
Recommended
More Related Content
Similar to JOINING FORCESJOINING FORCESJOINING FORCESJOINING FORCESJOININ.docx
Similar to JOINING FORCESJOINING FORCESJOINING FORCESJOINING FORCESJOININ.docx (20)
More from christiandean12115
More from christiandean12115 (20)
Recently uploaded
Recently uploaded (20)
JOINING FORCESJOINING FORCESJOINING FORCESJOINING FORCESJOININ.docx
- 1. JOINING FORCESJOINING FORCESJOINING FORCESJOINING FORCESJOINING FORCES A Crosswalk of the Human Services Value Curve with Organizational Culture and Climate By Anthony Hemmelgarn and Phil Basso JOINING FORCESJOINING FORCESJOINING FORCESJOINING FORCESJOINING FORCESJOINING FORCESJOINING FORCESJOINING FORCESJOINING FORCESJOINING FORCESJOINING FORCES Policy & Practice June 201624 A s we evolve in our working partnership with APHSA’s Organizational Effectiveness team and the University of Tennessee’s Center for Behavioral Health Research (CBHR), formerly the Children’s Mental Health Services Research Center, we have discovered great synergy in our respective efforts for supporting agency performance. These include APHSA’s efforts to help agencies progress through stages of the Health and Human Services Value Curve, and CBHR’s efforts to help
- 2. agencies improve by addressing their organizations’ cultures and climates. The Value Curve is a lens—a way of looking at what we do from the point of view of our consumers—and its four levels represent ways of engaging consumers and their communities that result in greater impact as orga- nizations move up the Value Curve. At the first level, called the regula- tive level, the key word is “integrity.” Consumers receive a product or service that is timely, accurate, cost effective, and easy to understand. Next, at the collaborative level, the key word is “service.” Consumers have an easier time of it when they “walk through a single door” and have access to a more complete array of products and services because programs, and even jurisdictions, are collaborating to make it happen for them. At the integrative level, the key term is “root causes.” Products and services are designed using consumers’ input so that we address their true needs and even begin to reach “upstream” to address causal problems rather than “treating the symptoms.” At the gen- erative level, the key term is “bigger than the family.” Root- cause analysis is done at a “population-wide level,” resulting in prevention strategies and other forms of support broader than
- 3. those an individual or family would receive directly.1 Organizational culture and climate is another potent lens that human service organizations can use to look at their performance and improve their outcomes. APHSA’s partners at CBHR have been building that case for more than 20 years, demonstrating the substantial impact of organizational culture and climate on the effective- ness of human services.2 Their work demonstrates that: (1) human service agencies vary widely in their organi- zational culture and climate profiles, (2) agencies with positive profiles have substantially better outcomes, and (3) agencies can improve their turnover, EBP/EBT implementation, client, and other outcomes through strategies that improve their cultures and climates. The CBHR uses its Organizational Social Context Measure (OSC-M) to profile agencies across dimensions of culture and climate that have been shown to be important to the suc- cessful functioning of human service organizations. Taken together, these dimensions encapsulate key aspects of an agency’s “personality” and offer insights that can be used to improve performance metrics. As an example of the synergy
- 4. between our two models, the following crosswalk describes proficiency, one of the dimensions of culture, in the context of the Value Curve. In profi- cient cultures, staff shares expectations that it will be responsive to the unique needs of its clients and have up-to- date knowledge and practice skills.3 Broadly, we expect proficiency levels to rise as organizations advance to higher levels on the Value Curve. The Regulative Level and Proficiency The regulative level for organiza- tions is about building a stable and reliable infrastructure, and while the value proposition is foundational and compliance oriented, much of the cultural focus is internal. This includes laying out standards and pro- cesses for how the organization will operate, creating greater certainty, and establishing a framework to achieve efficiency. These are essential organi- zational capabilities; without them, there is chaos and failure. Unfortunately, organizations at this level can easily elevate order and “covering the bases” to be ends rather than means. When this happens, pro- ficiency drops dramatically. Phil Basso encounters this often in his fieldwork,
- 5. and coined the term “bad regulative” for this approach (see his article in April’s Policy and Practice, “Travels with the Value Curve”). A number of years ago Anthony Hemmelgarn helped conduct 25 focus groups from one end of a state to the other. More than 200 child welfare managers participated. The goal of each session was to answer a single question: “What needs to be measured to determine staff success?” The answers, over and over, were about process: how many clients were contacted, how many seen, paper- work completed on time. In and of themselves, there is nothing wrong with such responses. But not a single manager suggested anything related to clients getting better, and a laser focus on this is essential for high proficiency. This child welfare system was paying little attention to addressing its clients’ needs. Proficiency, we can safely assume, was extremely low. Human service systems often rely on standardized case management practices, such as requirements to visit families so many times per week, in a sincere effort to improve quality of care. But such tactics run counter to proficiency. “One size fits all” policies are, in fact, unresponsive to clients’ unique needs. Case managers’ time
