The Effects of Repetitive Transcranical Magnetic Stimulation Treatment on Major Depression by Qinpu He
•Download as PPT, PDF•
0 likes•1,069 views

Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to The Effects of Repetitive Transcranical Magnetic Stimulation Treatment on Major Depression by Qinpu He
Similar to The Effects of Repetitive Transcranical Magnetic Stimulation Treatment on Major Depression by Qinpu He (20)
More from Brown Fellows Program
More from Brown Fellows Program (20)
The Effects of Repetitive Transcranical Magnetic Stimulation Treatment on Major Depression by Qinpu He
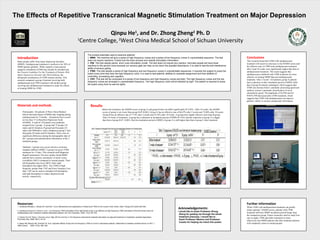
- 1. The Effects of Repetitive Transcranical Magnetic Stimulation Treatment on Major Depression Qinpu He , and Dr. Zhong Zheng Ph. D 1 2 Centre College, West China Medical School of Sichuan University 1 Introduction Many people suffer from major depression disorders (MMD). Antidepressant treatment is ineffective for 30% of MMD patients globally. While repetitive transcranical magnetic stimulation (rTMS) has already be included into the Practice Guideline For the Treatment of Patients With Major Depressive Disorder (the Third Edition), the therapeutic mechanisms of rTMS remains unclear. This research compared a group of patients receiving both antidepressant and rTMS treatment with another group receiving just antidepressant treatment to study the effects of treating MMD by rTMS. Materials and methods Participants: All patients of West China Medical School that had relapse of MMD after stopping taking antidepressant for 3 months. All patients have scored no less than 17 in Hamilton Depression Scale (HAMD). A total of 159 people were randomly assigned into 2 groups. A group had 75 people (18 males and 62 females), B group had 84 people (25 males and 59females) and a comparison group C had 90 people (28 males and 62 females). There were no significant difference among the demographic data of the 3 groups and medicalization information of the 2 treatment groups. 2 The evoked potentials used to examine patients: 1. MMN: The machine will give a series of high frequency voices and a series of low frequency voices in unpredictable sequence. The test does not require reactions. It tests how the brain process and classify stimulation information. 2. P50: This test adopts paired short voice stimulation model. The test does not require any reaction. Normally people will have lower reactions to the second voice because our sensory gate can help us low down the possible disturbance. It is used to test the anti-interference ability of sensory gating. 3. P300: This test adopts a series of high frequency and low frequency voices in unpredictable sequences. It requires the subject to press the button every time they hear the high frequency voice. It is used to test patients’ abilities to complete assignment and their abilities of controlling, processing and cognition. 4. CNV: This test will be composed of a series of low frequency and high frequency voices and light. The high frequency voices and the low frequency voices are arranged in unpredictable frequency. The high frequency voice will be followed by light. The patient is required to press the button every time he see the lights. Conclusions This research found that rTMS with antidepressant treatment will result in a decrease in the HAMD scores and the effective rate of rTMS with antidepressant treatment after 2 and 10 weeks were significantly higher than that of antidepressant treatment. This result suggests that antidepressant combined with rTMS treatment are more effective in treating MMD than just antidepressant treatment. After 2 weeks’ of treatment, group A patients had a reduction in their incubation period of MMN while that of group B remains unchanged, which suggests that rTMS can increase brain’s automatic processing speed and auditory system’s automatic classification of novel stimulations speed. The amplitude of S2-P50 and S2P50/S1-P50 decreased after rTMS treatment, which suggests that rTMS with antidepressant can improve patients’ ability to restrain unimportant information. Results Before the treatment, the HAMD scores of group A and group B does not differ significantly (P>0.05) ; After 10 weeks, the HAMD scores of group A are lower than group B (P<0.001). Group A has an effective rate of 86.67% after 2 weeks and 72.00% after 10 weeks. Group B has an effective rate of 7.14% after 2 weeks and 54.76% after 10 weeks. A groups have higher effective rates than B group. After 10 weeks of treatment, A group has a reduction in incubation period of MMN (P<0.01) and the reduction of group A is bigger than that of group B (P <0.001). But the incubation period of MMN of group A is still higher than that of group C after treatment. Acknowledgemen © File copyright Colin Purrington. You may use for making your poster, of course, but please do not plagiarize, adapt, or put on your own site. Also, do not upload this file, even if modified, to third-party file-sharing sites such as doctoc.com. If you have insatiable need to post a template onto your own site, search the internet for a different template to steal. File downloaded from http://colinpurrington.com/tips/academi c/posterdesign. Methods: 3 groups were given selective serotonin reuptake inhibitor (SSRI). A group was given rTMS treatment for 15 days. This research used Magnstim Rapid2 instruments. Previous studies found MMD patients have contrary asymmetry of motor cortex excitability (MCE) compared to normal people. Their left hemisphere has lower MCE while right hemisphere has higher MCE. The rTMS of high frequency greater than 5 HZ and lower frequency less than 1 HZ can be used to stimulate left hemisphere and right hemisphere to reduce depression and anxiety, respectively. Resources: 1. Cárdenas-Morales L, Nowak DA, Kammer T,et al. Mechanisms and applications of theta-burst rTMS on the human motor cortex. Brain Topogr,2010;22(4):294-306. 2. Isenberg K,Downs D, Pierce K, et al . Low frequency rTMS stimulation of the right frontal cortex is as effective as high frequency rTMS stimulation of the left frontal cortex for antidepressant-free, treatment-resistant depressed patients. Ann Clin Psychiatry, 2005 ;17(3):153-159. 3. Garcia-Toro M, Salva J, Daumal J,et al. High (20-Hz) and low (1-Hz) frequency transcranial magnetic stimulation as adjuvant treatment in medication-resistant depression. Psychiatry Res, 2006;146(1): 53–57. 4. Speer AM, Benson BE, Kimbrell TK, et al. Opposite effects of high and low frequency rTMS on mood in depressed patients: relationship to baseline cerebral activity on PET. J Affect Disord , 2009;115(3): 386–394. Further information Acknowledgements: I would like to thank Professor Zhong Zheng for guiding me through the whole treatment preocess. I would like to thank Professor Weston and Professor Cusato for helping me check this poster. While rTMS with antidepressant treatment can greatly reduce patients’ HAMD scores, patients with rTMS treatment still have MMN incubation period longer than the comparison group. Future researches need to study how can we apply rTMS and other treatments to more effectively treat MMD patients that after treatment patients will completely return to normal people.
Editor's Notes
- <number>