social Health
Activist (ASHA) - act as the interface
between the community and the
public health system.
• Strengthening sub-centre through an
untied fund
• Strengthening existing PHCs and CHCs,
• Health Plan for each village and district
• Integrating vertical Health and Family
Welfare programmes at National , State
, Block and District levels.
• Public-Private Partnership for public
health goals.
• A Task Group to examine new health
financing mechanisms
• Reorienting Health/Medical Education to
support rural health issues.
PLAN OF ACTION
Source: http://nrhm.nic.in
20. EFFECTS OF CLIMATE CHANGE ON HEALTH
Direct
Thermal Stress
Indirect
Ecologically mediated
Vector-borne diseases
Marine-borne diseases
Food productivity
Air pollution
Weather disaster
Sea-level rise
CLIMATE
CHANGE
OZONE
DEPLETION
Cardiovascular and
respiratory morbidity and
mortality
e.g. Malaria, dengue,
schistosomiasis
Toxic algae and cholera
Malnutrition
Asthma and cardio-respiratory
disorders
Deaths, injuries, damage to
health infrastructure,
increased risk of infectious
diseases, conflicts
Skin cancers, cataract,
immunosuppression
21. CLASSIFICATION OF PROTEIN ENERGY MALNUTRITION (PEM)
Based on weight for age
(% of expected):
Nutritiona
l status
Gomez
1956
IAP
1972
Normal >90 >80
I degree 75-90 71-80
II degree 60-75 61-70
III degree
<60, all cases
with edema
51-60
IV degree <50
Based on height for age
(% of expected):
Height for age
(% of expected)
Waterlow’s
Normal >95
I degree stunting 90-95
II degree stunting 85-90
III degree stunting <85
EARLY DETECTION OF PEM IN COMMUNITY
SHAKIR’S TAPE – to measure Mid Arm Circumference
between 1 to 5 years of age
>13.5 cm -- Green -- Normal
12.5-13.5 cm -- Yellow -- Moderate PEM
<12.5 cm -- Red -- Severe PEM
• Bangle test – inner diameter of 4 cm
• Nabarrow’s thinness chart – (Wt for HT)
• Growth card ( Age dependent)
22. NATIONAL AIDS CONTROL PROGRAMME PHASE – III
[2006-2011]
Goal
To halt and reverse the epidemic in
India over the next 5 years
Specific objective
To reduce new infection as estimated
in the first year of the programme by:
Sixty per cent (60%) in high
prevalence states so as to obtain the
reversal of the epidemic; and
Forty per cent (40%) in the vulnerable
states so as to stabilize the epidemic.
Strategies
1. Prevention of new infections in high risk
groups and general population through:
a. Saturation of coverage of high risk
groups with targeted interventions
b. Scaled up interventions in the
general population
2. Providing greater care, support and
treatment to larger number of PLHA.
3. Strengthening the infrastructure, systems
and human resources in prevention, care,
support and treatment programmes at the
district, state and national level.
4. Strengthening the nationwide Strategic
Information Management System.
Source: http://nrhm.nic.in
23. COMPUTER VISION SYNDROME
• Computer monitor emit no harmful
ionizing radiation (such as X-ray) or
non ionizing radiation (such as ultra
violet rays) under normal operating
conditions.
• Computer monitors can cause Dry
eyes, Eye strain, Eye irritation, Head
ache, Back ache etc,
• Changing the arrangement of the work
station or providing rest to the eyes in
between the work often relieve these
complaints.
Prevention
• Computer users should keep their
screen at a distance.
• Place the monitors slightly below eye
level.
• The reference material should be kept
close to the screen to minimize head
and eye movements and focusing
changes.
• Illumination should be proper to
minimize reflection and glare use.
• The monitor screen should be kept
clean.
• Frequent blinking will lubricate the eyes
and prevent them from drying out.
Source: http://nrhm.nic.in
24. • 80-90% of all eye injuries are
preventable. 45-45% of them occur in
and around the home.
• Eye injuries need urgent medical
attention. Self treatment should be
avoided.
Preventive measures during
festival
• Don’t give crackers to small children.
• Don’t stand too close to fireworks.
• Don’t ignite fireworks indoor.
• Adult supervision is essential.
• Place a bucket of water nearby to put
out fire.
• If chemicals falls in the eyes wash with
plenty of water.
PREVENT ‘EYE’ INJURIES
Preventive measures at home
• Sharp edged toys, knife, needle,
scissors etc,--Kept away from children.
