Rop laser
•Download as PPTX, PDF•
0 likes•11 views

Got an opportunity to join virtual laser course on last year , i add on some pictures for better comprehension & appreciation.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Rop laser
Similar to Rop laser (20)
More from Azul .
Recently uploaded
Recently uploaded (20)
Rop laser
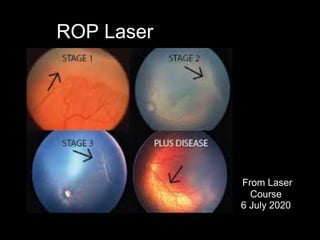
- 1. ROP Laser From Laser Course 6 July 2020
- 2. Retinopathy of prematurity • Vasoproliferative disorder unique to premature infants • Classified according to ICROP (International Classification of ROP)
- 3. Principles of treatment • Early detection • Appropriate treatment within specified time frame • Screening criteria 1. Birth weight: 1.5kg and below 2. Gestational age: 32 weeks and below
- 4. Screening Guidelines Gestational age at birth Age at initial examination(weeks) Post-conceptional age Post-natal age 22 31 9 23 31 8 24 31 7 25 31 6 26 31 5 27 31 4 28 32 4 29 33 4 30 34 4 31 35 4 32 36 4
- 5. Why screen at 31 weeks and above? • ROP has two phases: the vaso-obliterative (hyperoxic ) phase and the vaso-proliferative (neovascularization) phase • The neovascularization phase occurs at 31-44 weeks • If screened less than 31 weeks, poor pupil dilatation and tunica vasculosa lentis hinders fundal examination • >99% of sight-threatening ROP is detected within 31-46 weeks of ROP screening
- 6. When to treat • Zone I, any stage with plus • Zone 1, stage 3 with/without plus • Zone II, stage 2 or 3, wi t h plus Type 1 ROP (High-risk prethreshold) • 5 continuous / 8 total clock hours stage 3 • zone I or II • plus Threshold ROP • Prominent Plus • Zone I (posterior) • Deceptively featureless retina neovascularization APROP (Aggressive Posterior ROP)
- 7. When to laser? • Within 24 hours • Max: 72 hours!
- 8. Based on principle of retinal ablation. Treatment is directed to the avascular part of the retina with the goal of decreasing the production of angiogenic growth factors. The effectiveness of cryotherapy/ laser in reducing poor visual and structural outcomes of eyes with threshold ROP is well established. The effectiveness of intravitreal injection of antivascular endothelial growth factor antibodies as treatment for ROP is under study.
- 9. Why laser in ROP? • Disease regression of 71-100% • Superior visual outcomes to cryo • Less morbidity • Less eye manipulation • Less traumatic • More effective for zone 2 and zone 1 disease
- 10. Preparation for laser • Laser machine • 28D or 30D lens • Goggles • BSS • Mydriacaine • Scleral indentors • Conjunctival forceps • Disposable dressing set • Tuberculin syringes • Gauze (Loads!)
