The management of pediatric polytrauma -a simple review
Guerrero, Sara_Medical Assistance in Emergencies_Logistical Challenges
1. Medical Assistance in Emergencies:
Logistical Challenges
A thesis submitted in partial fulfillment of the requirements for
the degree of M.Sc. Global Logistics
Kühne Logistics University
Supervisors:
Prof. Dr. Maria Besiou
Prof. Dr. Irina Dolinskaya
Date: 31.07.2015
Name of Student: Sara Guerrero
Student ID: 231180001
Address: Schreyerring 8, 22309, Hamburg, Germany
Telephone number: +49 176 98591587
Email: sara.guerrero@gl.the-klu.org
2. i
Acknowledgement
Special thanks to the eight practitioners that agreed to share their experiences and
knowledge from the humanitarian sector. Their contribution is an important part of
this study.
I am very grateful for the supervision of Prof. Dr. Maria Besiou from the Kühne
Logistics University and Prof. Dr. Irina Dolinskaya from the Northwestern
University. Their invaluable support, guidance and enthusiasm drove me to the
achievement of this research.
I am indebted to my family and friends for their unconditional support.
3. ii
Table of Contents
Table of Contents..........................................................................................................ii
List of Figures..............................................................................................................iii
List of Tables ...............................................................................................................iv
List of Abbreviations ....................................................................................................v
Abstract........................................................................................................................vi
1. Introduction...............................................................................................................1
2. Research Methodology .............................................................................................2
3. Supply Chain Theoretical Framework......................................................................3
3.1. External challenges ............................................................................................8
3.2. Internal challenges..............................................................................................9
4. Distribution of Healthcare Goods in Emergencies: The Case of Ebola..................10
5. Interviews with Practitioners ..................................................................................14
5.1. Data process description...................................................................................14
5.2. Main findings ...................................................................................................18
5.2.1. The impact of external and internal challenges .........................................18
5.2.2. The impact of access..................................................................................21
5.2.3. The impact of the mission statement .........................................................22
6. Conclusions.............................................................................................................24
Appendices..................................................................................................................27
References...................................................................................................................98
Declaration of Authorship.........................................................................................102
4. iii
List of Figures
Figure 1 The six building blocks of a health system: aims and desirable attributes.
Source: WHO (2007) ....................................................................................................4
Figure 2 Stylized form of the supply chain of medical goods in emergencies. ............5
Figure 3 Main stakeholders of the supply chain of medical assistance in emergencies.
.......................................................................................................................................6
Figure 4 Supply chain theoretical framework of the logistical challenges impacting
the medical assistance in emergencies. Challenges identified in the literature review. 7
Figure 5 Supply chain theoretical framework of the logistical challenges impacting
the medical assistance in emergencies. Challenges identified in the literature review
and in the Ebola case study.........................................................................................11
Figure 6 Projection of the demand of PPEs versus the reality of the Ebola cases.
Source: POMS Conference (2015) .............................................................................13
Figure 7 Supply chain theoretical framework of the logistical challenges impacting
the medical assistance in emergencies. Challenges identified in the literature review,
in the Ebola case study and in the findings from the interviews with practitioners. ..17
Figure 8 Ranking of the main challenges of deploying medical programs in
emergencies as indicated by the respondents..............................................................18
Figure 9 Ranking of the main challenges of the medical supply chain in emergencies
as indicated by the respondents...................................................................................20
Figure 10 Strengths of MSF and ICRC identified by the respondents. ......................24
5. iv
List of Tables
Table 1 Reasons from IHO to not deploy medical assistance in emergencies ...........23
6. v
List of Abbreviations
CDC U.S. Centers for Disease Control and Prevention
DFID Department for International Development
ECHO European Commission’s Humanitarian Aid and Civil
Protection Department
HR Human resources
ICRC International Committee of Red Cross
IHO International Humanitarian Organizations
INGO International Non-Governmental Organization
MSF Médecins sans Frontières (Doctors without Borders)
POMS Production and Operations Management Society
PPE Personal protective equipment
UN United Nations
USAID United States Agency for International Development
WASH Water, sanitation and hygiene
WFP World Food Programme
WHO World Health Organization
7. vi
Abstract
Right after a disaster takes place, medical assistance is critical for the survival of
the victims (Fritz Institute, 2011; The Sphere Project, 2011). The awareness of the
challenges of the medical assistance is crucial for the effectiveness of the response.
