Oval Window - neurotology meeting tel aviv dec 2014- 021114
1. Oval Window Obliteration: How, Why and What to Do ?
Tal Marom, MD, Abraham Goldfarb, MD, Yahav Oron, MD, Sharon Ovnat Tamir, MD
Edith Wolfson Medical Center, Tel-Aviv University, Sackler School of Medicine, Israel
ABSTRACT
Congenital absent oval window is an uncommon condition
that results in significant hearing loss in the pediatric
population. The cause remains unknown, but there are
several theories pertaining to explain. Treatment outcomes
and results following surgery are still not well established,
due to the limited number of cases that have been published
in the literature.
This is a review of the causes, the theories and treatment of
oval window obliteration.
INTRODUCTION
Congenital absent oval window (CAOW) is a rare condition.
Despite its first description as early as 1958 (1), there has
been limited literature and progress in the understanding
and management.
It is theorized that the cause of CAOW involves failure of the
otic capsule bone to open into the vesitbule (the stapes
footplate fails to develop; alternatively, the primitive stapes
fails to fuse with the primitive vesitbule) (2) .CAOW results
from hypo-development of the second branchial arch. CAOW
manifests with significant congenital conductive hearing loss
of up to 60 dB.
CASE PRESENTATION
A 15 year-old male presented with a maximal right ear
conductive hearing loss. The patient had a history of
recurrent ventilating tube insertions during childhood, with a
residual tympanic membrane perforation that underwent
myringoplasty at the age of 13.
During myringoplasty, the surgeon suspected
tympanosclerosis and further investigation was warranted in
order to make a surgical decision. High resolution temporal
bone CT scan showed calcification of the right oval window,
aberrant facial nerve course, and no other ossicular
malformations were identified. The patient deferred any
treatment except surgery. Hence, he underwent middle ear
exploration. The surgical findings were: CAOW with no
anatomical landmarks, a malformed stapes with only one
crus and no footplate. It was not possible to assess the
position of the facial nerve. The incudo-stapedial joint was
malformed with no capitulum. After discussion with the
parents, abortion of the procedure was decided. Following
recovery, the option of BAHA was discussed with the
patient.
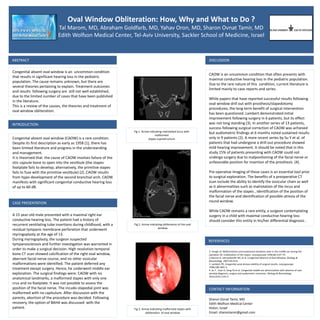
Fig 1. Arrow indicating malrotated incus with
malformed
stapes suprastructure
Fig 2. Arrow indicating obliteration of the oval
window
Fig 3. Arrow indicating malformed stapes with
obliteration of oval window
DISCUSSION
CAOW is an uncommon condition that often presents with
maximal conductive hearing loss in the pediatric population.
Due to the rare nature of this condition, current literature is
limited mainly to case reports and series.
While papers that have reported successful results following
oval window drill out with prosthesis/stapedotomy
procedures, the long term benefit of surgical intervention
has been questioned. Lambert demonstrated initial
improvement following surgery in 6 patients, but its effect
was not long standing (3). In another series of 13 patients,
success following surgical correction of CAOW was achieved
but audiometric findings at 6 months noted sustained results
only in 9 patients (2). A more recent series by Su Y et al. of
patients that had undergone a drill-out procedure showed
mild hearing improvement. It should be noted that in this
study 15% of patients presenting with CAOW could not
undergo surgery due to malpositioning of the facial nerve or
unfavorable position for insertion of the prosthesis (4).
Pre-operative imaging of these cases is an essential tool prior
to surgical exploration. The benefits of a preoperative CT
scan include the ability to identify the ossicular chain as well
as it abnormalities such as malrotation of the incus and
malformation of the stapes , identification of the position of
the facial nerve and identification of possible atresia of the
round window.
While CAOW remains a rare entity, a surgeon contemplating
surgery in a child with maximal conductive hearing loss
should consider this entity in his/her differential diagnosis .
Sharon Ovnat Tamir, MD
Edith Wolfson Medical Center
Holon, Israel
Email: sharontamir@gmail.com
CONTACT INFORMATION
REFERENCES
1. Hough JV. Malformations and anatomical variations seen in the middle ear during the
operation for mobilization of the stapes. Laryngoscope 1958;68:1337-79.
2.Alarcon A, Jahrsodoerfer RA, et al. Congenital Absence of Oval Window. Otology &
Neurotology 2007;29:23-8.
3. Lambert PR. Congenital aural atresia stability of surgical results. Laryngoscope
1998;108:1801-5.
4. Su Y , Yuan H, Song YS et al. Congenital middle ear abnormalities with absence of oval
window:diagnosis, surgery and audiometric outcomes. Otology & Neurotology
2014;35(7):1191-5