• All spray nozzles are directed away
from when we press down on the
handle.
• Instructions read carefully before using
detergents, ammonia, or harsh
chemicals. Hands washed thoroughly
after use.
Preventive measures at play
• Avoid projectile toys such as pellet guns.
• Many toys with pointed or sharp ends
and games like boxing can prove
dangerous.
• Teach children the correct way to handle
potentially dangerous items such as
scissors, pencils, bows and arrows.
Source: http://nrhm.nic.in
25. NOTIFIABLE DISEASES AS PER SECTION 62 OF
TAMILNADU PUBLIC HEALTH ACT - 1939
NAME OF THE
DISEASE
GO
NO.
CEREBRO-SPINAL
FEVERS
As
Per
Section
62
of
TNPH
Act
-
1939
CHICKEN POX
DIPHTHERIA
LEPROSY
CHOLERA
MEASLES
PLAGUE
RABIES
SCARLET FEVER
SMALL POX
TYPHOID /
ENTERIC FEVER
NAME OF THE
DISEASE
G.O. NUMBER
TUBERCULOSIS G.O.Ms.No.211/Health/ Dated:18-1-1955
INFECTIOUS
HEPATITIS
G.O.Ms.No.1054/Health/ Dated:21-3-1956
EPIDEMIC INFLUENZA G.O.Ms.No.1497/Health/ Dated:15-5-1957
WHOOPING COUGH G.O.Ms.No.2355/Health/ Dated:30-7-1958
VIRAL ENCEPHALITIS G.O.Ms.No.2415/Health/ Dated:6-8-1958
HAEMORRHAGIC
FEVER
G.O.Ms.No.214/Health/ Dated:1-10-1964
MALARIA G.O.Ms.No.2797/Health/ Dated:1-12-1972
TETANUS
G.O.Ms.No.1404/Health/ Dated:30-8-1980
POLIO
AIDS G.O.Ms.No.1220/Health/ Dated:3-7-1990
26. TOBACCO CONTROL ACT 2003
Cigarettes and Other tobacco products
(Prohibition of Advertisement and
Regulation of Trade and Commerce,
Production, Supply, and Distribution) Act,
2003
FOUR KEY COMPONENTS
• Prohibition of smoking in a public place –
S.4
• Prohibition of advertisement of cigarettes
and other tobacco products – S.5
• Prohibition on sale of cigarettes or other
tobacco products to and by minors and in
a particular area – S.6
• Specified health warning labels on all
tobacco products including pictorial
warnings – S.7,8,9,10
Amendment rules notified in 2005
• Sale through vending machines
banned
• Ban on display of tobacco products or
their use in movies or television
• Health warning to be placed as a
prominent bottom scroll in cinema and
television programmes, which have
been produced prior to this notification
• Ban on display of names / logos of
tobacco brands in any manner during
media coverage of international events
sponsored by tobacco manufacturers.
27. SOCIO ECONOMIC CLASSIFICATION
• Prasad classification
• Standard of living index – Rural
areas
• Kuppuswamy’s scale – Urban
areas
• Pareek classification – Rural areas
PRASAD CLASSIFICATION
Social
class
Per capita income
of the family
I >2200
II 1100 – 2199
III 660-1099
IV 330-659
V <330
28. GOALS TO BE ACHIEVED BY 2005-2015
( NATIONAL HEALTH POLICY 2002)
Goal
Target
year
Eradicate Polio and Yaws 2005
Eliminate Leprosy 2005
Eliminate Kala Azar 2010
Eliminate Lymphatic Filariasis 2015
Achieve Zero level growth of HIV/AIDS 2007
Reduce Mortality by 50% on account
of TB, Malaria and Other Vector and
Water Borne diseases
2010
Reduce Prevalence of Blindness to
0.5%
2010
Reduce IMR to 30/1000 And MMR to
100/Lakh
2010
Increase utilization of public health
facilities from current Level of <20 to
>75%
2010
Goal
Target
year
Establish an integrated system of
surveillance, National Health Accounts
and Health Statistics.
2005
Increase health expenditure by
Government as a % of GDP from the
existing 0.9 % to 2.0%
2010
Increase share of Central grants to
Constitute at least 25% of total health
spending
2010
Increase State Sector Health spending
from 5.5% to 7% of the budget
Further increase to 8%
2005
2010
29. DEMOGRAPHIC CYCLE & TRANSITION
Over decades, the change in the population size shows a step by step pattern. These
pattern of variation is called as ‘Demographic Cycle’.