For this reason, we identify its logistical challenges in emergencies. The contribution
of this research is twofold. First, we build a supply chain theoretical framework using
a concurrent triangulation research design. The framework encompasses: (1) the
logistical challenges identified by a review of academic and practitioner literature on
medical assistance; (2) the challenges identified from a case study of the response to
the Ebola outbreak in western Africa in 2014 and, (3) the logistical challenges
appointed by practitioners during structured interviews. Second, we answer two
research questions based on the results from the interviews: (1) Investigate whether
there is a reluctance or disengagement of the international humanitarian actors when
it comes to emergency medical assistance and, (2) Identify whether logistics or
supply chain challenges are part of the main root-causes that International
Humanitarian Organizations (IHO) face towards their effort to provide medical
assistance in emergencies.
8. 1
1. Introduction
The Ebola outbreak that affected western Africa in 2014 was declared by the
World Health Organization (WHO, 2014a) as a “public health emergency with
international concern” (para. 1). For the purpose of this research, the meaning of
emergency defined by the World Food Programme (WFP, 2005) is employed.
Hence, “[emergency] is a demonstrably abnormal event or series of events which
produces dislocation in the life of a community on an exceptional scale” (p. 3).
Donors and International Humanitarian Organizations (IHO) responded to the
Ebola emergency. The estimated funding reported was $1.53 billion (FTS, 2015).
This funding supported the mobilization of medical or healthcare1
goods
necessary to assist the victims. Nonetheless, according to Doctors without Borders
(MSF, 2015b) “the Ebola outbreak…exposed the reality of how inefficient and
slow health and aid systems are to respond to emergencies” (p. 4).
Humanitarian logistics2
played a very important role in the response to the
Ebola emergency. It is a key component of the aid systems and defined by
Thomas et al., (2005) as “the process of planning, implementing and controlling
the efficient, cost-effective flow and storage of goods and materials, as well as
related information, from point of origin to point of consumption for the purpose
of meeting the end of beneficiary’s requirements” (p. 60). In order to find out
what causes the inefficiencies in the supply of medical goods, we consider
relevant to identify the logistical challenges of the medical assistance in
emergencies.
Our research contribution is twofold. First, it presents a supply chain
theoretical framework identifying the main logistical challenges of the medical
assistance in emergencies. Second, through interviews with practitioners we
answer the following research questions:
Q1- Investigate whether there is a reluctance or disengagement of the
international humanitarian actors when it comes to emergency medical
assistance.
1
The terms medical and healthcare are used as synonyms.
2
This study does not make a distinction between the term supply chain and logistics, hence,
humanitarian supply chain is the same as humanitarian logistics.
9. 2
Q2- Identify whether logistics or supply chain challenges are part of the main
root-causes that IHO face towards their effort to provide medical assistance in
emergencies.
The theoretical framework is built based on data from three different sources.
Qualitative and quantitative data are analyzed and a concurrent triangulation
research is completed to converge the results (Creswell, 2009). The framework
encompasses: (1) the logistical challenges identified by a review of academic and
practitioner literature on medical assistance; (2) the challenges identified from a
case study of the response to the Ebola outbreak and, (3) the logistical challenges
appointed by practitioners during structured interviews.
In order to capture the logistical challenges, we developed an interviewer-
administered questionnaire with list and open questions to get some insights about
the position of the IHO regarding medical assistance in emergencies.
The main academic contribution of this study is the supply chain theoretical
framework that classifies the challenges into external and internal to the
management of the IHO. Furthermore, the findings from the interviews are also
an important part of this contribution. Based on our results, we identified laws and
regulations as the main logistical challenge in the medical assistance in
emergencies.
This thesis is organized as follows. Section 2 outlines the research
methodology. Section 3 introduces the supply chain theoretical framework based
on the literature review. Section 4 analyzes the logistical challenges of the Ebola
case. Section 5 describes the process of the interviews and summarizes the main
findings. Finally, Section 6 presents the conclusions of the study.
2. Research Methodology
This study combines qualitative and quantitative research techniques (mixed-
methods approach). It is based on concurrent triangulation strategy. The reason
behind the use of concurrent triangulation strategy was the possibility to converge
the qualitative and the quantitative results (Creswell, 2009) in a theoretical
framework.
10. 3
The qualitative phase encompasses the literature review and a case study
research. First, a review of academic and practitioner literature that distinguishes
the logistical challenges of the medical assistance in emergencies was completed.
Second, to illustrate a particular “example of a more general problem” (Flick,
2014, p. 122), a case study of the Ebola outbreak in west Africa in 2014 was
conducted. The logistical challenges of the assistance were identified in reports
published by IHO and practitioners. Moreover, the challenges mentioned by some
humanitarian actors part of the conference held by the Production and Operations
Management Society in May 2015 (POMS, 2015) were also included in the
framework.
