2. Contents
1. Definition
2. History
3. Incidence
4. Pathophysiology
5. Bell's staging
6. Investigation
7. New modalities of investigation
8. Management
9. Complications
2
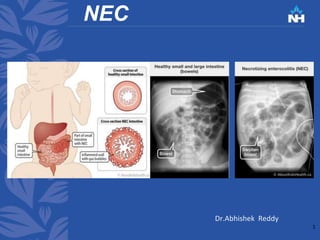
3. Definition
Necrotizing enterocolitis is an acquired disease, primarily
of preterm or sick neonates, characterized by mucosal or
even deeper intestinal necrosis. It is the most common GI
emergency among neonates.
3
4. History
NEC was unknown till 1953 when it was coined by
Schmid and Quaiser.
Previously it was described under idiopathic
gastrointestinal perforation
4
5. Incidence
incidence of NEC in babies less than 32 weeks
gestation was 5.2%(india)
Incidence varies from region to region
1-2 %in Japan
7% in Australia
10% in Greece
14% Argentina
28% in hong kong
Reason for disparity is unknown (Multifactorial)
5
Neonatal necrotizing enterocolitis an epidemiological study.
Narang A, Rao R, Bhakoo ON
Indian Pediatr. 1993 Oct; 30(10):1207-14.http://www.indianpediatrics.net/oct1993/1207.pdf
13. According to Neuhauser study in infants with NEC having
perforation
63% of infants with perforation present with
pneumoperitoneum
21% had radiographic evidence of ascites but no
pneumoperitoneum,
and 16% had neither free air nor
ascites.
1. NEUHAUSER EB, WITTENBORG MH. Pediatric radiology. N Engl J
Med. 1953;249(2):62–8. https://doi.org/10.1007/bf02396612 13
15. USG:
1. Free fluid, especially with echogenic debris, suggests
perforation
2. Bowel wall thickening
15
16. Role of contrast study:
• Not done for diagnosis of NEC
• Done after the NEC has resolved and in those
having features of obstruction to rule out
strictures
16
17. Newer modalities for diagnosing NEC
Urinary I-FABP levels are not suitable as screening
tool for NEC before clinical suspicion. However,
urinary I-FABP and claudin-3 and
fecal calprotectin are promising diagnostic markers
for NEC.
1. Thuijls G, Derikx JPM, Wijck K Van, Zimmermann LJI. Non-Invasive Markers for Early Diagnosis and
Determination of the Severity of Necrotizing Enterocolitis. 2010;
https://doi.org/10.1097/SLA.0b013e3181d778c4
17
18. In future…..
https://doi.org/10.1016/j.jpedsurg.2018.02.083
1. Goldstein SD, Beaulieu RJ, Niño DF, Chun Y, Banerjee A,
Sodhi CP, et al. Early detection of necrotizing enterocolitis
using broadband optical spectroscopy. J Pediatr Surg
18
Early detection of necrotizing
enterocolitis using broadband
optical spectroscopy
spectral waveforms from mice
with NEC.
When subsequently tested on
cohorts of diseased and control
mice by a blinded examiner,
noninvasive BOS
was able to detect disease with
100% specificity and sensitivity.
20. Management
Non operative : in absence of intestinal necrosis or
perforation
NPO
Ng tube
Labs:CBC,CRP,Blood gas analysis , serum
electrolytes.
Broad spectrum antibiotics (Vancomycin &
Gentamycin/Cefalosporins 3rd gen) for 7-14 days
Frequent clinical examination and radiography
20
21. • Once the infant is clinically well small
volume feeds are started .
• Stools are to be tested for reducing
substance and occult blood .
• Feeding is discontinued if either of this
tests are positive .
21
22. Indications for operation
Main goal is to remove the gangrenous
bowel and preserve intestinal length
Widely accepted indication to operation is -
Pneumoperitoneum
Relative indications for operations:
Positive paracentesis, Palpable mass,
abdominal wall erythema, portal vein gas,
fixed intestinal loop, Clinical detrioration
despite medical management 22
24. • The DAAS provides a standardized 10-point radiographic
scale that increases with disease severity when using
need for surgical intervention as a surrogate for severe
NEC. For every 1-point increase in the DAAS score,
patients were statistically significantly more likely to
have severe disease as measured by need for surgical
intervention
• 93% of operated infants in study have a Duke abdominal
assessment score >7
1. Coursey CA, Hollingsworth CL, Wriston C, Beam C, Rice H, Bisset G.
Radiographic predictors of disease severity in neonates and infants with
necrotizing enterocolitis. Am J Roentgenol. 2009;193(5):1408–13.
