1. 37Glucocorticoids Reduce Astrocyte Numbers
PP
P
Glial
Number
in
PFC
for
Mood
Disorders
15
10
5
x106
Glial
Number
37Glucocorticoids Reduce Astrocyte Numbers
cells reported that GR knockdown promoted cell prolif-
eration, which is in contrast to our results (21). This
discrepancy suggests that the relationship between GR
expression and cell proliferation may depend on cell
type. The mechanisms by which GR regulates cell prolif-
eration should be determined in future research.
PP
P
Fig. 7. Repeated adrenocorticotropic hormone (ACTH) administration decreased glucocorticoid receptor (GR) expression and
the number of astrocytes in vivo. A, B: GR expression in the frontal cortex (A) and hippocampus (B) after 14 days of saline or
ACTH administration. The bottom graphs show the quantified data of the GR/GAPDH ratio. n = 3. C: GFAP and GAPDH were
detected by western blotting in the frontal cortex after 14 days of repeated ACTH administration. D: Neuronal nuclei (NeuN)- or
GFAP-positive cells were stained by immunohistochemistry and their numbers calculated from 30 slices. E: Representative pic-
tures show GFAP-positive cells in the prefrontal cortex of rats administered with saline or ACTH for 14 days. Scale bar = 50
μm.
Chronic Stress as a Potential Non-Genetic Cause for Bipolar Disorder
Anant Naik1, Bhavani Murakonda1, Atsushi Asakura2
1Department of Biomedical Engineering, University of Minnesota Twin Cities, 2Department of Neurology, University of Minnesota Twin Cities
A.
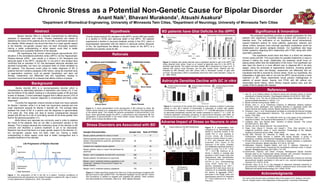
Figure 3: Patients with bipolar disorder have a significant decline in glia in the dlPFC. A)
Using obtained brain slices, Ongur et al. looked at Agranular area 24 in the dlPFC to
ascertain glial density. This region has been shaded. B) A comparison by Ongur et al. of
patients with various mood disorders, and the glial number found. Patients with BD,
indicated by fBD (familial) and oBD (other) have a decreased number of glial cells
(p<0.05). The decrease in fBD is substantially lower than other mood disorders. (Ongur et
al., 1998, PNAS)
References
1. Aas, M., et al. Additive effects of childhood abuse and cannabis abuse on clinical
expressions of bipolar disorders. Psychological medicine 44.08 (2014): 1653-1662.
2. Aas, Monica, et al. The role of childhood trauma in bipolar disorders. International
journal of bipolar disorders 4.1 (2016): 1-10.
3. Bipolar Disorder Among Adults. NIMH. n.d.
4. Brooks, John O., et al. Preliminary evidence of differential relations between
prefrontal cortex metabolism and sustained attention in depressed adults with
bipolar disorder and healthy controls. Bipolar disorders 8.3 (2006): 248-254.
5. Cerqueira, Joao J., et al. Morphological correlates of corticosteroid-induced changes
in prefrontal cortex-dependent behaviors. The Journal of Neuroscience 25.34
(2005): 7792-7800.
6. Cerqueira, João J., et al. The prefrontal cortex as a key target of the maladaptive
response to stress. The Journal of Neuroscience 27.11 (2007): 2781-2787.
7. Craddock, Nick, and Pamela Sklar. Genetics of bipolar disorder. The Lancet
381.9878 (2013): 1654-1662.
8. Grande, Iria, et al. Bipolar disorder. The Lancet (2015).
9. Öngür, Dost, Wayne C. Drevets, and Joseph L. Price. Glial reduction in the
subgenual prefrontal cortex in mood disorders. Proceedings of the National
Academy of Sciences 95.22 (1998): 13290-13295.
10. Otto MW, Perlman CA, Wernicke R, Reese HE, Bauer MS, Pollack MH.
Posttraumatic stress disorder in patients with bipolar disorder: a review of
prevalence, correlates, and treatment strategies. Bipolar Disord 2004: 6: 470–479.