- 6. and other valuable resources are rou- tinely wasted. Morale suffers. June 2016 Policy & Practice 25 It must also be noted that many of the regulatory requirements that agencies confront are externally applied and beyond the control of agency leaders and staff . They must meet funder requirements. They must trying new approaches, and effi cacy in helping clients builds; attention to eff ectiveness for clients increases along with profi ciency. Front-line staff must also be able to work closely together within its own teams, and the teams must have the skills and tools neces- sary to eff ectively interact and problem solve with other programs and depart- ments, and with external organizations and stakeholders. Such work increases the probability that programs and organizations will reach out and work with others in the community. As with individuals, a sense of effi cacy increases confi dence and openness to relating to others. Eff ective teams with a clear sense of purpose, organizational support, and a sense of their competence to improve their clients’ well-being provide plat-
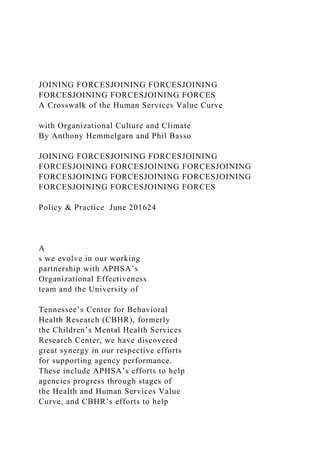
- 7. forms for broadening the network of relationships required to reach higher levels of the Value Curve. However, collaboration has its own traps. Similar to the regulative level, an overemphasis on process can undo profi ciency. For example, spending considerable time and eff ort negoti- ating collaborations across programs Ef� ciency in Achieving Outcomes Effectiveness in Achieving Outcomes Regulative Business Model: The focus is on serving constituents who are eligible for particular services while complying with categorical policy and program regulations. Collaborative Business Model: The focus is on supporting constituents in receiving all services for which they’re eligible by working across agency and programmatic borders. Integrative Business Model: The focus is on addressing the root causes of client needs and problems by coordinating and integrating services at an optimum level. Generative Business Model: The focus is on generating healthy communities by co-creating solutions for multi-dimensional
- 8. family and socioeconomic challenges and opportunities. Generative Business Model Integrative Business Model Ou tco me Fr on tie rs Collaborative Business Model Regulative Business Model © The Human Services Value Curve by Antonio M. Oftelie & Leadership for a Networked World is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. Based on a work at lnwprogram.org/hsvc. Permissions beyond the scope of this license may be available at lnwprogram.org.
- 9. The Human Services Value Curve comply with legal mandates. While uniformly well intended, such external pressures often result in barriers to increasing profi ciency. This is particu- larly true when compliance is enforced negatively or in a punitive fashion. The Collaborative Level and Profi ciency At this level, organizations are concerned with connecting across programs and agencies to improve effi ciency and eff ectiveness. More pro- fi cient organizations are likely to work toward meaningful client outcomes that cut across internal silos. They are more likely to involve teams and personnel at all levels in improvement- driven activities such as Continuous Quality Improvement. There is more emphasis on the effi cacy of front-line staff as well as support for the front- line staff to learn from their errors, mistakes, and problems. At the most important end of human service organizations—the front line—staff must feel safe and confi - dent in its ability to achieve outcomes centered on client well-being. As skills develop internally, safety increases for Policy & Practice June 201626
- 10. Phil Basso is the deputy director of the American Public Human Services Association. Anthony Hemmelgarn is an industrial and organizational psychologist, is a research scientist at the University of Tennessee’s Center for Behavioral Health Research. http://lnwprogram.org/hsvc http://lnwprogram.org/ and organizations can consume resources better directed toward clients. Collaboration can also become its own end rather than a means, leading to excessive focus on collabo- ration-driven sharing (e.g., paperwork) and miss the boat on solving real barriers to client care. An additional concern is that the research on collaboration as a way to improve client outcomes is mixed. Moreover, collaboration can be seen by communities as a panacea to address a
- 11. lack of resources. Basically, let’s have this poor program work with that poor program, and we won’t need to increase funding for this service. This happens frequently in communities, and is a harmful side of collaboration. In Basso’s fieldwork he has, at times, discovered that agency leaders view themselves as operating at the Integrative level, but then cannot demonstrate related methods for family-centered engagement, compre- hensive risk assessment, root-cause analysis tools and metrics, or related caseworker skill-building, suggesting the move to a collaborative mode was targeted to streamlining business processes only. Proficiency through the Value Curve’s Collaborative stage still requires sufficient resources to get the desired value and set the stage for further progress. The Integrative Level and Proficiency The distinguishing characteristic of this level is pulling clients into the problem-solving process. In organiza- tions that achieve this level, proficiency is likely to be high. Integrating clients into the process means letting go of power and transferring it to the clients. Teams and programs with the confi- dence, skill, and support necessary to
- 12. do this will have high proficiency levels. The integrative level also requires rethinking casework practice and the use of technology and data. The his- torical failure rate for such endeavors in child welfare is alarmingly high. Why? Because these types of changes are almost always applied from the top down, assuming that it will be benefi- cial for front-line case managers and their clients. Little thought is given to the perceived impact on the front line. The OSC Measure and ARC (avail- ability, responsiveness, and continuity) change strategy are built on the socio- technical model of change. This model argues that technological change is as much a social process as a technological one. In sum, inattention to social issues and concerns (organizational culture and climate) dooms technological change. This is a primary cause of the numerous technological failures in child welfare. Organizations at the integra- tive level will necessarily have positive cultures and climates, including profi- ciency. This foundation is essential for organizations to address the sweeping challenges required to achieve this level. APHSA’s Organizational Effectiveness (OE) practice model and toolkit focuses on guiding a process whereby the organization’s own staff