To gather quantifiable data (Saunders et al., 2012), the quantitative phase
comprises the results of structured interviews conducted to logisticians, experts in
the field of emergency assistance and medical logistics. This study refers as
medical supply chain or medical logistics to the process of delivering healthcare
goods and healthcare assistance to the victims of a disaster. For the purpose of
this study, the meaning of disaster proposed by Van Wassenhove (2006) is used.
That is, “… a disruption that physically affects a system as a whole and threatens
its priorities and goals” (p. 476). Finally, the challenges appointed by the
respondents were also incorporated to the supply chain theoretical framework.
3. Supply Chain Theoretical Framework
A theoretical framework is developed by conducting a review of academic and
practitioner literature on medical assistance in humanitarian emergencies. This
framework identifies the logistical challenges of the medical assistance in
emergencies, which is one of the specific contributions of this research.
Right after a disaster takes place, medical assistance is critical for the survival
of the victims (Fritz Institute, 2011; The Sphere Project, 2011). As indicated by
The Sphere Project (2011) the objective of the humanitarian response is “to
maintain the crude mortality rate3
and under-5 mortality rate4
at, or reduce to, less
3
Crude mortality rate is defined by the Humanitarian Practice Network as “number of deaths
occurring in a given population at risk during a specified time period (also known as the recall
period). In emergencies, usually expressed as deaths per 10,000 persons per day; alternatively, as
deaths per 1,000 persons per month or per year” (Checchi et al., 2005, p. 36).
11. 4
than double the baseline rate documented for the population prior to the disaster”
(p. 292). After a disaster strikes, the Minimum Standards of Health should be
followed in order to reduce the excess mortality and morbidity and determine the
minimal levels of health service in emergencies. These standards are divided in
health systems and essential health services (The Sphere Project, 2011).
Health systems are defined by the WHO (2007) as “all the organizations,
people and actions whose primary intent is to promote, restore or maintain health”
(p. 2). It includes all the stakeholders implicated in the provision of medical
assistance from central to household level (The Sphere Project, 2011). The WHO
has designed a framework with six “building blocks” that constitute the system.
Figure 1 illustrates the system building blocks and their outcomes. These building
blocks are the base for the health system standards defined by The Sphere Project
and used during the response to a disaster.
Figure 1 The six building blocks of a health system: aims and desirable attributes. Source: WHO
(2007)
Essential health services address the medical needs of a population in the
aftermath of a disaster. They are described by The Sphere Project (2011) as
“preventive and curative health services” (p. 309) and are categorized in six
sections: control and communicable diseases such as cholera and tuberculosis;
child health for example vaccinations, newborn and childhood illness; sexual and
4
Under-5 mortality rate is defined by the Humanitarian Practice Network as the “number of deaths
occurring in a given population of under-five children during a specified time period” (Checchi et
al., 2005, p. 36).
12. 5
reproductive health (HIV/AIDS); injury such as trauma and surgical care; mental
health such as anxiety and, non-communicable diseases for example asthma,
diabetes and epilepsy.
Figure 2 illustrates the stylized form of the supply chain of medical goods in
order to deliver essential health services in emergencies.
Figure 2 Stylized form of the supply chain of medical goods in emergencies.
Important stakeholders are recognized in the supply chain process (Figure 3).
Manufacturers as GSK, Pfizer, Aventis, Hartmann, play a key role as producers of
healthcare goods. Manufacturers of drugs must have the certificate of Good
Manufacturing Practice and meet the WHO international standards of quality in
order to avoid substandard products and counterfeit (Sukkar, 2015; Yadav et al.,
2013). The producers supply to IHO and global wholesalers. The latter are
companies in charge of procuring and storing medical goods from multiple
companies. They also supply the IHO with medical kits,5
for example cholera,
Ebola, surgical instruments and dressing kits. Important wholesalers are Imres,
IDA Foundation and, Medical Export Group. Transport companies and 3PLs are
in charge of the movement of goods. Once the freights reach the affected country,
its government plays a key role in the supply chain- it approves the shipment to
come into the country and authorizes the IHO to enter its territory. The assistance
is highlighted by the media (Van Wassenhove, 2006) and supported by the
donors, as they are the most significant source of funding and often determine the
5
Medical kits are defined as “self-contained assortments of carefully selected goods in
predetermined quantities which are designed for providing specific services such as first aid,
medical treatment in a clinic or immunization services. Self-sufficient field hospitals which
include medical services as well as power and water supply are an extension of the kit concept”
(McGuire, 2011, p. 46).
13. 6
type and length of aid (Bogdanova, 2008; Koch et al., 2009; McGuire, 2011;
Oloruntoba et al., 2009).
