Improving Healthcare Through Digital Transformation
Implementing Telestroke Technology in Rural Hospitals
1. Implementing Telestroke Technology
in Rural Hospitals
Eli King, Tyler Mock, Tania Tando, Ogomah Egembah
Gordon Ford College of Business, Western Kentucky University, Bowling Green, KY
Abstract
We explored the possibility of implementing
telemedicine in the Medical Centers of
Scottsville and Franklin to improve stroke
outcomes. Telestroke, a category of
telemedicine, allows a remote neurologist to
advise hospital staff during stroke care via
video streaming. Through interviews with
experts and telemedicine companies we
determined Neurocall, an on-demand stroke
service, was the optimal choice. We also
determined the most efficient technology
to accompany this service that was intuitive to
use and reliable. By introducing telestroke,
CHC can lower the financial burden of having a
stroke for its rural residents and also increase
revenue; but more importantly patients
receiving CHC’s modernized stroke care will
enjoy more favorable health outcomes.
Acknowledgements
We would like to thank Dr. Bob Hatfield for aligning our group with CHC. We
thank Eric Hagan, Sally Tanaro and their team for allowing us to work on this
project.
Methods
We analyzed the stroke incidence rates and outcomes in these
rural areas by collecting hospital emergency room data as well as
mining the most recent census data available. To outline the
current demand we used regression to update these values to
2015. By interviewing subject matter experts and corresponding
with telehealth services we were able to research telestroke
services that matched the hospitals’ needs.
Introduction
Every year in the United States more than
600,000 ischemic stroke patients do not
receive tissue plasminogen activator (tPA),
the one medication endorsed by the U.S. Food
and Drug Administration for acute ischemic
stroke. Administering intravenous tPA soon
after the onset of an ischemic stroke is a cost-
effective treatment that can reduce mortality
and disability, FDA limits the use of IV tPA to
3 hours from the onset of stroke symptoms.
The lack of treatment is due partly to
shortages of neurological experts in rural and
underserved areas and the danger of
administering the drug to non-ischemic stroke
patients who will be negatively affected.
Telestroke programs can improve stroke care
for patients in rural and underserved settings
by using interactive telecommunication
technology that connects hospitals without
stroke expertise with neurologists who advise
the diagnosis and treatment of stroke patients.
Kentucky has enacted policies that facilitate
telestroke access and ensures repayment by
insurance companies for telestroke services.
Results
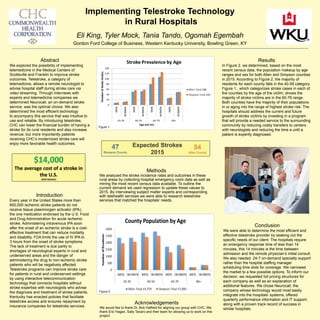
In Figure 2. we determined, based on the most
recent census data, the population makeup by age
ranges and sex for both Allen and Simpson counties
in 2015. According to Figure 2, the majority of
residents for each county falls in the 40-59 category.
Figure 1., which categorizes stroke cases in each of
the counties by the age of the victim, shows the
majority of stroke victims are in the 60-79 range.
Both counties have the majority of their populations
in or aging into the range of highest stroke risk. The
hospitals should address the current and future
growth of stroke victims by investing in a program
that will provide a needed service to the surrounding
community by reducing costly transfers to centers
with neurologists and reducing the time a until a
patient is expertly diagnosed.
Figure 1.
Conclusion
We were able to determine the most efficient and
effective telestroke provider by seeking out the
specific needs of our client. The hospitals require
an emergency response time of less than 14
minutes, this 14 minutes is the time between
admission and the remote physician’s initial consult.
We also needed 24-7 on-demand specialty support
rather than the hospital staffing manager
scheduling time slots for coverage. We narrowed
the market to a few possible options. To inform our
decision, we requested full pricing structures for
each company as well as an explanation of
additional features. We chose Neurocall, the
company whose technology would most easily
integrate into the hospitals’ systems, offered
quarterly performance information and IT support;
along with a proven track record of success in
similar hospitals.
Figure 2.