- 13. generates solutions by first defining a desired state, assessing current strengths and gaps, determining the root causes for gaps, and then setting in motion solutions that are well-sup- ported in implementation and ongoing monitoring, forming a learning cycle. This approach—similar to an integra- tive casework approach—is designed to build proficiency while establishing a sound structure and process for improvement and goal attainment. The Generative Level and Proficiency This level moves to a broad, commu- nity-based conceptualization of service delivery and addressing risk factors at a population level, through co-creating new capacity in the community as a whole, and through joint advocacy efforts that affect general beliefs and norms that may enable or impede progress. To achieve this Value Curve stage, multiple organizations will need to come together. They will have to share a great deal. They will have to trust each other. They will have to share a common vision. Funders, particularly federal and state governments, will have to re-con- ceptualize what they want to fund. Frankly, it is hard to envision this in most communities. At the same time,
- 14. when it comes to the culture of commu- nity leaders, partners, and consumers of health and human services, this stage is most appealing as the desired state of things. Head issues off at the pass by working on them upstream. Pay me now instead of paying me later. Build a com- munity that evens the playing field for people and helps them reach their full potential. It is fair to say that high pro- ficiency will be a prerequisite across all participating organizations to reach the generative level. And, both the expecta- tion of proficiency and proficiency itself will be prerequisite for funders and other stakeholders. What is certain in human services is that the problems being addressed are numerous, highly complex, and difficult to solve. This article demonstrates that our respective models add value to the other, and we believe this can benefit the organizations we work with. From our perspective, combining these two lenses leads to a better focus and clearer solutions than either lens alone. Reference Notes 1. See the Human Services Value Curve at http://aphsa.org /content/dam/ aphsa/Toolkit/Human%20Services%20 Value%20Curve%209-5-14.pdf 2. Glisson, C., Hemmelgarn, A., Green, P.,
- 15. & Williams, N. (2013). “Randomized Trial of the Availability, Responsiveness and Continuity (ARC) Organizational Intervention for Improving Youth Outcomes in Community Mental Health Programs.” Journal of the American Academy of Child and Adolescent Psychiatry, 52(5), 493–500. 3. Williams, N. J., & Glisson, C. (2013). “Reducing turnover is not enough: The need for proficient organizational cultures to support positive youth outcomes in child welfare.” Children and Youth Services Review, 35:11, 1871–1877. It is fair to say that high proficiency will be a prerequisite across all participating organizations to reach the generative level. And, both the expectation of proficiency and proficiency itself will be prerequisite for funders and other stakeholders. June 2016 Policy & Practice 27 http://aphsa.org/content/dam/
- 16. Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. ESTABLISHING VALUES-BASED LEADERSHIP AND VALUE SYSTEMS IN HEALTHCARE ORGANIZATIONS DAVID R. GRABER ANNE OSBORNE KILPATRICK Medical University of South Carolina ABSTRACT The importance of values in organizations is often discussed in management literature. Possessing strong or inspiring values is increasingly considered to be a key quality of successful leaders. Another common theme is that organizational values contribute to the culture and ultimate success of organizations. These conceptions or expectations are clearly applicable to healthcare organizations in the United States. However, healthcare organizations have unique structures and are subject to societal expectations that must be accommodated within an organizational values system. This article describes theoretical literature on organizational values. Cultural and religious influences on Americans and how
- 17. they may influence expectations from healthcare providers are discussed. Organizational cultures and the training and socialization of the numerous professional groups in healthcare also add to the considerable heterogeneity of value systems within healthcare organizations. These contribute to another challenge confronting healthcare managers - competing or conflicting values within a unit or the entire organization. Organizations often fail to reward members who uphold or enact the organization’s values, which can lead to lack of motivation and commitment to the organization. Four key elements of values- based leadership are presented for healthcare managers who seek to develop as values-based leaders. 1) Recognize your personal and professional values, 2) Determine what you expect from the larger organization and what you can implement within your sphere of influence, 3) Understand and incorporate the values of internal stakeholders, and 4) Commit to values-based leadership. 180 JHHSA FALL 2008 In recent years, leadership writers and theorists have increasingly described values as a key component of effective leadership and as an essential trait for leaders to possess. A common theme is that leaders should possess a