Figure 3 Main stakeholders of the supply chain of medical assistance in emergencies.
As Kunz et al. (2012) established, the effectiveness in the humanitarian
logistics context is determined by “timely delivery of the right relief items” (p.
119). The awareness of the logistical challenges during the medical assistance in
humanitarian emergencies are crucial for the effectiveness of the response. The
theoretical framework presents the challenges encounter by the IHO that provide
essential health services after a disaster occurs in developing6
and least developed
countries7
. Following the classification presented by Pedraza Martinez et al.
(2011) of the potential factors affecting field vehicle fleet management of IHO.
We classify the logistical challenges into external and internal to the management
of the organization (Figure 4).
6
Other developing countries are classified by the United Nations as the ones which are neither
least developed countries nor developed countries. Examples are: Mexico, Brazil, Indonesia,
Philippines, Malaysia, Pakistan, China, Singapore, Kazakhstan, among others (UN Conference on
Trade and Development, 2014).
7
Least developed countries are designated by the United Nations Economic and Social Council
based on three criteria: (1) per capita income, (2) human assets and, (3) economic vulnerability. At
present there are 48 least developed countries. Examples are: Afghanistan, Haiti, Somalia, South
Sudan, Yemen, Myanmar (UN Conference on Trade and Development, 2014).
14. 7
Figure 4 Supply chain theoretical framework of the logistical challenges impacting the medical assistance in emergencies. Challenges identified in the literature review.
15. 8
3.1. External challenges
External challenges are outside of the direct management of the IHO. Clear
examples of them are demand uncertainty and, laws and regulations. Donations
are predominantly external, however the organization’s management might have
influence over them. Figure 4 shows donations on the spectrum between external
and internal challenges and located closer to the internal in comparison to the
other two.
According to Privett et al. (2014) and Yadav et al. (2010) demand uncertainty
is a major issue impacting the medical supply chain. Indeed, during complex
political emergencies demand is difficult to calculate as it changes based on the
type of war, the weapons used, intensity of the conflict and the health status of the
population (McGuire, 2011).
Yadav et al. (2010; 2013) have also identified that the production of drugs and
health commodities follow strict regulations and worldwide quality standards. In
this respect, specific laws and regulations apply during their importation to the
country affected by a disaster (McGuire, 2011). This process requires a great deal
of collaboration from the government affected as it must obey its national
regulations and legislations. This situation has been exposed by Sukkar (2015),
since the importation of drugs in the Middle East, specifically in Jordan, is
impossible due to regulatory constraints.
Jahre (2008) suggests that in-kind goods hinder the response. In this respect,
in-kind donations of drugs must follow the Guidelines for Medicine Donations by
the WHO. Hence, all donated medicines should have a remaining shelf-life of at
least one year and the international nonproprietary name or generic name has to
be included in the label. Additionally, the declared value of the donations is
required in the documentation that accompanied the shipment, the guidelines for
packaging and labelling must be followed, as well as, the appropriate disposal of
expired drugs (WHO, 2011).
16. 9
3.2. Internal challenges
Internal challenges are directly managed by the IHO. A clear example is lack
of expertise. Cold chain8
, quality, availability and capacity of domestic
transportation and warehouses are predominantly internal challenges however,
external factors and/or actors affect their management. Figure 4 presents these
four challenges on the spectrum between external and internal challenges.
The nature of medical goods refers to the physical and chemical characteristics
that commonly determine their transport and storage requirements (McGuire,
2011). These characteristics provoke the cold chain in their supply process.
Moreover, their expiration date is determined based on ideal transport and
warehousing conditions (Privett et al., 2014). Monitoring the temperature should
be done frequently during the entire supply chain. Storage conditions have to be
optimal with trained staff, proper warehouse equipment and right installations.
The quality of the product could be highly damaged in case of not meeting the
specifications of temperature, exposure to sunlight and humidity of the place
(WHO et al., 2006).
A problem during armed conflicts is that “domestic transportation and storage
capacities may be of limited quality, may have insufficient capacities, may not be
(immediately) available at all and may lack the necessary expertise for handling
healthcare goods” (McGuire, 2011, p. 203). These circumstances push the IHO to
come up with new alternatives to solve these challenges and deliver the healthcare
goods in the right condition.
Figure 4 summarizes the theoretical framework. External and internal
challenges impact the effectiveness of the medical supply chain and therefore, the
delivery of essential health services in emergencies. External challenges are not
directly managed by the IHO. Examples of them are: demand uncertainty,
donations and, laws and regulations. Internal challenges are directly managed by
the IHO. Lack of expertise, cold chain, quality, availability and capacity of
domestic transportation and storage are examples of internal challenges. The cold
chain could be affected by the quality of the vehicles and the warehouses.