India is in the middle of Demographic transition (Late Expanding stage).
Both fertility and mortality are declining. Births exceed Deaths –Population continues
to grow.
1. High
Stationary
2. Early
Expanding
3. Late
Expanding
4. Low
Stationary
5. Declining
Demographic
Cycle
30. HOSPITAL WASTE DISPOSAL: COLOUR CODING
Colour coding Type of Container Waste Category Treatment options
Yellow Plastic Bags
Human and animal wastes, Microbial
and Biological wastes and soiled
wastes
Incineration/ Deep Burial
Red
Disinfected container/
Plastic bags
Microbiological and Biological wastes,
Soiled wastes, Solid wastes
Autoclave/ Microwave/
Chemical Treatment)
Blue/ White/
Transparent
Plastic bag, Puncture
proof container
Waste sharps and solid waste
Autoclave/ Microwave/
Chemical Treatment
Destruction and Shredding
Black Plastic bag
Discarded medicines, Cytotoxic drugs,
Incineration ash and chemical waste
Disposal in secured land
fills
Green Plastic Container
General waste such as office waste,
food waste & garden waste
Disposed in secured
landfills
31. India & Major States
IMR
(2005)
India 58
Assam 68
Bihar 61
Madhya Pradesh 76
Orissa 75
Rajasthan 68
Uttar Pradesh 73
Andhra Pradesh 57
Karnataka 50
Kerala 14
Tamil Nadu 37
Gujarat 54
Haryana 60
Maharashtra 36
Source: Current level—SRS Bulletin,
Vol. 41, No. 1, October 2006
Trend of Infant Mortality Rate in India Infant Mortality Rate in
Major States of India
Source: National Family Health Survey (2005-06)
INFANT MORTALITY RATE IN INDIA
Infant mortality rates by demographic characteristics
Mother's age at birth Birth order Previous birth interval
32. SANITATION BARRIER
Disease cycle may be broken at various
levels
1. Segregation of faeces
2. Protection of foods
3. Personal hygiene
4. Control of flies
Most effective step is segregation of
faeces and proper disposal.
• Segregation of excreta can be done by imposing barrier called sanitation barrier.
• This Barrier can be provided by sanitary latrine and disposal pit.
• More elaborate system includes installation of sewerage system and treatment plants.
• Thereby the disease agent cannot reach the new host, Directly or Indirectly.
33. • The greenhouse effect is a natural
warming process. Carbon dioxide (Co2)
and certain other gases are always
present in the atmosphere. These
gases create a warming effect that has
some similarity to the warming inside a
green house, hence the name ‘green
house effect’.
• The greenhouse effect is important.
Without the greenhouse effect, the
Earth would not be warm enough for
humans to live. But if the greenhouse
effect becomes stronger, it could make
the Earth warmer than usual.
• Human actions, particularly the burning
of fossil fuels, are increasing the
concentration of green house gases.
This is believed to be raising the Earth's
temperature, creating the prospect of
global climate change. This is the
Enhanced Greenhouse Effect.
34. CURRENT CONTRACEPTIVE USE BY METHOD
Source: NFHS-3, India, 2005-06
Percent of currently married women age 15-49
35. HOUSEHOLD ENVIRONMENT : NFHS-3 DATA
• 68% of households
have electricity, up from
60% in NFHS-2
• 88% of households use
an improved source of
drinking water
• Only 29% of households
have improved toilet
facilities
Source: NFHS-3, India, 2005-06
36. HIV ESTIMATES IN INDIA
Source: National Family Health Survey-3 (2005-06)
Sex
Women
(%)
Men (
%)
Total
(%)
Urban 0.29 0.41 0.35
Rural 0.18 0.32 0.25
Total 0.22 0.36 0.28
HIV Prevalence by place of residence
State
Women
(%)
Men
( %)
Total
(%)
Manipur 0.76 1.59 1.13
Andhra Pradesh 0.76 1.22 0.97
Karnataka 0.54 0.86 0.69
Maharashtra 0.48 0.78 0.62
Tamil Nadu 0.40 0.27 0.34
Uttar Pradesh 0.05 0.10 0.07
Non-high
prevalence states
0.08 0.16 0.12
Total 0.22 0.36 0.28
HIV Prevalence by State
HIV/ AIDS awareness indicators
37. PREVALENCE OF ANEMIA AMONG WOMEN IN INDIA
Category Hb (gm/dl)
Normal > 11
Mild 10 - 10.9
Moderate 7.0 - 9.9
Severe < 7.0
Classification of Anemia in Pregnant and
non-pregnant women
26
31
2
59
39
16
2
56
0
10
20
30
40
50
60
70
Mild Moderate Severe Any anaemia
Pregnant women Non-pregnant women
Prevalence of Anemia in Pregnant and
non-pregnant women of India
Source: National Family Health Survey-3 (2005-06)
38. TOTAL FERTILITY RATE (TFR)
• TFR represents the average number of
children a women would have if she were to
pass through her reproductive years bearing
children at the same rates as the women now
in each age group.