- 18. strong foundation of personal values, principles, or ethics. Another recurring thought is that the values of the leader should reflect the organization’s values, which are transmitted to or at least accepted by the organization’s members. What is a value? It is defined in Webster’s Dictionary as “something (as a principle or quality) intrinsically valuable or desirable” (Merriam-Webster Online Dictionary, 2005). Rokeach offered a frequently cited definition of a human value as being an "enduring belief that a specific mode of conduct or end-state of existence is personally or socially preferable to an opposite or converse mode of conduct or end-state of existence" (Rokeach, 1973, p.5). Rokeach argued that one’s major values combine to form a value system, which is "an enduring organization of beliefs concerning preferable modes of conduct or end-states of existence along a continuum of importance" (1973, p.5). Thus, an individual will possess a plethora of values and these values will be given varying importance, albeit not necessarily consciously. Healthcare organizations often list principles in their mission statements that are courses of action or behavior, such as “Our hospital is committed to serving our patients and their family members by providing the highest level of patient care quality.” The underlying value for this principle might simply be “quality care.” The American public has deep-rooted values about the provision of healthcare. These values, which include compassion and service to others, may be at odds with healthcare organizations that have an organizational culture and organizational priorities that are largely independent of
- 19. JHHSA FALL 2008 181 these values. For a healthcare organization to fit into the community and achieve some degree of community goodwill, the organization should reflect and embody some measure of the community’s values. A few exemplary organizations may even be recognized for their professed and enacted values. Values are therefore conceived by the authors as critical contributors to the image and the success of an organization and its leaders. This article reviews recent literature on values and principles as key characteristics of effective leadership. Literature addressing the importance of values within the healthcare field and for healthcare managers is also described. The article discusses challenges facing healthcare managers who have strong personal values and wish to adhere to these values as much as possible. In conclusion, suggestions are given regarding how personal values systems may be successfully integrated into healthcare management. American Values and Healthcare The heritage and history of the United States and western culture is inextricably intertwined with American values as they relate to the provision of health care. Americans have always valued selfless service and compassionate health care. The majority of Americans raised in the Christian tradition were exposed from an early age to such stories as those of Christ healing lepers, the crippled, and the blind man, and the story of the Good
- 20. Samaritan. Throughout history many individuals who served the sick and dying have been highly respected and widely recognized. In the twentieth century, the work of Albert Schweitzer and Mother Theresa’s Sisters of Charity received world-wide acclaim. The early American traditions of hospitals with religious affiliations and almshouses founded by benevolent societies or religious groups also may have contributed to values held by many 182 JHHSA FALL 2008 Americans that there should be access to care for all, and the provision of healthcare should be something greater than a purely financial or economic enterprise. On the other hand, Americans tend to value individualism higher than people in virtually all other countries, and tend to rate a collectivist or community identification lower than people in many other countries (Hofstede, 1980). Individualistic values could be supportive of a healthcare system that does not serve everyone in the community, but serves those people who work hard, are successful, and are deemed to be deserving. Professional Values Little has been written the relation of one’s personal values to professional values, and the other levels of values (e.g., religious values, national values). For example, an individual will complete basic schooling, with an established value system: one that is based in his or her family, religious, cultural, and national background. After this, professional socialization often takes place. Professional socialization has been considered as potentially homogenizing value differences (among members of the same profession) and reducing individual
- 21. differences on at least some values (Hofstede, 1980). Using a values scale, undergraduate management students were noted to score higher on authority, advancement, economic, and risk values and lower on an altruism value, than undergraduate nursing students (Thorpe & Loo, 2003). This study suggests that values are related to choice of educational programs and to career choices. What is less known is the extent to which these values change during the course of education and professional socialization. One study, using the Balanced Emotional Empathy Scale, revealed a statistically significant decline in empathy among male medical students from the third to the fourth year of school (Newton JHHSA FALL 2008 183 et al., 2000). Another study used the Jefferson Scale of Physician Empathy, and noted a statistically significant decline in empathy from the first year of medical school to the third year among 125 medical students (Hojat et al., 2004). For those who expect some degree of empathic concern from their personal physician, these findings are troubling. If these findings can be generalized, they suggest that many medical students may enter medical school with compassionate and humanistic values, but these values are eradicated or suppressed during the course of education As the above-described study of Thorpe and Loo (2003) suggests, there appear to be differences in the value systems of individuals entering different disciplines: nurses are likely to value caring and compassion than management students, who may be more interested in authority and