Therefore, the framework shows an arrow that goes from the quality of domestic
8
Cold chain equipment includes “refrigerator, freezer, cold box, vaccines carrier, thermometer,
monitoring card” (McGuire, 2011, p. 334).
17. 10
transportation to the cold chain. Additionally, it shows another arrow that goes
from the quality of in-country warehouses to the cold chain. The next section
presents the logistical challenges encountered in the response to the Ebola
outbreak in 2014.
4. Distribution of Healthcare Goods in Emergencies: The
Case of Ebola
The Ebola virus disease has an average case fatality rate9
of 50% (WHO,
2015b) and has killed a total of 11,162 people in six countries (Data reported up to
May 31, 2015 (WHO, 2015a)). The outbreak in western Africa was first officially
reported on March 22, 2014 by the Guinea Ministry of Health. Liberia confirmed
cases on March 31 and, the Ministry of Health in Sierra Leone confirmed the first
case on May 26, 2014 (MSF, 2015b).
According to the U.S. Centers for Disease Control and Prevention (CDC,
2015) the transmission occurs when the broken skin or mucous membranes of a
person has direct contact with “blood or body fluids and objects of a person who
is sick with or has died from Ebola” (para. 6).
There are no specific therapies or vaccinations approved for the cure of this
illness, so during its treatment supportive care with essential medicines is
provided to lengthen the life of the patient (WHO, 2015c). The healthcare workers
assisting the patients, as well as cleaning and conducting safe burials, have to
wear a personal protective equipment (PPE) (WHO, 2015d). The PPE consists of
goggles or face shield (the effectiveness of both is equal, the choice mostly
depends on the preference of the organization and the health workers), fluid
resistant medical/surgical mask or fluid-resistant particulate respirator, double
gloves (preferable nitrile gloves), protective body wear (i.e., disposable gown and
disposable waterproof apron or disposable coverall and disposable waterproof
apron- gown and coverall should resist the penetration of blood and body fluids or
to blood-borne pathogens), waterproof boots and head cover (WHO, 2014c).
During the response, some logistical challenges were identified (Figure 5):
9
Case fatality ratio or rate, is defined by the Humanitarian Practice Network as “the proportion of
cases of a given disease that result in death” (Checchi et al., 2005, p. 36).
18. 11
Figure 5 Supply chain theoretical framework of the logistical challenges impacting the medical assistance in emergencies. Challenges identified in the literature review and in
the Ebola case study.
19. 12
External challenges: uncertainty in the demand of PPEs (DFID, 2014), lack of
global coordination of IHO regarding the suppliers of PPEs (POMS, 2015), ban
imposed by some airlines to fly to Ebola-affected countries (MSF, 2015b;
Sardo-Infirri et al., 2014) and, weak/lack of local infrastructures (Han, 2015).
Internal challenges: difficulties for securing private contractors for in-country
services (DFID, 2014).
Uncertainty in the demand of PPEs was caused by several factors. The
diagnose of infected people was problematic since the symptoms are similar to the
ones caused by malaria, cholera and influenza (MSF, 2015b; WHO, 2015c). In
addition, families hiding infected relatives at home (WHO, 2014d) and the
unknown number of people travelling between borders made it difficult to
forecast the cases in specific zones (MSF, 2015b). Besides, some remote areas
were impossible to investigate, either because of difficult access or due to low
cooperation from the community (WHO, 2014d). Therefore, the quantity of
healthcare goods needed for assistance was uncertain and, the picture of the level
of necessary response was not clear (DFID, 2014). This uncertainty provoked an
underestimation on the demand and, therefore, an urgency in upcoming
purchasing orders. Indeed, MSF reported that it was not until September 2014 that
the orders were forecasted based on real consumptions (Sardo-Infirri et al., 2014).
The shortage of PPEs affected the scale of response to the outbreak with some
organizations being unwilling to open a new clinic or expand their operations if
they did not have enough PPEs available for their healthcare workers. In addition,
the difficulty of forecasting requirements based on an uncertain demand provoked
a bullwhip effect in the supply chain (POMS, 2015). This phenomenon caused the
PPE manufacturers, such as DuPont to triple their production (Mcavoy et al.,
2014).