11. Pompili, Maurizio, et al. Epidemiology of suicide in bipolar disorders: a systematic
review of the literature. Bipolar disorders 15.5 (2013): 457-490.
12. Rajkowska, Grazyna, Angelos Halaris, and Lynn D. Selemon. Reductions in
neuronal and glial density characterize the dorsolateral prefrontal cortex in bipolar
disorder. Biological psychiatry 49.9 (2001): 741-752.
13. Salzbrenner, Stephen, and Eileen Conaway. Misdiagnosed Bipolar Disorder
Reveals Itself to be Posttraumatic Stress Disorder with Comorbid Pseudotumor
Cerebri: A Case Report. Psychiatry (Edgmont) 6.8 (2009): 29.
14. Unemura, Kazuhiro, et al. Glucocorticoids decrease astrocyte numbers by reducing
glucocorticoid receptor expression in vitro and in vivo. Journal of pharmacological
sciences 119.1 (2012): 30-39.
15. Vermeer, Harry, et al. An in vitro bioassay to determine individual sensitivity to
glucocorticoids: induction of FKBP51 mRNA in peripheral blood mononuclear cells.
Molecular and cellular endocrinology 218.1 (2004): 49-55.
HypothesisAbstract
Background
Rationale
Stress Disorders are Associated with BD
Astrocyte Densities Decline with GC in vitro
Adverse Impact of Stress on Neurons in vivo
Significance & Innovation
Sample
Characteris7cs Sample
Size Rate
of
PTSD%
Bipolar patients admitted for mania or mixed 71 17
National general population survey: respondents with
bipolar I characterized by euphoria, grandiosity, and
excessive energy
29 39
Inpatient and outpatient bipolar patients 50 40
Bipolar patients, manic or mixed: first admission for
psychosis
77 21
Bipolar I and II outpatients recruited from community 288 7
Bipolar patients: first admission for psychosis 102 11
Bipolar I and II, treatment-seeking outpatients in the
Systematic Treatment Enhancement Program for
bipolar disorder
475 17
Bipolar I and II, treatment-seeking outpatients 122 19
Figure 5: A representation from
Cerquiera et. al. demonstrating the
decline in neuronal number in the
medial PFC in mice exposed to
chronic stress. A) Volumetric
decline in neurons shown in Layer I,
II, III-VI, and molecular (Mol) and
pyramidal (Pyr) layers of the
subiculum of the cortex. Dramatic
and statistically significant decline is
evident in Layer I & II (*P < 0.05,
**P < 0.01) B) Unemura et al.
shows a decline in average glial
densities in both Frontal Cortex and
Hippocampus after administration
of Adrenocorticotropic Hormone
(ACTH) in vivo, immunostaining
using GFAP. Scale bar = 50
microns. (Cerqueira et al., 2007, J
Neurosci) C) A pilot study done by
Unemura et al presented showing
the decline of aggregate GFAP+
astrocytes in the frontal cortex and
hippocampus post-ACTH treatment
(P < 0.05) (Unemura et al., 2012, J
Phar Sci.)
Chronic stress-induced GC elevation in the dlPFC via the HPA axis results
in a decline in GCRs and astrocyte death in the dlPFC. BD patients
experienced a decline in neuronal metabolic activity in the PFC, which is
physiologically associated with the decline in astrocyte activity. Because
of this, we hypothesize the effects of chronic stress on the dlPFC is a
potential non-genetic cause for BD.
Bipolar disorder (BD) is a neuroprogressive disorder which is
characterized by alternating episodes of depression and mania (12). It can
last the lifetime of the patient, leading to a decreased quality of life and high
burden of disease. Current estimates suggest that it affects around 2.6% of
the national population, however diagnosis is complicated and likely under
diagnosed.
Currently the diagnostic criteria includes at least one manic episode
for Bipolar I disorder, while it is at least one hypomanic episode and one
major depressive episode for Bipolar II disorder (8). The average delay
between the onset of BD in a person and the diagnosis is approximately
5-10 years (8). This delay can lead to severe consequences because
people with BD are at a risk of committing suicide 20-30 times greater than
that for the general population (11).