• This measure gives the approximate
magnitude of “completed family size”
• In simple terms TFR denotes –average
number of children borne per women.
• Current TFR- 2.7
• Goal- To achieve TFR 2.1 by 2010 as
per National Population Policy
• All India TFR is expected to reach
replacement level by 2021(GOI)
Source: National Family Health Survey-3 (2005-06)
41. LITERACY
A Person is deemed as ‘Literate’ if
she / he can read and write with
understanding in any one of the
Languages
A Person who can merely read but
can not write is not considered
‘Literate’
Expressed as Percentage (%)
As per Census 2001 the Literacy
Rates for Males, Females & Total
were 75.85%, 54.16%, & 64.38%
respectively
States with < 56 % Literacy Rate:
Bihar, J&K and Arunachal Pradesh
Source: Census 2001. Government of India
42. OZONE DEPLETION
o The ozone layer is a thin layer of ozone in
the atmosphere, 10 - 50 kilometres above
the earth.
o The ozone layer absorbs most of the
harmful ultraviolet-B radiation from the
sun.
o The production and emission of
chlorofluorocarbons, is by far the leading
cause of ozone depletion.
o If the ozone layer depletes, more harmful
UV-B radiation will reach the earth through
the damaged ozone layer.”
o More UV-B radiation means more skin
cancers, more diseases and eye cataracts,
less yield from plants, less productivity
from oceans, damage to plastics
Ozone absorbs
99% of the
harmful ultra
violet (UV)
radiation.
What does ozone layer do?
Most of the
harmful UV
radiation will
penetrate the
atmosphere
Without the ozone layer
43. MATERNAL CARE - INDIA
Antenatal care (for most recent birth
in the last 5 years)
(Percentage)
Source: National Family Health Survey-3 (2005-06)
44. NUTRITIONAL STATUS OF CHILDREN
Indicators
Height-for-age (stunting)
Indicator of chronic under-nutrition
Weight-for-height (wasting)
Indicator of acute under-nutrition
Weight-for-age (underweight)
Composite measure of chronic and acute
malnutrition
Under-nutrition in Children under Age 5
INDIA and Tamil Nadu
Source: National Family Health Survey-3 (2005-06)
45. PREVENTION OF PARENT TO CHILD TRANSMISSION (PPTCT)-HIV
The Four-Pronged Approach to PPTCT
1. Primary prevention of HIV infection
(Abstinence, Faithful to one HIV-uninfected
partner, Condoms)
2. Prevention of unintended pregnancies in HIV-
infected women (Safe, consistent, effective
contraception)
3. Prevention of HIV transmission from HIV-
infected women to their infants (ARV
prophylaxis, Safer delivery practices, Safer
infant feeding practices )
4. Provision of treatment, care and support of
HIV-infected women, their infants and their
families (Prevention and treatment of
opportunistic infections, ARV treatment,
Palliative and non-HIV care, Nutritional
support)
46. NATIONAL CLASSIFICATION OF OCCUPATIONS- 2004
1. Legislators, senior officials and managers
2. Professionals
3. Technicians and associate professionals
4. Clerks
5. Service workers and shop & market sales workers
6. Skilled agricultural and fishery workers
7. Craft and related trades workers
8. Plant and machine operators and assemblers
9. Elementary occupations
10. Workers not classified by occupations
Source: http://dget.nic.in
47. NEW INTERVENTIONS IN FAMILY PLANNING
(GOI)
• Addressing the unmet need in contraception through
a. Assured delivery of family planning services.
b. Developing skilled manpower for the same.
• Increasing male participation through intensive promotion of no
scalpel vasectomy.
• Promotion of IUDs as a short and long term spacing method.
• Promotion of Emergency contraceptive pills.
• Ensuring Quality care in Family Planning services.
• Promoting public private partnerships.
• Revised compensation scheme.
• Family planning insurance scheme.
• Increasing basket of services.
• Promoting contraceptives through increased advocacy
Source: http://mohfw.nic.in