The lack of global coordination of the humanitarian agencies regarding the
suppliers of PPEs is another challenge characterizing this response. Because of the
nature of the virus, more than 50% of the protective gear is single use, and only
the goggles, boots and aprons could be disinfected and re-utilized (Sardo-Infirri et
al., 2014). This situation provoked a high level of demand that led to a
competition among agencies and consequential a price increase. For example, the
20. 13
Ebola PPE Price Index reported a coverall price, which reached $4.37 per piece
from an average price of $2.71. The boot covers also increased from an average of
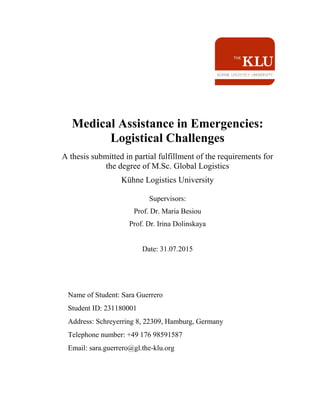
$0.52 per piece to a maximum of $2.28 (ECRI Institute, 2014). Figure 6 shows the
demand projected by the manufactures versus the actual observation. The slope of
the projection reflects the production of the manufacturers and a consecutive
increase of the cases. The slope opposes the concave shape of the reality, which
shows a peak of the number of victims within a short period of time. This figure
illustrates one of the main reasons for the shortage encountered by the agencies in
charge of the supply of PPEs.
Figure 6 Projection of the demand of PPEs versus the reality of the Ebola cases. Source: POMS
Conference (2015)
In terms of transport of medical goods, the movement of suppliers from outside
the country until reaching the Ebola care units10
and Ebola treatment centers11
presented distinctive challenges. The ban imposed by some airlines to fly to
Ebola-affected countries increased the already problematic situation of supply
(MSF, 2015b; Sardo-Infirri et al., 2014). Furthermore, the arrival of a great
quantity of materials in airports with weak infrastructure (e.g., the United States
10
Ebola care units are “established as complementary approach to prevent transmission in affected
areas at community level. Services will be monitoring suspected patients and basically providing
only oral treatment and other simple supportive/palliative care without injections or other similar
procedures” (WHO, 2014b).
11
Ebola treatment center “is where initial triage is done and patients with suspected Ebola are
strictly separated from those in whom the disease has been confirmed, and then treated. It can
include administering intravenous fluids and injections” (WHO, 2014b).
21. 14
Agency for International Development (USAID) transported more than 400
metric tons of medical and disaster items by air), challenged the teams of
logisticians to come up with viable solutions to move the items quickly from the
airports to the Ebola care units and treatment centers. In this respect, the USAID
and the WFP built a system of 5 different warehouses located in strategic zones
for the operations in Liberia. The warehouses received the supplies by trucks and
kept the Ebola care units and treatment centers running without issues of
shortages (Han, 2015). In terms of storage, the Department for International
Development (DFID, 2014) reported that “securing private contractor for in-
country services such as facilities management has been a considerable challenge”
(p. 6).
In summary, Figure 5 shows in red color the challenges identified during the
Ebola response. External challenges are uncertainty in the demand, lack of global
coordination of IHO, ban from airlines, weak/lack of local infrastructure. Securing
private for in-country services is considered as an internal challenge. The
framework shows a direct arrow that goes from the weak/lack of local
infrastructures to the demand uncertainty. That is because the number of Ebola
cases was unknown partially due to the impossibility to reach some remote areas.
The next section presents the main challenges identified by the experts in the field
of humanitarian aid.
5. Interviews with Practitioners
First, this section explains the type of data collected, the data collection
methods and the type of analysis carried out. Second, it elaborates on the main
findings and their impact on the theoretical framework.
5.1. Data process description
The focus group for this research was the organizations and practitioners
directly involved in the response to international emergencies as identified by the
research team. An introduction letter was sent by email to 30 candidates
(Appendix C). We received response from eight practitioners who participated in
the study. Due to anonymity requirements, the names of the organizations and the
participants are not mentioned. From here on, they are referred to as IHO-1 to 8.
A brief description of each respondent is given.
22. 15
IHO-1 Head of logistics and supply from an International Non-Governmental
Organization (INGO) that responds to emergency situations with clean
water, food, sanitation and protection.
IHO-2 Healthcare logistician with 20 years of experience in field projects and
with wide experience in the provision of healthcare goods in complex
political emergencies.
IHO-3 Procurement and logistics specialist from an INGO that focuses on
children’s development by promoting child rights and education.
IHO-4 Coordinator of an INGO in the area of international logistics.
Permanently based in the operational center in charge of procurement,
warehousing and deployment of medical items.
IHO-5 Logistics officer representing an INGO in charge of providing
lifesaving medical and healthcare related emergency services.
IHO-6 Practitioner with 20 years of experience in a medical INGO. Part of the
operational center in charge of procurement, warehousing and
deployment of medical items.
IHO-7 Practitioner in the area of logistics with more than 10 years of
experience. Part of the operational center of an INGO in charge of
providing medical and healthcare related emergency services.
