3. Regulation of arterial pressure (АP)
Formula: АP = CO · PR
CO – cardiac output
PR – peripheral resistance (depended to arterioles tone)
CO leads to PR and АP normalizes finally
PR leads to CO and АP normalizes finally
7. Depresors system
• Barroreceptors of aorta arch and
sinus caroticus
• PG A, E, I;
• Natriuretic peptide hormone
• Parasympathetic nervous system.
8. Regulative systems
1. Barroreceptors of aorta arch and sinus caroticus
Barroreceptors
of the vessels
Medulla oblongata
(vessel’s active center)
Afferent impulses
Heart (CO increase at
decreased АP)
Arterioles (spasm) Еfferent і impulses
9. Regulative systems
2. Renin–angiotensin system
АP
Activation of kidney
JGA (juxta glomerular
apparatus)
Excretion of the RENIN
(it is enzyme)
Conversation
angiotensin 1 into angiotensin 2
Conversation
angiotensinogen into
angiotensin 1
Angiotensin converting
enzyme (АCE)
10. Regulative systems
3. Renin–angiotensin-aldosteron system
Renin Actination of
suprarenal glangs
(cortical layer)
Na reabsorbtion
in kidney increase
Angiotensin 2
Aldosteron
excretion
Na concentration in
blood increase,
blood osmotic
pressure increase
Move of extravascular
fluid inside the
vessels
Increase of circulative
blood volume
(CBV)
CО increase
12. AP elevation
(value above 140/90 mm Hg), which
is resulted from rising of peripheral
vessels resistance
(one of the most common cardiovascular disorders)
Arterial hypertension (АH)
13. Classification of arterial hypertension
Category Systolic BP
(mm hg)
Diastolic BP
(mm hg)
Normal BP Below 130 Below 85
High-normal BP
(pre-hypertension)
130-139 85-89
Stage 1 (mild) hypertension 140-159 90-99
Stage 2 (moderate) hypertension 160-179 100-109
Stage 3 (severe) hypertension 180 or higher 110 or higher
15. Reason is unknown.
AH is polyetiological disease.
AH arises on the ground of genetically
peculiarities of metabolism.
That is possible to have genetically defect of the
systems, which control relaxation of the
smooth muscle cells of the arterioles.
Etiology (primary AH)
16. Contributing factors
Family history
Age-related changes in blood
pressure High salt intake
Stress
Hyperinsulinemia:
causes high activity sympathetic link of ANS and its
effect on cardiac output, peripheral vascular
resistance and renal sodium retention;
stimulates sodium and calcium transport across the
cell membrane of vascular smooth muscle,
thereby sensitizing blood vessels to vasopressor
stimuli
Obesity (because hyperinsulinemia)
Excess alcohol consumption
(mechanism in unclear)
17. Pathogenesis of primary (essential) hypertension
• Dysregulatory theory - violations of regulatory
mechanisms of arterial vessels tone.
There are two phases:
1. Hyperkinetic
1 stage: activation of the sympathetic and adrenal
system under the action of stress factors
2 stage: activation of the rennin-angiotensin-
aldosteron system
3 stage: activation of aldosteron and vasopressin
systems
18. Pathogenesis of primary (essential)
hypertension
2. Hypokinetic - is characterized by the irreversible
structural changes of compession and resistance
vessels, peripheral vascular resistance and arterial
vessels tone grows as a result constantly. The main
significance has following factors:
• constant spasm of arterioles;
• hypertrophy of smooth muscles;
• atherosclerosis and substitution of smooth
muscles by connective tissue.
19. Pathogenesis of primary (essential)
hypertension
• Membrane theory is the hereditarily conditioned
violation of ionic pumps of membranes of smooth
muscles fibers:
• defect of Ca2+- pump- this leads to the
development of permanent contraction and the
increase of peripheral vascular resistance.
• decrease work of Na -K –pump - the outcome is the
thickening of vessel’s wall and diminishing of
diameter of vessels increase of sensitization to the
action of catecholamine, damage and necrosis of
cells, atherosclerosis).
21. Renal
Renovascular
Reason of origin of renovascular AH is a reduced renal
blood flow :
a) compression of renal arteries by a tumor, scar;
b) narrowing of vessels by embolus, atherosclerotic
plaque;
c) hypovolemia ;
The decreased renal blood flow activates renin-
angiotensin-aldosterone mechanism.
22. 2. Renoprive
(arises after kidney remove)
Etiology
secondary АH
Reason of renoprive AH is a degradation of
structural components of kidneys which provide
hypotension effects, in particular:
1) angiotenzinazu, which destroys an angiotensin-II
2) Phospholipid inhibitir of renine;
3)Prostaglandin E
23. Depressive function of kidney – synthesis of the
substances for AP reduce
PG Е 2
Phospholipid Renin
Inhibitor
Angiotensinase
Phosphatydilcholin
alkali ethers
! ! !
