1. A Bi-monthly publication from The Gardner Group August 2012
Reflections on Higher Limits for HSA
Supreme Court Contributions
Decision The US Internal Revenue Service announced
the 2013 limits on contribution and out-of-
Late in June, the Supreme pocket spending amounts for health savings
Court of the United States accounts (HSAs) and for the high-deductible
(SCOTUS) upheld the health plans (HDHPs) to which HSAs must be
Affordable Care Act (ACA), linked.
President Obama’s
signature health care The higher rates reflect the cost-of-living
reform law. As with adjustment and rounding rules of Internal
SCOTUS opinions, the devil Revenue Code section 223.
is in the details.
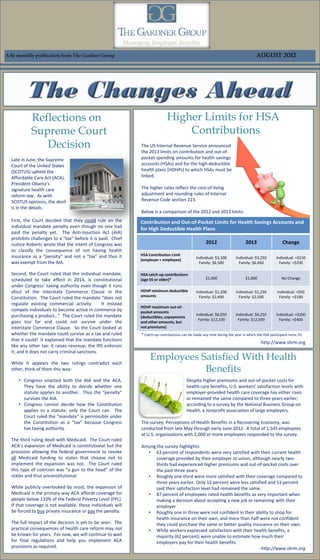
Below is a comparison of the 2012 and 2013 limits:
First, the Court decided that they could rule on the Contribution and Out-of-Pocket Limits for Health Savings Accounts and
individual mandate penalty even though no one had
for High Deductible Health Plans
paid the penalty yet. The Anti-Injuction Act (AIA)
prohibits challenges to a “tax” before it is paid. Chief
Justice Roberts wrote that the intent of Congress was 2012 2013 Change
to classify the consequence of not having health
insurance as a “penalty” and not a “tax” and thus it HSA Contribution Limit
Individual: $3,100 Individual: $3,250 Individual: +$150
(employer + employee)
was exempt from the AIA. Family: $6,500 Family: $6,450 Family: +$200
Second, the Court ruled that the individual mandate, HSA catch-up contributions
scheduled to take effect in 2014, is constitutional (age 55 or older)* $1,000 $1,000 No Change
under Congress’ taxing authority even though it runs
afoul of the Interstate Commerce Clause in the HDHP minimum deductible Individual: $1,200 Individual: $1,250 Individual: +$50
amounts Family: $2,400 Family: $2,500 Family: +$100
Constitution. The Court ruled the mandate “does not
regulate existing commercial activity. It instead
HDHP maximum out-of-
compels individuals to become active in commerce by pocket amounts
purchasing a product…” The Court ruled the mandate Individual: $6,050 Individual: $6,250 Individual: +$200
(deductibles, copayments
Family: $12,100 Family: $12,500 Family: +$400
goes too far and could not survive under the and other amounts, but
Interstate Commerce Clause. So the Court looked at not premiums)
whether the mandate could survive as a tax and ruled * Catch-up contributions can be made any time during the year in which the HSA participant turns 55.
that it could! It explained that the mandate functions
-http://www.shrm.org
like any other tax: it raises revenue; the IRS enforces
it; and it does not carry criminal sanctions.
While it appears the two rulings contradict each
Employees Satisfied With Health
other, think of them this way: Benefits
• Congress enacted both the AIA and the ACA. Despite higher premiums and out-of-pocket costs for
They have the ability to decide whether one health care benefits, U.S. workers’ satisfaction levels with
statute applies to another. Thus the “penalty” employer-provided health care coverage has either risen
survives the AIA. or remained the same compared to three years earlier,
• Congress cannot decide how the Constitution according to a survey by the National Business Group on
applies to a statute, only the Court can. The Health, a nonprofit association of large employers.
Court ruled the “mandate” is permissible under
the Constitution as a “tax” because Congress The survey, Perceptions of Health Benefits in a Recovering Economy, was
has taxing authority. conducted from late May through early June 2012. A total of 1,545 employees
at U.S. organizations with 2,000 or more employees responded to the survey.
The third ruling dealt with Medicaid. The Court ruled
ACA’s expansion of Medicaid is constitutional but the Among the survey highlights:
provision allowing the federal government to revoke • 63 percent of respondents were very satisfied with their current health
all Medicaid funding to states that choose not to coverage provided by their employer or union, although nearly two-
implement the expansion was not. The Court ruled thirds had experienced higher premiums and out-of-pocket costs over
this type of coercion was “a gun to the head” of the the past three years.
states and thus unconstitutional. • Roughly one-third were more satisfied with their coverage compared to
three years earlier. Only 12 percent were less satisfied and 53 percent
While publicly overlooked by most, the expansion of said their satisfaction level had remained the same.
Medicaid is the primary way ACA affords coverage for • 87 percent of employees rated health benefits as very important when
people below 133% of the Federal Poverty Level (FPL). making a decision about accepting a new job or remaining with their
If that coverage is not available, those individuals will employer
be forced to buy private insurance or pay the penalty. • Roughly one in three were not confident in their ability to shop for
health insurance on their own, and more than half were not confident
The full impact of the decision is yet to be seen. The they could purchase the same or better quality insurance on their own.
practical consequences of health care reform may not • While workers expressed satisfaction with their health benefits, a
be known for years. For now, we will continue to wait majority (62 percent) were unable to estimate how much their
for final regulations and help you implement ACA employers pay for their health benefits.
provisions as required. -http://www.shrm.org
2. August 2012
Let Us Take Your Group to the Ball Game!