IHO-8 Director of operations from a private company that offers procurement,
logistics and consultancy services to social institutions.
Data was collected thru structured interviews. Between April, 2015 and June,
2015 the total of interviews were conducted. Appendix A shows the breakdown of
conducted interviews specifying the date. Appendix D presents the interviewer-
administered questionnaire used during the interviews. The questions focused on
the type and speed of the medical deployment in emergencies, the challenges of
the medical assistance in emergencies and the position of the organization during
the Ebola outbreak in 2014. The questions were tested with a practitioner to check
if the content was clear and understandable. The questionnaire was modified three
times taking in consideration comments given by the participants. Appendix B
compiled the changes made. The participants were asked the same questions in
23. 16
the same order. However, some questions were not applicable to the four
participants that do not deploy direct medical assistance or do not represent any
specific organization (IHO-1, IHO-2, IHO-3 and IHO-8).
All the interviews were conducted by the same researcher. The interviews were
conducted via Skype call. By using the modality of “share screens” the
participants were able to look at the questions while the conversation was taking
place. The interviews were recorded except in two cases when the questionnaire
was answered via email and in one case when the interviewee requested
otherwise. The average duration of an interview was 60 minutes. The answers
were sent for approval after the interview. The completed questionnaires are given
for reference in the section of appendices (appendix E corresponds to IHO-1 and
the subsequent appendices follow the numerical order until appendix L).
List questions were asked to reveal the level of involvement of each
organization in medical and logistical activities and to identify the challenges of
these activities. The multi-response variables were converted in a set of indicator
variables with two categories. Number one (1) indicated that the option was
chosen by the participant and cero (0) that the option was not elected.
Open questions provided us with detailed answers of the point of view of each
respondent (Saunders et al., 2012). A comparison of the answers was conducted to
reveal new statements and to identify the generalizable ones (Flick, 2014). The
preliminary analysis allowed us to focus on the logistical challenges appointed by
the respondents. The next section presents the main findings and the final version
of the supply chain theoretical framework (Figure 7).
24. 17
Figure 7 Supply chain theoretical framework of the logistical challenges impacting the medical assistance in emergencies. Challenges identified in the literature review, in the
Ebola case study and in the findings from the interviews with practitioners.
25. 18
5.2. Main findings
Sub-section 5.2.1 and 5.2.2 presents the main findings regarding the logistical
challenges. Sub-section 5.2.3 presents the main findings regarding the mission
and characteristics of the organizations involved in deploying medical assistance.
5.2.1. The impact of external and internal challenges
During the response to an emergency, many logistical and medical activities
take place. Additional to the processes of supply such as, procurement,
warehousing and transportation of medical and relief goods, the IHO must set up
healthcare sites with electricity, water supply systems and waste disposal areas.
Moreover, they conduct the maintenance of bio-medical and diagnostic imaging
equipment in addition to the maintenance of the fleet equipment of medical
vehicles such as, mobile clinics and ambulances. Respondents involved in medical
direct assistance indicated that supply processes and healthcare site management
are the major challenges in the deployment of aid. Medical equipment
management ranked as a second place. Electrical and water installations, waste
management and fleet management of medical vehicles received just one voted
each (Figure 8).
Figure 8 Ranking of the main challenges of deploying medical programs in emergencies as
indicated by the respondents.
Furthermore in the same question, IHO-6 indicated that none of the challenges
previously described is a main challenge and discussed the following statement:
26. 19
The real challenge in emergencies is to be ready as soon as possible, in other
words, capacity of fast deployment. In a short period of time we have to be
operational for the assistance. This time is crucial and makes the difference
between the capacity of an organization to intervene or not in a disaster. For
example, if you are not in the site during the first 48 hours after an earthquake,
then you completely missed the emergency. After a week it is not called
anymore emergency but post-emergency and the nature of the support in post-
emergencies is completely different….
Capacity of fast deployment impacts all the activities previously mentioned.
Not just the supply of medical goods needs to be fast but the deployment of
people and technical items to setup the operation has to be done immediately after
a disaster. This variable can be directly managed by the IHO however it is also
affected by external actors and/or factors. Taking that into consideration, we
classify capacity of fast deployment as an internal challenge and located in the
spectrum between internal and external challenges (Figure 7).