- 11. Preparation for laser • Dark-room • Screens to protect staff • Neonatal staff on standby • Anaesthesia
- 12. Anaesthesia for laser Anaesthesia General Sedation Local - topical - subtenon
- 13. Types of ROP lasers • Diode (810)nm • Argon green (514nm) • Frequency-doubled Nd-YAG (532nm green)
- 14. Laser settings • Power: 200mW • Duration: 0.10 seconds • Interval : 0.10 seconds • NO SPOT SIZE! • Titrate upwards to get moderate intensity GREY burns
- 15. Laser method • Ablade avascular retina • Test shots • Barricade shots • Moderate intensity • Near-confluent burns
- 16. How much is enough laser? • All avascular areas fully lasered • 2000-3000 shots per eye • Takes average of 45 mins to one hour per eye
- 17. Prevention of skip lesions • Multiple indentors • Recheck laser sites • Two people
- 18. APROP laser • Laser till mid-periphery • Allow area for retina to grow • May need re-treatment later • Intravitreal VEGF
- 19. Post-laser management • Steroid-antibiotic eyedrops for two weeks • Review post-laser day one for trauma or infection • Review fundus one week post-laser • Weekly reviews for regression
- 20. Signs of regression of ROP • Good pupil dilatation • Clear media • Regression on neovascularization • Normal feeder vessles • Flattening ridge • No traction
- 21. Laser treatment complications • Under-treatment • Overtreatment (retinal breaks, choroidal bleeds, exudative RD, VH) • Anterior segment trauma • Cataract • Myopia • Reduced night vision • Visual field defects
- 22. Laser ROP FAQs • What if the pupil doesn’t dilate? 1. Did not dilate pupil prior to procedure 2. Pupil constricts due to morphine 3. Iris tauma from laser burns 4. Plus disease • Adequate pupil dilatation • Subconjunctival mydriacaine 0.05ml/eye (aseptic technique)
- 23. Laser ROP FAQs • Why is the cornea hazy during ROP? 1. Irrigating solution 2. Vigorous indentation 3. Corneal trauma • View is hazy during half- way through laser 1. Hit blood vessel 2. Excessive inflammation
- 24. Laser ROP FAQs • Baby unstable for laser under GA • Liase with neonatologists • Consider sedation with LA (topical +subtenon) • LA (topical +subtenon) • Intravitreal anti-VEGF
- 25. Thank you
Editor's Notes
- by location (zones) and severity (stages), as well as defines plus and pre-plus disease, was updated in 2005 Stage 1 Demarcation line separates avascular from vascularized retina Stage 2 Ridge arising in region of demarcation line Stage 3 Extraretinal fibrovascular proliferation/neovascularization Stage 4 Partial retinal detachment Stage 5 Total retinal detachment Pre-plus disease More vascular tortuosity than normal, but insufficient for diagnosis of plus disease Plus disease Vascular dilation and tortuosity of at least two quadrants of the eye
- ROP takes the longest to develop in the most immature infants. Data from two large clinical trials – the Multicenter Trial of Cryotherapy (CRYO-ROP) study and the Light Reduction in Retinopathy of Prematurity (LIGHT-ROP) study
- ROP takes the longest to develop in the most immature infants. Data from two large clinical trials – the Multicenter Trial of Cryotherapy (CRYO-ROP) study and the Light Reduction in Retinopathy of Prematurity (LIGHT-ROP) study Infants with GA of 26 6/7 weeks or less at birth – initial screen at 31 weeks’ PMA; Infants with GA of 27 weeks or more at birth – initial screen at four weeks’ CA.
- 99% of prethreshold ROP develops by 45 weeks’ PMA Duration of acute ROP screening Cessation of ROP screening depends on eye findings and PMA. AAP indications for stopping screening examinations include the following: Complete vascularization; Zone III vascularization without previous zone I or II ROP; PMA of 45 weeks and no prethreshold disease or worse ROP; Regression of ROP.
- (APROP) is characterized by severe plus disease, flat neovascularization in zone 1 or posterior zone 2, intraretinal shunting, hemorrhages, and a rapid progression to retinal detachment. Retinal ablative therapy should be considered for high-risk prethreshold ROP: Zone I – any stage ROP with plus disease. Zone I – stage 3 ROP with or without plus disease. Zone II – stage 2 or 3 ROP with plus disease. Retinal ablative therapy should be performed for threshold ROP (at least five contiguous or eight cumulative clock hours of stage 3 ROP in zone 1 or 2 in the presence of plus disease). Treatment should be performed within 72 h of examination.
- Principle of retinal ablation. Treatment is directed to the avascular part of the retina with the goal of decreasing the production of angiogenic growth factors. The effectiveness of cryotherapy and laser photocoagulation (the preferred treatment method) in reducing poor visual and structural outcomes of eyes with threshold ROP is well established (2). However, despite treatment, the incidence of unfavourable outcome for these infants remains significant. Results of the Early Treatment for Retinopathy of Prematurity (ETROP) randomized trial (20) have shown that treatment of eyes with high-risk prethreshold ROP further reduced unfavourable visual acuity and structural outcomes. Based on the results of this trial, indications for treatment have been refined. The effectiveness of intravitreal injection of antivascular endothelial growth factor antibodies as treatment for ROP is under study.
- Near-confluent ablation of peripheral avascular retina, burns space one half burn width apart, from orra serrata up to ridge for 360 degree