- 22. advancement. However, the medical school education studies cited above provide evidence that individual value systems, whatever they may be at the inception of professional education, are influenced and modified in the course of professional education. Although values are normally considered to be “enduring beliefs”, the apparent malleability of the empathy value in the course of medical education begs the question, “To what extent are values truly enduring?” Are individual value systems modified during the course of professional education, or are professional values created, which do not supplant, but coexist, perhaps at times uncomfortably, with one’s underlying value system? Such questions have been largely unexplored in research studies. Values in Organizations The most comprehensive review of leadership literature in the early to mid-twentieth century may well have been that of Ralph Stogdill, who examined 287 studies conducted from 1904 through 1970 (Bass, 1981). 184 JHHSA FALL 2008 He noted hundreds of leadership traits that had been described in these studies - adherence to values or principles was not identified as one of the top ten traits. Stogdill’s work provides some evidence that a focus on values (and associated qualities such as integrity or character) was not, at least during most of the 20th century, considered among the most critical traits of leadership. In the latter part of the 20th century, a discussion of values in management became more common. Selznick (1957) wrote that organizations become mature and
- 23. “institutionalized” only when leaders infuse them with values. A new way of perceiving and evaluating experience is transmitted to employees, and the organization acquires a unique identity and competence. For Selznick, institutional change occurs in organizations through processes that are developed and implemented by organizational leaders, such as the transmission of values. James Burns articulated the widely-known paradigm of transformational leadership in the 1970s. The interrelation of employee and managers values is a key facet of transformational leadership. Burns stated, “The essence of leadership in any polity is the recognition of real need, the uncovering and exploiting of contradictions among values and between values and practice, the realigning of values…The leader’s fundamental act is to induce people to be aware or conscious of what they feel -- to feel their true needs so strongly, to define their values so meaningfully, that they can be moved to purposeful action” (Burns, 1978, p. 43). For Burns, leadership clearly involves influencing and clarifying human values and aligning them with the needs of the organization. In more recent years, management theorists have, to varying degrees, acknowledged values, and related factors, such as ethics and principles, as key ingredients in a successful leadership formula. The most widely-read of these theorists, Stephen Covey, in Principle-Centered JHHSA FALL 2008 185 Leadership, asserted that our values should be aligned with
- 24. certain correct principles, which show us the way to effective leadership. Covey also states that involving employees in developing a shared vision and principles for an organization will help unite people in the organization (Covey, 1991, p.185). In recent years, there has been a shift away from the concept of the leader as the primary or sole creator of an organization’s values, and as stated by Covey, a strong emphasis by many writers on organizations developing shared principles, values, and missions using a participative process. Other writers appear to differ from Covey and do not appear to consider values to be subjective, but consider values to be objective and fundamental. For example, Lebow and Simon (1997) list eight basic people values for organizations: truth, trust, mentoring, openness, giving credit, honesty, and caring. In contrast to Covey’s emphasis on principles, many organizational writers in recent years consider a focus on values to be the critical challenge facing organizational leaders. Blanchard and O’Connor (1997) consider solid and enduring shared values to be the foundation of a successful organization, and one that also leads to profitability. They stress involving all stakeholders in the process of formulating and institutionalizing the company’s values. Conger (1998) also describes shared values as critical, especially when seeking major change or making an appeal to members of the organization. Badaracco (1998) argued that values come to the forefront in challenging or difficult situations that confront organizations, which he termed defining moments. Then a true leader will reflect on one or more of the following questions, “Who am I?” “Who are we?” “Who is the company?” This process of self-enquiry enables the leader
- 25. to deeply discern his or her true values and live up to them. 186 JHHSA FALL 2008 Thus, challenges and crises are in a sense necessary to not only test, but to evoke, the leader’s values. The writers described above represent only a few of the numerous proponents of what is often termed, “values- based leadership”. However, in healthcare organizations values-based leadership is not always easily implemented, due to their unique cultures, and their structural and operational characteristics. Challenges to Implementing Shared Value Systems in Healthcare Organizations The literature on values in management and in healthcare organizations stresses the importance of identifying values and adhering to values. Circumstances and organizational structures that can ameliorate or even negate a values-based approach to management are rarely discussed. Healthcare is a unique field and particularly in large healthcare organizations, implementing value systems is almost always much more difficult than professing them. Diverse values among organizational groups. One of the main challenges to management-based values in hospitals is that managers have limited authority over professional, licensed personnel. This is particularly salient in regard to physicians with whom management has