While lithium and valproate are commonly used in order to stabilize
the mood of the patients, they do not offer a permanent solution to the
disease. This is largely because the underlying cause of the disorder is still
unknown and therefore a curative treatment is yet to be discovered.
Research has found that there is a major genetic aspect to the disorder (7),
but non-genetic causes have not been ruled out. Having a better
understanding in either aspect could lead to better management and a
possible treatment of the disorder.
The proposed hypothesis provides a possible explanation for why
patients who experience incredible stress develop BD compared to a
baseline level. The verification of our hypothesis would tremendously
expand treatment options for many patients, particularly veterans and
abuse victims, because more thorough psychiatric evaluations would be
emphasized over genetic pedigree analysis. Our hypothesis also begs
further questions regarding BD’s relationship with PTSD, along with other
psychiatric disorders.
This hypothesis would show that there is a direct link between
chronic stress and BD. This would allow for possible treatments or ways to
prevent it before the onset. Additionally, the treatment would focus on
easing stress rather than the stabilization of the mood. This hypothesis can
also open the doors to a more efficient way to diagnose BD in its early
stages. Using the principles of regenerative medicine, including genetic
transfection and stem cell therapy, researchers can effectively test our
hypothesis that BD is induced by chronic stress. Given our hypothesis, the
implantation of glial stem cells in vivo into the dlPFC would provide a novel
treatment to BD. These experiments would prevent misdiagnoses of
patients of sexual abuse, trauma, and PTSD with BD without any
discernable family history, which directly impacts patient care, and the
quality of life for people with disease.
A.
B.
34 K Unemura et al
results suggest that glucocorticoids inhibited astrocyte
proliferation and reduced GR expression mediated via
GR.
GR knockdown led to a reduction in astrocyte numbers
To investigate the relationship between reduction in
GR expression and inhibition of astrocyte proliferation
by glucocorticoids, siRNA targeting GR was transfected
Fig. 2. Corticosterone (CRT) and dexamethasone (DEX) reduced the number of astrocytes via a glucocorticoid receptor but did
not induce astrocytic damage. A, B: The 3-(4,5-dimethyl-2-thiazolyl)-2,5-diphenyltetrazolium bromide (MTT) assay was per-
formed 72 h after treatment with CRT (0.01 – 1 μM) and DEX (0.01 – 1 μM). C: The lactate dehydrogenase (LDH) assay was
performed 72 h after treatment with CRT (1 μM) and DEX (1 μM) or 24 h after treatment with H2O2 (1 mM). D, E, F: The MTT
assay was performed 72 h after treatment with CRT (1 μM); DEX (1 μM); RU486 (0.3 – 3 μM), a GR antagonist; and eplerenone
(10 μM), a mineralcorticoid receptor antagonist. n = 4. ***P < 0.001 vs. control, ###
P < 0.001 vs. CRT or DEX alone. n.s., not
significant.
Fig. 3. Reduction in astrocyte prolif-
eration by corticosterone (CRT) and
dexamethasone (DEX) via a glucocor-
ticoid receptor. Bromodeoxyuridine
(BrdU)- and GFAP-positive cells were
detected 48 h after treatment with CRT
(1 μM), DEX (1 μM), and RU486 (3
μM) plus BrdU (1 μM). A: CRT, B:
DEX. n = 8. **P < 0.01, ***P < 0.001
vs. control; #
P < 0.05, ###
P < 0.001 vs.
CRT or DEX alone.
34 K Unemura et al
results suggest that glucocorticoids inhibited astrocyte
proliferation and reduced GR expression mediated via
GR.
GR knockdown led to a reduction in astrocyte numbers
To investigate the relationship between reduction in
GR expression and inhibition of astrocyte proliferation
by glucocorticoids, siRNA targeting GR was transfected
Fig. 2. Corticosterone (CRT) and dexamethasone (DEX) reduced the number of astrocytes via a glucocorticoid receptor but did
not induce astrocytic damage. A, B: The 3-(4,5-dimethyl-2-thiazolyl)-2,5-diphenyltetrazolium bromide (MTT) assay was per-
formed 72 h after treatment with CRT (0.01 – 1 μM) and DEX (0.01 – 1 μM). C: The lactate dehydrogenase (LDH) assay was
performed 72 h after treatment with CRT (1 μM) and DEX (1 μM) or 24 h after treatment with H2O2 (1 mM). D, E, F: The MTT
assay was performed 72 h after treatment with CRT (1 μM); DEX (1 μM); RU486 (0.3 – 3 μM), a GR antagonist; and eplerenone
(10 μM), a mineralcorticoid receptor antagonist. n = 4. ***P < 0.001 vs. control, ###
P < 0.001 vs. CRT or DEX alone. n.s., not
significant.