10.2214/AJR.08.2306
24
25. Paracentesis: positive result on
paracentesis is defined as free flowing
aspiration of more than 0.5 ml of brown
or yellow -brown fluid that contains
bacteria on gram stain highly specific for
intestinal necrosis.
25
26. Poratal venous gas :
hepatic portal venous gas not an indication for surgery
since 47% of infants with NEC and HPVG survive without
operative procedure.
Fixed bowel loops :
Peristent location of bowel loop for more than 24 hrs.
It is a relative indication for operation
Half of the patients with fixed loop recover without
operation
1. Abboud B, El Hachem J, Yazbeck T, Doumit C. Hepatic portal venous gas:
Physiopathology, etiology, prognosis and treatment. Vol. 15, World Journal of
Gastroenterology. 2009. p. 3585–90. https://doi.org/10.3748/wjg.15.3585 26
27. Operative management
Primary peritoneal drainage:
PPD was used in infants < 1000gm at birth with
perforated NEC to allow resuscitation and stabilisation
before definitive laparotomy.
According to Rees(1) Peritoneal drainage does not
immediately improve clinical status in extremely low
birth weight infants with bowel perforation. The use of
PD as a stabilizing or temporizing measure is not
supported
1. Trial NET, Rees CM, Eaton S, Khoo AK, Kiely EM. Peritoneal drainage does not stabilize
extremely low birth weight infants with perforated bowel : data from the. J Pediatr Surg
[Internet]. 2010;45(2):324–9. Available from:
http://dx.doi.org/10.1016/j.jpedsurg.2009.10.066 27
28. Laparotomy :
1. Resection with enterostomy
2. Resection with anastomosis
3. Proximal enterostomy
4. Clip and drop technique
5. Patch drain
6. Wait technique
28
29. Mortality
Regardless of birth weight, surgical NEC showed a
mortality at approximately 30%.
The laparotomy alone and drainage with laparotomy
groups had similar mortalities, while the drainage
alone treatment cohort was associated with the
highest mortality.
Surgical -31%
Surgical and PPD 34%
PPD-50%
Medically treated -21%
1. Hull MA, Fisher JG, Gutierrez IM, Jones BA, Kang KH, Kenny M, et al. Mortality and Management of
Surgical Necrotizing Enterocolitis in Very Low Birth Weight Neonates : A Prospective Cohort Study. J Am
Coll Surg [Internet]. 2013; Available from: http://dx.doi.org/10.1016/j.jamcollsurg.2013.11.015 29
30. 1. Hull MA, Fisher JG, Gutierrez IM, Jones BA, Kang KH, Kenny M, et al. Mortality and Management of Surgical
Necrotizing Enterocolitis in Very Low Birth Weight Neonates : A Prospective Cohort Study. J Am Coll Surg [Internet].
2013; Available from: http://dx.doi.org/10.1016/j.jamcollsurg.2013.11.015 30
31. Complications
Gastrointestinal:
Intestinal stricture-
Most common site for stricture formation is colon(80%),
it is more frequently associated with non operative
management
Of the colon splenic flexure is most common
2nd most common site is terminal ileum
It has to be suspected after non operative management
of NEC in infants with failure to thrive , rectal bleeding or
bowel obstruction.
31
32. cont…..complications
• Intestinal malabsorption and short bowel
syndrome
Short bowel syndrome is seen in infant who
undergo surgical intervention(23%).
• Cholestatic liver disease
Seen in those on TPN for prolonged period of time
32
33. Cont….complications GI
• Recurrent NEC
Cause is not known incidence is 4-6%
Cardiac patients are resistant to recurrence 0.6%
Sarah S. Pickard, Jeffrey A. Feinstein, Rita A. Popat, Lyen Huang and Sanjeev Dutta
Pediatrics May 2009, 123 (5) e901-e906; DOI: https://doi.org/10.1542/peds.2008-3216
33
34. Cont …..GI complications
• Anastomotic ulceration
This complication seen several years after
surgery(Resection and anastomosis done in
neonatal period) they present with lower GI
bleeding symptoms like hematochezia .
