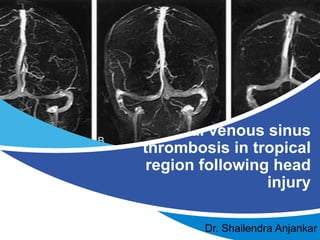
Dural venous sinus thrombosis in tropical region following head injury.
•Download as PPTX, PDF•
1 like•77 views

- The document discusses 5 cases of dural venous sinus thrombosis (DVST) following traumatic brain injury in a tropical region of central India. - All 5 patients presented with intracranial bleeding shown on CT scans but had no signs of external head injury. They were found to be dehydrated. - DVST was diagnosed using MRI and MR venography. The patients were treated with low molecular weight heparin and showed improvement without requiring surgery. - The author hypothesizes that dehydration may be an aggravating factor for DVST following traumatic brain injury in hot, dry climates like central India. High clinical suspicion is needed for prompt diagnosis.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Dural venous sinus thrombosis in tropical region following head injury.
Similar to Dural venous sinus thrombosis in tropical region following head injury. (20)
Recently uploaded
Recently uploaded (20)
Dural venous sinus thrombosis in tropical region following head injury.
- 1. Dural venous sinus thrombosis in tropical region following head injury Dr. Shailendra Anjankar
- 2. Dural venous sinus thrombosis in tropical region following head injury. Dr. Shailendra Anjankar Consultant Neurosurgeon, SD, SevenStar & Orange City Hospital Nagpur. Ex –Assistant Professor, JNMC, Sawangi (M), Wardha 2 TITLE
- 3. • Dural Venous Sinus Thrombosis (DVST) is rarely reported as a sequel following traumatic brain injury (TBI). • It usually follows hypercoagulable states such as pregnancy, following skull fracture, and severe dehydration etc. INTRODUCTION Reference: Ciliz D et al. Turkish Neurosurgery. 2008;18:70-7. Bhatoe HS et al. Neurol India 2015;63:832-3
- 4. 4 • Central India has a tropical semi- arid climate where the rate of evaporation of water is higher than the rate of moisture received through precipitation. • The temperature of Vidarbha region ranges from a minimum of 12- 25°C to a maximum of 30- 48°C, with relative humidity varying from 10-15% to 60-95% Reference: Tiple AD,et al . Odonatologica. 2013;42:237-45.
- 5. 5
- 6. 6 • In emergency room, when CT Brain shows bleed, it is difficult to differentiate that has the intracranial bleed caused trauma; or trauma caused bleed. Trauma IC Bleed
- 7. • 61-year male, known case of seizure disorder, no other co-morbidities, presented with alleged H/o RTA. • He had 1 episode of seizures and was brought to hospital in post ictal state. • He had no external injury. CASE SERIES – CASE 1
- 8. CASE 2,3,4,5 • All the 5 patients had no external injury on head and on CT showed bleed and MRI Brain with MRV showed DVST. • All of them had signs of dehydration like dry tongue and decreased skin turgor with increased blood urea to creatinine ratio. • No obvious external head
- 9. 9 • In our small case series of 5 patients, were treated with Low molecular weight Heparin for 3 to 5 days and on repeat imaging we could not find any fresh bleed whereas there was resolution of bleed and cerebral oedema with symptomatic improvement in headache. • Fortunately, none of them required surgery, but strict monitoring of patient’s condition, repeat imaging plan, and surgery plan was always kept at stand by.
- 10. • DVST if diagnosed early and managed promptly may improve prognosis. Various imaging modalities can help in early diagnosis if there is clinical suspicion. • Treatment includes maintaining good hydration, anti-edema medications & anticonvulsants. • Anticoagulation therapy is the first choice in such cases although it remains controversial in traumatic brain injury, in view increase risk of bleeding. DISCUSSION Reference: Kumar GS, et al. Neurology India. 2004;52:123-4. Stam J: et al Adv Neurol 92: 233-240, 2003
- 11. 11 • Various hypothesises are given for DVST. • Carrie and Jaffe stated that abnormalities in the clotting mechanism, disturbances in blood flow or damage to the capillary endothelium may predispose and lead to thrombosis. Pre-existing coagulopathy may be a factor in predisposing patients. • Case series by Delgado Almandoz JE et al showed strong co-relation between skull fracture and DVST, whereas in our series we could not find any.Reference: Carrie AW, Jaffe FA. J Neurosurg 1954;11:173-82. Delgado Almandoz JE, et al Radiology. 2010;255:570-7.
- 12. 12 • Dehydration is strongly and independently associated with venous thromboembolism in all age group and types of patients. • In this small case series, we found discrepancy in external injury and internal bleed size in all patients. DVST needs a high index for suspicion for prompt diagnosis, and this discrepancy could be one of the clue for the diagnosis. Reference: Kelly J, et al. Qjm. 2004;97:293-6.
- 13. • We included only those patients who had no external injury, • Small case series, • Not investigated for Factor V Leiden, deficiency of antithrombin, protein C and protein S, elevated homocysteine. LIMITATION
- 14. • In tropical region, where the climate is hot and dry dehydration may be the aggravating factor for DVST following TBI. • DVST needs a high index for suspicion for prompt diagnosis. • The discrepancy in external injury and internal bleed size can serve as one of the clue for clinical suspicion. CONCLUSION
- 15. ACKNOWLEDGEMENT
- 16. 16
Editor's Notes
- © Copyright PresentationGo.com – The free PowerPoint template library
- © Copyright PresentationGo.com – The free PowerPoint template library
- © Copyright PresentationGo.com – The free PowerPoint template library
- © Copyright PresentationGo.com – The free PowerPoint template library
- © Copyright PresentationGo.com – The free PowerPoint template library
- © Copyright PresentationGo.com – The free PowerPoint template library
- © Copyright PresentationGo.com – The free PowerPoint template library
- © Copyright PresentationGo.com – The free PowerPoint template library
- © Copyright PresentationGo.com – The free PowerPoint template library