Fig. 3. Reduction in astrocyte prolif-
eration by corticosterone (CRT) and
dexamethasone (DEX) via a glucocor-
ticoid receptor. Bromodeoxyuridine
(BrdU)- and GFAP-positive cells were
detected 48 h after treatment with CRT
(1 μM), DEX (1 μM), and RU486 (3
μM) plus BrdU (1 μM). A: CRT, B:
DEX. n = 8. **P < 0.01, ***P < 0.001
vs. control; #
P < 0.05, ###
P < 0.001 vs.
CRT or DEX alone.
36 K Unemura et al
These results suggest that secretion of high concentra-
tions of glucocorticoids induced by repeated ACTH ad-
ministration leads to a reduction in both GR expression
and the number of astrocytes in vivo.
Discussion
This study investigated the mechanism by which glu-
cocorticoids inhibit astrocyte proliferation. The results
demonstrated a relationship between astrocyte prolifera-
tion and GR expression following treatment with gluco-
corticoids. This was demonstrated in an animal model (in
vivo) as well as cultured astrocytes (in vitro). In sum-
mary, our results suggest that glucocorticoids reduce
astrocyte proliferation by inducing a reduction in GR
expression.
In the first experiment, the subcellular localization of
GR was observed in cultured astrocytes, with GR found
to be primarily expressed in the nuclei (Fig. 1). Neuronal
GR performs functions other than gene transcription, for
example, GR interacts with receptor tyrosine kinase for
BDNF (trkB) and promotes glutamate release (20). In
contrast, functions of astrocytic GR other than the func-
tion of binding to a glucocorticoid have not yet been re-
ported. Based on our results, we assumed that astrocytic
as well as neuronal GRs have some unknown functions
in our culture conditions.
Corticosterone and dexamethasone reduced the num-
ber of astrocytes via GR by inhibiting astrocyte prolifera-
tion (Figs. 2 and 3). These results are consistent with
those of a previous report that suggested that the neural
cell adhesion molecule (NCAM) inhibited astrocyte
proliferation via GR (16). In neurons and astrocytes, GR
expression has also been shown to change with glucocor-
ticoid administration in vitro (19). The mechanisms by
which GR expression affects astrocyte function are
largely unknown. We showed that short-term (1 – 6 h)
glucocorticoid treatment increased GR expression,
whereas long-term (> 12 h) treatment decreased GR ex-
pression. RU486 also increased GR expression in a short
term; however, this expression did not decrease subse-
quently (Fig. 4). We examined the effect of RU486 on
the glucocorticoid-induced change in GR expression. GR
expression increased by glucocorticoid treatment was
enhanced by RU486, whereas GR expression reduced by
glucocorticoid treatment was inhibited by RU486 (Fig.
5).
We hypothesized that reduced GR expression follow-
ing long-term glucocorticoid treatment plays a crucial
role in astrocyte proliferation. To validate this hypothesis,
we used siRNA to silence GR. GR knockdown reduced
the number of astrocytes by inhibiting their proliferation
(Fig. 6). GR antagonism by RU486 did not induce pro-
motion of astrocyte proliferation. We suppose that this is
because RU486 does not decrease GR expression in as-
trocyte. Thus, we propose that prolonged reduction in
GR expression inhibits proliferation of cultured astro-
cytes. However, another study using murine macrophage
Fig. 6. Glucocorticoid receptor (GR)
knockdown reduced astrocyte prolifera-
tion. A: Representative western blotting
example of GR and GAPDH 96 h after
siRNA transfection. B: Quantification of
the GR/GAPDH ratio in panel A. n = 4.