Diagnosed with colonoscopy treated with
revision of anastomosis and resection of
ulcer
34
35. Neurodevelopmental :
The incidence of NDI in NEC survivors is 40%.
NEC survivors are more likely than age-matched
controls to develop cerebral palsy, blindness,
and hearing impairment.
Babies with severe NEC that require surgery
have poorer neurological outcomes than
those with milder NEC that can be treated
Conservatively.
Matei A, Montalva L, Goodbaum A, et alNeurodevelopmental impairment in necrotising enterocolitis survivors:
systematic review and meta-analysisArchives of Disease in Childhood - Fetal and Neonatal Edition Published
Online First: 04 December 2019. doi: 10.1136/archdischild-2019-317830
35
36. What can be done?
Developmental screening has to be performed
every 4monthly for fies year and evry 6months
during second year of life.
36
37. Prevention
Augmentation of host defense
1. Oral immunoglobulin preparation
Enteral administration of IgG & IgA decereases the
incidence of NEC
It acts by preventing bacterial translocation by enhancing
gut mucosal barrier
Wolf, H. and Eibl, M. (1994), The anti‐inflammatory effect of an oral immunoglobulin (IgA‐IgG) preparation
and its possible relevance for the prevention of necrotizing enterocolitis. Acta Pædiatrica, 83: 37-40.
https://doi.org/10.1111/j.1651-2227.1994.tb13240.x
37
38. 2.Maternal glucocorticoids administration
There is significant reduction in incidenc of NEC in baby
born to mothers receiving antenatal glucocorticoids for
fetal plumonary maturation 2% from 7% (Controls)
Because of accelerated intestinal maturity
Charles R. Bauer, John C. Morrison, W. Kenneth Poole, Sheldon B. Korones, John J.
Boehm, Henrique Rigatto and Richard D. Zachman
Pediatrics May 1984, 73 (5) 682-688;https://pediatrics.aappublications.org/content/73/5/682/tab-article-info
38
39. Cont …..prevention
3.Breast milk:
Breast milk has array of humoral & cellular anti
infectious factors, growth factor, probiotics, vitamins ,
IgA, macrophages , lymphocytes, lactoferrin, lysozyme,
probiotics Bifidobacterium infantis and lactobacillus
acidophilus, PAF acetylhydrolase.
Breast milk inhibits growth of E Coli by providing acidic
environment
39
40. Cont…...prevention
Incidence of NEC in formula fed infant is 4-6 times than
with breast fed infants.
For every 100 ml /kg increase in human milk intake with
the 14 days of diagnosis there is decreased risk of NEC or
death
Alan H. JobeNEC and human milk
The Journal of Pediatrics, Volume 156, Issue 4, April 2010, Pages A2
https://doi.org/10.1016/j.jpeds.2009.10.040
41. Methods to decrease intestinal bacterial
colonization
1. Probiotics
They are live microbial supplements that colonize the
intestine to provide benefit to the host.
Commonly used are
• Lactobacillus bifidobacterium
• Streptococcus salivarius
• Saccharomyces boulardii
30% reduction in incidence of NEC
41
42. 2.Prebiotics
Administration non digestible dietary supplements as
long chain carbohydrate or mucin that promotes
proliferation of beneficial commensal bacteria.
3.Postbiotic
These are bacterial metabolites like butyric acid and
short chain fatty acids produced by commensal
organisms by catabolism of complex carbohydrates it is
major energy source for colonic enterocytes , its
suppresses the inflammation and apoptosis.