- 26. traditionally shared authority. Since physicians are often not employees of a hospital (or of many other healthcare organizations), management’s capacity to influence physicians is limited. Alexander and Morlock (1994) describe some of the key cultural differences between physicians and healthcare executives on several key dimensions. They state that the executive’s focus is (or should be) on positioning the organization for the future, so their time frame of action is middle to long term. Physicians have a more short term time frame, arising from the necessity of meeting the JHHSA FALL 2008 187 immediate needs of patients. Executives are described as viewing resources as limited and being highly aware of the need to allocate scarce resources effectively. Conversely, physicians are said to consider resources as critical for serving their own patients and maximizing the quality of care. Executives consider service to patients within the organization and also providing services and programs to the greater community as being highly important. Physicians’ patient focus is considered to be much narrower – on their individual patients. Clearly, physicians and executives have different world views and professional identities, and their professional identities are based in different professional values. To minimize problems and conflicts it would seem essential for management to extensively elicit physician input in formulating and implementing organizational values systems. In doing this, both groups should learn to
- 27. understand what is important and worthwhile in each other’s value systems. Although physicians are undoubtedly key actors in healthcare organizations, they are not the only element in the considerable heterogeneity of these organizations. For example, as mentioned previously, nurses may possess stronger values of altruism and compassion than healthcare administrators (Thorpe and Loo, 2003). Healthcare organizations often have high proportions of members of specific racial or ethnic groups who may be dissimilar to management on some important values. Due to this heterogeneity, which is very common in many regions of the country, the formulation of organizational values should involve a multitude of internal groups and stakeholders. In such ethnically diverse situations, organizational members should try to identify overarching values. Smolicz (1985, p.11) notes that this process should allow ethnic groups to retain certain core values relating to their traditions, language, and religions, and also contribute to a dynamic 188 JHHSA FALL 2008 equilibrium, “between the overarching and shared values…and the ethnic or core values.” Similar to finding overarching values, is obtaining normative consensus, that is, consensus or agreement on the important norms for an organization. A norm is “a principle of right action… serving to guide, control, or regulate proper and acceptable behavior” (Merriam- Webster Online Dictionary, 2005). Values are considered internal and do not necessarily imply actions; however, norms do involve actions and behavior. Nevertheless,
- 28. norms are grounded in personal values. Organizations may wish to first establish overarching values, and then use this as a foundation for identifying the key norms in different department or units, using a participative approach to reach a normative consensus. Competing, conflicting, and shifting values There are not only diverse and sometimes competing values across professional groups, but values may clash within any group in the organization. Worthley (1999) describes common clashes in organizations between serving the individual or the community; achieving quality versus reducing costs; upholding patient rights or organizational control; and allowing freedom versus maintaining order and control. These are not uncommon clashes. Indeed, issues around the relative importance of one value to another take place continually in organizations at all levels. Who is right or wrong when values clash? This decision can only be made when one set of values is deemed to be higher or more worthy than another set of values. Since values have worth, as many executives are aware, sometimes a problem or a difficult decision is a conflict between right and right (Badaracco, 1998). For example, a healthcare organization’s managers may strongly desire to raise nursing salaries, but also wish to JHHSA FALL 2008 189
- 29. improve patient parking, and only have enough revenue to accomplish one goal. A solution that is often suggested is for managers or management to reflect on the organization’s core values to guide them when making such difficult decisions. This is a worthy suggestion; however, values are generally not the only relevant consideration in many difficult organizational situations. There appears to be considerable overlap, but no real consensus, on what should be included in a list of values. There also is considerable heterogeneity among values, and some appear to be more achievable by human effort than others. For example, two of Rokeach’s instrumental values are logical and intellectual (Rokeach, 1973). How capable is an emotion/feeling-centered person of becoming highly logical or intellectual? Other values propounded by Rokeach may be more attainable, such as being helpful or polite. Writers on organizational values have failed to note that it may be much easier to infuse some values into an organization than others. A dimension closely related to and overlapping with values are human needs and dimensions of personality. Various models or schema of human needs have been posited and widely used in research, consulting, hiring, etc. One model, the FIRO-B developed by William Schutz, describes the primary human needs as being inclusion, control, and affection (Schutz, 1966). Control and affection are not identical to but overlap closely with Rokeach’s values of self-control and being loving (Rokeach, 1973). On the group level, Schutz (1966) posited that the predominant need would change at various stages of the group’s development (e.g., early stage – inclusion; later stage – affection). Organizational group assignments may