C: The MTT assay was performed 120 h
after siRNA transfection. n = 4. D: BrdU-
positive cells were detected 48 h after
BrdU treatment (1 μM) 72 h after siRNA
transfection. n = 8. *P < 0.05, ***P <
0.001 vs. control siRNA.
Figure 4: A summary of the results from Unemura et al. showing a decline in astrocyte
density in vitro. A) A decline of functionality in astrocytes is evident with greater
concentrations of cortisone compared to control (*** P < 0.05) B) Application of cortisone
on astrocytes dramatically reduced cell number compared to control (*** P < 0.05). C)
Cortisone application decreases prevalence of Glucocorticoid Receptor (GR) RNA, an
indicator for the prevalence of GR in cells (*P < 0.05). (Unemura et al., 2012, J Phar Sci.)
A. B. C.
Figure 3: A table describing results from Otto et al. A high percentage of patients with
BD were found to also exhibit PTSD. The National Population Survey with BD I shows
39% prevalence, in addition to Inpatient and outpatient BD patients. Other numbers
also demonstrate the comorbidity. (Otto et al., 2004, Bipolar Disorder)
Bipolar disorder (BD) is a disorder characterized by alternating
episodes of depression and mania. Present treatments are aimed at
stabilizing the mood of the patients and do not offer a permanent solution to
the disease. While research has found that there is a major genetic aspect
to the disorder, non-genetic causes have not been thoroughly explored.
Having a better understanding in either aspect could lead to better
management and a possible treatment of the disorder.
We hypothesize that chronic stress-induced glucocorticoid (GC)
elevation in the dorsolateral prefrontal cortex (dlPFC) via the Hippocampal-
Pituitary-Adrenal (HPA) axis results in a decline in GC Receptors and
astrocyte death in the dlPFC, causing BD. In vivo and in vitro studies have
confirmed that an elevation in GC has decreased astrocyte densities and
declined functionality, but have not compared them to levels exhibited by
BD patients. This discovery would allow for better diagnosis of BD in
patients that don’t exhibit a pedigree of BD history. Using the important tools
of regenerative medicine, such as genetic transfection and stem cell
therapy, researchers can effectively test this hypothesis, leading to
important novel treatments for a disease that affects millions of people.
B.
Neuron
Astrocyte
Blood vessel
GC
Neuron
Blood vessel
GC
Degeneration
of Astrocyte
In Prefrontal Cortex
Bipolar Disorder
Figure 2: A visual representation of the development of BD induced by stress. A)
Chronic stress results in an upregulation of the HPA axis, resulting in the hyperactivity
of the adrenal gland. This creates the adverse upregulation of glucocorticoids in the
blood, which specifically targets the dlPFC, a phenomenon less understood. B) The
upregulation of glucocorticoids in the blood stream causes astrocyte death in the
dlPFC, which induces the effects of BD.
A. B.Cerebrum and Cerebellum Prefrontal Cortex
Endocrine GC
Feedback to
stress
Endocrine
response to
stress
Adrenal Gland
GC release due
to stress
PFC
Stress
Hypothalamus
Bipolar Disorder
Blood Vessel
Blood Vessel
Neuron
Neuron
Astrocyte
Degeneration
of Astrocyte
Figure 1: The progression of BD in the life of a patient. Transient oscillations of
hypomania/mania and depression are evident throughout a patient’s life. Age of onset is
in early adolescence (Grande et al., 2015, The Lancet)
Life Progression of Bipolar Disorder
Mania
Hypomania
Euthymia
Subthreshold
Depression
Major Depression
Mixed State
Severityof
Mania
Severityof
Depression
C.
BD patients have Glial Deficits in the dlPFC
Cor7sone
Impact
on
Astrocyte
Func7onality
Cor7sone
Impact
on
Astrocyte
Number
Cor7sone
Impact
on
GR
RNA
Prevalence
Acknowledgments
Our work could not have been completed without the support of Dr. Asakura, and input
from Dr. Russell Carter in the Department of Neuroscience, University of Minnesota.
Volume
of
Neurons
in
the
mPFC
Pre/Post-‐Stress
ACTH
impact
on
Astrocytes
in
vivo
Saline
ACTH