Enter to win 20 Jacksonville Suns tickets for any remaining home games by simply “Liking” us on
Facebook or “Following” us on LinkedIn between August 1st and August 8th. Follow the links below
to get to our Facebook and LinkedIn Pages. The winner will be announced on August 9th. Good Luck!
www.facebook.com/managingemployeebenefits
www.linkedin.com/company/the-gardner-group---managing-employee-benefits
Outcomes-Based Medical Loss Ratio Rebates
Wellness Incentives The Patient Protection and Affordable Care Act of 2010 includes many
provisions that are continuously being uncovered and defined. One such
provision, the Medical Loss Ratio (MLR) provision, requires health insurers who
A coalition of health care
spend more than a specified percentage of premium dollars on categories of
organizations has produced
spending other than “clinical services and activities designed to improve the
new guidance for the use of
quality of healthcare” (claim payments and medical management costs) to
outcomes-based incentives
rebate a portion of the premium dollars collected to enrollees. The minimum
in employer-sponsored
medical loss ratio is 80% for the small group market and 85% for the large
wellness programs.
group market. This requirement first applied to health insurers for calendar
Outcomes-based incentives year 2011 and, to the extent rebates are required, they will be paid before
provide employees with a August 1, 2012.
financial reward for meeting a specific health target—or a
penalty may be imposed for failure to meet a health The MLR is not calculated at the individual plan or employee level, but based
standard—rather than simply providing an incentive to on the collective experience of all plans in a certain, legally-defined grouping.
participate in the program. Outcomes-based incentives are Employer plans are grouped together based generally on the legal entity that
expected to become more common in the workplace as a issued the coverage (insurance company or HMO), the state where the policy is
result of provisions in the Patient Protection and Affordable issued and the appropriate market segment (large group, small group,
Care Act that encourage their use. individual insurance). It is possible that an employer can have more than one
plan within these groupings.
The new guidance includes the following 10 suggestions for
employers using outcome-based incentives: So, what are employers required to do when they receive the rebate
1. Consider using the four biometric target categories of check?
weight, cholesterol, blood pressure and tobacco use.
First, employers must determine who paid the premiums for the health
2. Factor in potential financial and time burdens for insurance policy. If employees made premium contributions, the employer
employees when determining the specific standard you must determine what portion of the rebate is attributable to participant
are asking them to meet. contributions. The portion of the rebate attributable to participant
3. Consider whether the incentive design is likely to place contributions is usually based on the share or percentage of premiums paid by
a greater economic burden on one race, ethnic group employees.
or other category of employees.
Second, the employer must decide how to use the participant’s share of the
4. Consider incentive designs that are reasonable goals
rebate. There are basically three (3) ways outlined by the Department of
(preferably individualized to the employee) rather than
Labor:
ideal targets applied rigidly to all employees.
5. Offer (as required by law) a reasonable alternative • The rebate can be paid to the participants
standard to employees for whom it would be under a fair and equitable allocation method.
unreasonably difficult to achieve a health standard due For example, an employee with family coverage,
to a medical condition, or who have a medical reason who paid a larger share of premiums, would
that makes it inadvisable for them to do so within the get a larger share of the rebate. The employer
allotted time. can also conclude that only current
participants are allowed to share in the
6. For employees with a medical condition that makes it
rebate. Each employee that
unreasonably difficult to achieve the health standard,
receives a share of the
or medically inadvisable to do so, consider deferring to
rebate will recognize
the views of the employee’s health care provider for
additional taxable
setting and achieving a reasonable alternative standard
income.
or providing a waiver.
7. Consider providing all employees with options for • The employer can apply the entire rebate toward future participant
attaining the incentive, rather than only offering an premium payments (i.e. give a “premium holiday”).
alternative standard to those with a medical
circumstance. • The employer could use the rebate to provide enhanced benefits for
participants.
8. Avoid using a reward or penalty that is so large it
discourages health plan enrollment, denies coverage, The DOL suggests that the second and third options should be used only if
or creates too heavy a financial penalty on individuals distributing payments to employees is not cost effective – for example, if the
who do not satisfy an initial wellness standard. payments are de minimis or if they would give rise to tax consequences to the
9. Consider an incentive design that rewards for progress employee. To avoid having to establish a trust to hold the rebate, the
toward the standard targets, instead of just rewarding employer should distribute the premium credit or enact the benefit
employees who meet the goal. enhancement within three months after receipt of the rebate.
10. Consider strategies that help employees integrate The Minimum Loss Ratio (MLR) mandate contained in PPACA has created a
healthy behaviors into their personal value framework myriad of compliance requirements for health insurers, health plans and
by promoting individual choice, so they are more likely employers. Until the Individual Mandate becomes effective in 2014, the
to sustain healthy behavior changes over time. calculation and distribution of rebate checks is potentially the most costly of
Click here for access to the full article. the PPACA requirements to date. The Gardner Group recognizes the challenges
faced in complying with PPACA and is monitoring legislation, interim rules and
- By Stephen Miller, CEBS operational best practices to provide direction through these legislative
- www.shrm.org nuances.