Exhaustion of kidney
depressive function
leads to arterial
hypertension
stabilization
dilates renal arteries, reduces renin
synthesis and reduces Na
reabsorbing in kidney
24. Endocrine
(develops in the result of endocrine glands pathology)
Etiology
secondary АH
Cushing's disease
(Adrenocorticotropin over production
by the pituitary gland anterior part)
Pheochromocytoma
(increase production of
catecholamines epinephrine and
norephinephrine )
Hyperaldosteronism –tumor of
glomerular zone of adrenal
Menopause
(age-depended decrease of female
gonads activity – estrogens
excretion decrease)
Possible mechanism – deficit of NO
synthesis by endotheliocytes
25. Neurogenic
(is accompanying to nerves system pathology)
Etiology
secondary АH
Brain hemorrhage
Encephalitis
Brain tumor
Brain trauma
Brain ischemia
30. 2. Cardiac output increase
SAS activation
Adrenalin excretion
Increase of cardiac
contractility force
Increase of cardiac
output
Increase of heart beats
AP elevation
Pathogenesis
Formula: АP = CO · PR
31. 3. SAS activation
Interaction adrenalin and
alpha-adrenoreceptors
Arterioles smooth
muscles spasm
Suprarenal glands
activation
Venues smooth
muscles spasm
Increase of circulative
blood in big blood
circle
adrenoreceptors of
heart
Аdrenalin
Noradrenalin
Increase of CBV
CO increase
Arterioles
narrowing
alpha-adrenoreceptors
of vessels
CO increase
AP increase
SAS activation
Arterioles narrowing
PR increase
Pathogenesis
Formula: АP = CO · PR
32. 4. Kidney functions violation
Long time spasm of
kidney’s arteries
AP increase
AP decrease in renal
capillaries
Activation of JGA
Renin excretion
Angiotensin 2
synthesis
Angiotensin 2 effects
• Smooth muscles contraction in the
vessels
• Stimulation of the vasoactive center
in brain
• Noradrenalin excretion increase
• Adrenalin excretion increase from
suprarenal glands
• Aldosteron excretion increase from
suprarenal glands (Na retention due
to kidney)
Pathogenesis
33. 1st period
functional violations
(heart hypertrophy)
2d period
Pathological changes in arteries and arterioles (dystrophy):
- Arterioles sclerosis
- Arteriole’s wall infiltration by plasma (leads to dystrophy)
- Arterioles necrosis (hypertonic crisis arises in clinic)
- Vein’s wall thickening
Arterial hypertension after-effects
34. 3d period
Secondary changes in organs and systems
Kidney
(nephrosclerosis and chronic
kidney insufficiency)
CNS
– brain hypoxia
– neurons destruction
– apoplexy (because vessels destruction and rupture
leads to brain hemorrhages and brain
destruction)
Heart
Decompensate heart failure
Organs of vision
- retinopathy (retina’s vessels injury)
- hemorrhages and separation (exfoliation) of
retina, that leads to blindness
Endocrine system
Glands atrophy and sclerosis
Arterial hypertension after-effects
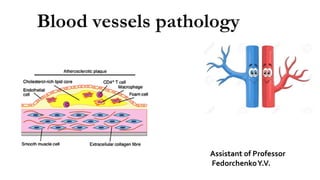
45. Pathology and pathogenesis
The lesions associated with atherosclerosis are of
three types:
The fatty streak
The fibrous atheromatous plaque
Complicated lesion
The latter two are responsible for the clinically
significant manifestations of the disease.
46.
47.
48. Fatty streaks are thin, flat yellow intimal discolorations that
progressively enlarge by becoming thicker and slightly elevated as
they grow in length.
They consist of macrophages and smooth muscle cells that have
become distended with lipid to form foam cells.
They increase in number until about age 20 years, and then they
remain static or regress.
50. Atheromatous plaques are the basic
lesions within the intima, having a core of
lipid (cholesterol and cholesterol esters)
and covering fibrous cap.
APs are also called fibrous, fibrofatty, lipid,
or fibrolipid plaques which have white to
whitish yellow colour and rise intima
slightly into the lumen of the artery.
The centers of larger plaques may contain
a yellow debris, hence the term atheroma.
51. Atheromatous plaques have 3 principal
components:
1) cells, including smooth muscle calls,
macrophages, and other leukocytes,
2) connective tissue extracellular matrix,
including collagen, elastic fibers, and
proteoglycans,
3) intracellular and extracellular lipid
deposits.
In advanced atherosclerosis, the fatty
atheroma may be converted to a fibrous scar.
52.
53. As the lesions increase in size, they encroach on the
lumen of the artery and eventually may occlude the
vessel or predispose to thrombus formation, causing a
reduction of blood flow.
54. The more advanced complicated lesions are characterized by
Hemorrhage
Ulceration
Scar tissue deposits
Thrombosis is the most important complication of
atherosclerosis.
It is caused by slowing and turbulence of blood flow in the region
of the plaque and ulceration of the plaque.
63. Clinical Manifestations
The clinical manifestations of atherosclerosis depend on the
vessels involved and the extent of vessel obstruction.
Atherosclerotic lesions produce their effects through:
narrowing of the vessel and production of ischemia;
sudden vessel obstruction caused by plaque hemorrhage
or rupture;
thrombosis and formation of emboli resulting from
damage to the vessel endothelium;
In larger vessels such as the aorta, the important
complications are those of thrombus formation and
weakening of the vessel wall.
In medium-size arteries such as the coronary and cerebral
arteries, ischemia and infarction caused by vessel occlusion
are more common.
Although atherosclerosis can affect any organ or tissue, the
arteries supplying the heart, brain, kidneys, lower extremities,
and small intestine are most frequently involved.
64. Atherosclerosis symptoms
If the narrowing of an artery is less than 70% - asymptomatic
Symptoms occur due to the location of the narrowing
Coronary arteries – angina pectoris, heart attack
Carotid arteries - brain stroke.
Arteries in the legs - leg cramps (intermittent claudication).
Renal arteries - kidney failure or high blood pressure (malignant
hypertension).
65.
66. Prevention and Treatment
Prevention – to modify risk factors
smoking,
high blood cholesterol levels,
high blood pressure,
obesity,
physical inactivity.
When atherosclerosis becomes severe the complications
themselves must be treated.