- 30. be more successful if the essential values or need profiles of potential members are considered. To state the obvious, a hospital task force to promote caring and compassion 190 JHHSA FALL 2008 should clearly seek to include at least a few members that value affection or being loving. Managers also may seek to stress specific organizational values to group members at the beginning and at various stages of groups’ activity. Leaders in organizations should consider advocating a parsimonious set of values and also determine if these key values are within the scope of the typical organizational member to achieve or internalize. Such reflection will make it far more likely that the final set of organizational values are embraced and actualized Inconsistency in rewards and organizational support. Although differing organizational and personal values may be tacitly accepted by organizational members, they will often have strong and negative reactions when the expressed values of the organization are consistently different from its actual values. This lack of consistency was noted by Kerr (1995) in a reprint of his classic article, “On the Folly of Rewarding A, While Hoping for B.” The article notes the results of a survey (of executives) and describes common conflicts between expressed organizational values and the reward system (e.g., We hope for innovative thinking and risk-taking, but we reward proven methods and not making mistakes. We hope for
- 31. employee involvement and empowerment, but we reward tight control over operations and resources). Thus, conflicting or ambiguous values will be reflected in the reward system, which will contribute to uncertainty about what the organization really wants from employees, and lead to a lack of motivation. Failure to reward organizational members for enacting desired values may at times be the result of the failure of leaders to overcome a crystallized bureaucracy, which continues to reward nonoptimal behaviors and at times to suppress creativity. For example, a staff member JHHSA FALL 2008 191 may have to work through several layers of bureaucracy to implement a novel program or idea. Members of a successful team may not be rewarded as the reward systems that are supported by the bureaucracy do not recognize team achievements. It is clearly not enough to profess important values only at the top of the organization. Those at the top must establish mechanisms that reward those who enact these values. As Kanter (1983, p. 299) noted, “The actions implied by the changes cannot reside on the level of ideas, as abstractions, but must be concretized in actual procedures or structures or communication channels or appraisal methods or work methods or rewards.” When this is accomplished, a vibrant, dynamic working environment is created. An analysis of numerous studies on burnout noted that organizational cultures with little
- 32. burnout among employees had higher job involvement, higher participation in decision-making, greater sharing of information, greater autonomy, and higher supervisor supportiveness than observed in organizations with high levels of burnout (Golembiewski et al., 1996). These observed high levels of participation and involvement in low burnout organizations provide strong evidence of an environment of normative consensus. These organizations also appear to have clearly enacted and concretized their underlying organizational values, which resulted in a positive working environment where employees were unlikely to experience burnout. RECOMMENDATIONS FOR HEALTHCARE MANAGERS In our view there are four key steps or tasks for health care managers who wish to practice values-based leadership. Following these steps should contribute to the development of a truly values-based organization, to less 192 JHHSA FALL 2008 conflict arising from diverse value systems, and the greater integration of the disparate values within an organization. Recognize Your Personal and Professional Values One of the first steps for healthcare managers who wish to uphold and communicate values, is to better understand their own value systems at work. Senge (1990)
- 33. differentiates between our expressed or communicated values (espoused theories) and the values we really act upon (theories-in-use). A healthcare manager may be highly directive and controlling over major projects, yet may really believe she values input and participation. In such cases, Senge believes a manager should do some soul- searching about what he really values in order to learn and grow as an individual and as a manager. Sometimes, Senge asserts, managers need outside input to “see themselves,” because it is often difficult for them to ascertain their own theories-in-use. Determine What You Expect From the Larger Organization and What You Can Implement Within Your Sphere Of Influence Managers need to decide how much they will expect from their healthcare organization, in terms of the regard the organization will exhibit toward its espoused values and how closely the organization will adhere to these values. A few organizations have taken the stance that they will stick to their core values even if it hurts the bottom line or hampers organizational effectiveness. However, most healthcare managers don’t work for such organizations or expect so much from them. Nash (1993) states that a more realistic attitude for managers is to develop organizations that have the normal range of human values and ethical instincts, and for them to work to see that these are not compromised in the workplace. JHHSA FALL 2008 193