42
43. Methods to decrease inflammatory cascade
1. Inflammatory mediator antagonists
PAF acetylhydrolase
1. Arginine
Substrate for NO production
It is known decrease incidence of NEC
1. Epidermal growth factor
Helps in healing of dammaged mucosa by inducing
mucosal enzyme, trefoil peptide expression and
inbibiting effects on gastric acid secretion
43
44. References
Gosfeld and
5. Neonatal necrotizing enterocolitis an epidemiological study.
Narang A, Rao R, Bhakoo ON
Indian Pediatr. 1993 Oct; 30(10):1207-14.http://www.indianpediatrics.net/oct1993/1207.pdf
6. https://www.ncbi.nlm.nih.gov/pubmed/21247316#
13. NEUHAUSER EB, WITTENBORG MH. Pediatric radiology. N Engl J Med. 1953;249(2):62–8.
https://doi.org/10.1007/bf02396612
17. . Thuijls G, Derikx JPM, Wijck K Van, Zimmermann LJI. Non-Invasive Markers for Early Diagnosis and
Determination of the Severity of Necrotizing Enterocolitis. 2010;
https://doi.org/10.1097/SLA.0b013e3181d778c4
18. https://doi.org/10.1016/j.jpedsurg.2018.02.083
1. Goldstein SD, Beaulieu RJ, Niño DF, Chun Y, Banerjee A,
Sodhi CP, et al. Early detection of necrotizing enterocolitis using broadband
optical spectroscopy. J Pediatr Surg
24. Coursey CA, Hollingsworth CL, Wriston C, Beam C, Rice H, Bisset G. Radiographic predictors of
disease severity in neonates and infants with necrotizing enterocolitis. Am J Roentgenol.
2009;193(5):1408–13. 10.2214/AJR.08.2306 44
45. 6. Abboud B, El Hachem J, Yazbeck T, Doumit C. Hepatic portal venous gas: Physiopathology, etiology, prognosis
and treatment. Vol. 15, World Journal of Gastroenterology. 2009. p. 3585–90.
https://doi.org/10.3748/wjg.15.3585
27. Trial NET, Rees CM, Eaton S, Khoo AK, Kiely EM. Peritoneal drainage does not stabilize extremely
low birth weight infants with perforated bowel : data from the. J Pediatr Surg [Internet]. 2010;45(2):324–
9. Available from: http://dx.doi.org/10.1016/j.jpedsurg.2009.10.066
29. Hull MA, Fisher JG, Gutierrez IM, Jones BA, Kang KH, Kenny M, et al. Mortality and Management of Surgical
Necrotizing Enterocolitis in Very Low Birth Weight Neonates : A Prospective Cohort Study. J Am Coll Surg
[Internet]. 2013; Available from: http://dx.doi.org/10.1016/j.jamcollsurg.2013.11.015
30. Hull MA, Fisher JG, Gutierrez IM, Jones BA, Kang KH, Kenny M, et al. Mortality and Management of Surgical
Necrotizing Enterocolitis in Very Low Birth Weight Neonates : A Prospective Cohort Study. J Am Coll Surg
[Internet]. 2013; Available from: http://dx.doi.org/10.1016/j.jamcollsurg.2013.11.015
33.Sarah S. Pickard,
Jeffrey A. Feinstein, Rita A. Popat, Lyen Huang and Sanjeev Dutta
Pediatrics May 2009,
123 (5) e901-e906; DOI: https://doi.org/10.1542/peds.2008-3216
45
46. 35. Matei A, Montalva L, Goodbaum A, et alNeurodevelopmental
impairment in necrotising enterocolitis survivors: systematic review and
meta-analysisArchives of Disease
in Childhood - Fetal and Neonatal Edition Published Online First: 04 December 2019. doi:
10.1136/archdischild-2019-317830
37.Wolf, H. and Eibl, M. (1994), The anti‐inflammatory effect of an oral immunoglobulin (IgA‐IgG)
preparation and its possible relevance for the prevention of necrotizing enterocolitis. Acta Pædiatrica,
83: 37-40. https://doi.org/10.1111/j.1651-2227.1994.tb13240.x
38. Charles R. Bauer, John C. Morrison, W. Kenneth Poole, Sheldon B. Korones, John J. Boehm,
Henrique Rigatto and Richard D. Zachman
Pediatrics May 1984,
73 (5) 682-688;https://pediatrics.aappublications.org/content/73/5/682/tab-article-info
40. Alan H. JobeNEC and human milk
The
Journal of Pediatrics, Volume 156, Issue 4, April 2010, Pages A2
https://doi.org/10.1016/j.jpeds.2009.10.040
46