- 34. A healthcare manager may work in an organization that she feels doesn’t possess an acceptable value system: or that the leaders espouse certain values, but aren’t really faithful to these values. For the higher level manager or executive, several options exist. An extreme, but sometimes necessary, one is to leave the organization. Another is to work with other like-minded leaders and healthcare professionals to change the organizational culture to be one with strong values that organizational members can embrace and adhere to. However, even when working in an organization without clear and positive values, for lower-level managers there often is considerable scope to enact strong value systems within their own department or bailiwick. As Rosabeth Moss Kanter (1983) stated, organizational changes often work best at the periphery in “zones of indifference,” where no one else cares enough to prevent a little deviance by a lower-level manager. Understand and Incorporate the Values of Internal Stakeholders When healthcare managers are keenly aware of their own professional values, they should also strive to understand and appreciate the value systems of other key stakeholders within the organization. Managers can and should appreciate the value systems of healthcare professionals such as physicians and nurses, who are the most closely involved in helping, serving, and satisfying the organization’s patients. When management and other internal stakeholders work respectfully, openly, and collaboratively to formulate the organization’s values, these values are much more likely to be embraced by all organizational members. Commit to Values-Based Leadership
- 35. Many healthcare executives fail to realize the foundation that values provide for effective organizations. 194 JHHSA FALL 2008 Mayer (2005) noted that “there is a pervasive attitude in the business community that ethics and values are all about restraint and denial, not about active and productive investments.” However, creative healthcare managers who are enthusiastic and committed to an established organizational values system should be able to develop new programs and services that are both financially viable and reflective of the organization’s values. Edgar Schein (1992) asserted that the only thing of real importance that leaders do is to create and manage culture. Organizational values are perhaps the main element in the culture of all dynamic organizations. Effective and influential leaders should not seek to be the sole sources of organizational values, but should include a multitude of internal groups in identifying key values. Once this is accomplished, they should continually communicate the organization’s values and work to assure that these values are not neglected, but are enacted within the organization. This includes structuring reward systems that recognize employees who enact the organization’s values. Leaders also need to stress that the organization’s values not only create a unique and dynamic culture, but also contribute to the competitiveness and success of the organization. Considering the frenetic, demanding world of healthcare management, attention to organizational values
- 36. may seem to some to be a marginal or non-critical issue. For others, attention to values may serve as a moral anchor that helps them to be true to themselves and do their best work in the fast-paced world of healthcare. In the view of the authors, values are clearly the foundation and impetus for a manager who seeks to serve the community and the underserved, to carry out her responsibilities conscientiously, and to communicate honestly and fully with her employees. In our view, those managers with strong personal, professional, and organizational values JHHSA FALL 2008 195 will be the ones most likely not only to succeed, but also to find fulfillment in their professional life. REFERENCES Alexander, A., & Morlock, L. (1994). “Power and politics in health services. In S. Shortell & A. Kaluzny (Eds.), Healthcare management: Organization design and behavior. New York: Delmar Publishers. Badaracco, J. 1998. “The discipline of building character.” In Harvard Business Review on Leadership (pp. 89- 114). Boston, MA: Harvard Business Review. Bass, B.M. (1981). Stogdill’s handbook of leadership. New York: Free Press.
- 37. Blanchard, K., and M. O’Connor. (1997). Managing by values. San Francisco: Berrett-Koehler Publishers. Burns, J.M. (1978). Leadership. New York: Harper and Row. Conger, J. (1998). Winning em’ over. New York: Simon and Schuster. Covey, S. (1991). Principle-centered leadership. New York: Free Press. Golembiewski, R., Boudreau, R., Munzenrider, R., & Luo, H. (1996). Global burnout: A worldwide pandemic explored by the phase model. Greenwich, CT: Jai Press. Hofstede, G. (1980). Culture’s consequences. Newbury Park, CA: Sage Publications. Hojat, M., Mangione, S., Nasca, T., Rattner, S., Erdmann, J., Gonnella, J., & Magee, M. (2004). An empirical study of the decline in empathy in medical school.” Medical Education, 38 (9): 934-41. Kanter, R.M. (1983). The change masters: Innovation for productivity in the American corporation. New York: Simon and Schuster. 196 JHHSA FALL 2008 Kerr, S. (1995). On the folly of rewarding A, while hoping for B. Academy of Management Executive, 9(1): 7-
- 38. 14. Lebow, R., & Simon, W.L. (1997). Lasting change: the shared values process that makes companies great. Hoboken, New Jersey: John Wiley and Sons. Mayer, R. 2005, March. Restoring character and confidence in the workplace: A case for values- based leadership. Presentation at the Caribbean Corporate Governance Forum, Saint Kitts. Merriam-Webster Online Dictionary. 2005. http://www.merriam-webster.com (21 May. 2005). Nash, L. (1993). Good intentions aside: A manager’s guide to resolving ethical problems. Cambridge, MA: Harvard Business School Press. Newton, B., Savidge, M., Barber, L., Cleveland, E., Clardy, J., Beeman, G., & Hart, T. (2000). Differences in medical students’ empathy. Academic Medicine, 75 (12): 1215. Rokeach, M. (1973). The nature of human values. New York: Free Press. Schein, E. (1992). Organizational culture and leadership. (2nd ed.). San Francisco: Jossey-Bass. Schutz, W. (1966). The Interpersonal Underworld. Palo Alto, CA: Science and Behavior Books. Selznick, P. 1957. Leadership in administration. New York: Harper and Row. Senge, P. (1990). The fifth discipline. New York:
- 39. Doubleday. Smolicz, J. 1984. Multiculturalism and an Overarching Framework of Values: Some Educational Responses for Ethnically Plural Societies. European Journal of Education 19 (1): 11-23. Thorpe, K., & R. Loo. 2003. The Values Profile of Nursing Undergraduate Students; Implications for Education JHHSA FALL 2008 197 and Professional Development. Journal of Nursing Education 42 (2): 83-90. Worthley, J.A. (1999). Organizational ethics in the compliance context. Chicago: Health Administration Press.