As previously mentioned, the supply of medical goods encompasses a variety
of activities. Figure 9 shows the ranking of challenges of the supply chain. The
100% of the sample indicated that issues of importation such as customs clearance
and national legislations, are the major logistical challenge to deploy medical
programs. As previously discussed in sub-section 3.1, the importation of drugs
and health commodities requires a great deal of collaboration from the
government of the affected country. During the interviews, the participants
expressed several times these complications. Sometimes even if the State of
emergency is declared, certain legislations slow down the importation of goods
impacting the assistance of the organization. The response in the aftermath of the
Myanmar cyclone on May 2, 2008 is a clear example of this challenge. The
national government denied visas to health workers and delayed the importation
of relief items until May 7 when it decided to waive the customs charges and
clearances after the United Nations for Humanitarian Affairs and Emergency
27. 20
Relief Coordinator asked the government to collaborate and allow the access to
the country (UN News Centre, 2008).
Figure 9 Ranking of the main challenges of the medical supply chain in emergencies as indicated
by the respondents.
The second major challenge of the supply chain is the procurement of items
(Figure 9). Participants highlighted that issues regarding licenses and regulations
of pharmaceuticals are the major concern within the procurement of drugs. The
situation in India where the organizations must procure locally was given as an
example by IHO-6. The position from the government to deny the importation of
drugs provokes to the IHO to seek for national suppliers that meet the required
quality. When the product is not available, the IHO seek for alternative
therapeutics that meet their protocol. This situation impacts shortages of
medicines and therefore, jeopardizes the supply chain operation.
Procurement processes were followed by order management that includes
issues such as the order of too many items or the codification of them (Figure 9).
As IHO-3 indicated, “the quantity of items to be ordered is determined by the
demand. If the demand is highly variable then it is impossible to be accurate in the
order”. Furthermore, as previously discussed in sub-section 3.2., the expiration
date is important in the supply of healthcare goods. During the order of medical
products, the remaining shelf-life must be considered to avoid expiry and loss of
items (McGuire, 2011). Too many items with a short remaining shelf-life could
provoke loss of stock. As the process of ordering is managed by the organization,
this challenge is classified as an internal (Figure 7).
28. 21
Shipping and warehouse management received one vote each. However, IHO-5
discussed, “in some countries there are no proper warehouses…so we have
difficulties to control the temperature and the humidity. In some places we even
have issues with domestic electricity and we run the warehouses using generators.
A clear example is South Sudan”. This statement supports our previous
observation, in sub-section 3.2, that the quality of in-country warehouses affects
the cold chain.
The capacity to find human resources with appropriate skills is not appointed
as a major challenge (Figure 9). However IHO-4, IHO-6 and IHO-7 discussed that
the complexity of current medical programs require higher professionalization.
The maintenance of X-ray equipment was given as an example. The organizations
needed to hire an expert that visits field operations given maintenance. As
discussed in sub-section 3.2., lack of expertise is an internal challenge and can be
directly managed by the organization.
5.2.2. The impact of access
Access to the beneficiaries is referred by the respondents to as the main
constraint of the deployment of medical assistance in emergencies. As explained
in the previous sub-section, the government of Myanmar did not let the IHO
access into the country. Consequently, the necessary aid did not arrive to the
beneficiaries in the first 72 hours and the first phase of the assistance was missed.
As one of the interviewees indicated “when nothing works is mainly because of
access, when there is access, the rest is a challenge”.
The respondents indicated three main external challenges that cause
inaccessibility to a disaster area: laws and regulations, security of the
humanitarian workers during armed conflicts and, lack of infrastructure in the
affected country. In the previous sub-section, we have explained the impact of
laws and regulations. Therefore, this sub-section focuses on the security during
armed conflicts and, the lack of infrastructure in the affected country.
We classify security as an external challenge. It is located on the spectrum
between external and internal challenges (Figure 7). It is outside the management
of the IHO, however to secure their workers the IHO have some options. First, try
to negotiate with armed groups and ensure the assistance. Negotiations with the
29. 22
parties of an armed conflict are particularly difficult. The power imbalance
between the IHO and the armed group during the negotiation (the latter can
employ coercive armed force) places the organization in a vulnerable situation
(McHugh et al., 2006). Second, deploy assistance by remote management. By this
option, the organization is represented only by local people. They distribute
medical items to the hospitals and assist the victims without having international
staff inside the country (international staff can be seen as enemies). Syria and
Somalia were mentioned as examples of places where remote management is
conducted by some organizations.
As previously indicated in Section 4, lack of local infrastructure is an external
challenge. IHO-3 discussed the difficulty to assist affected people due to
inaccessibility caused by damaged roads. The Haiti Earthquake in 2010 is a clear
example of its impact to the medical assistance. The limited availability of routes
to mobilize people for treatment was a main bottleneck faced by the IHO (Pedraza
Martinez et al., 2010).
In summary, Figure 7 shows in green color the challenges indicated by the
respondents. External challenges are security, laws and regulations and demand
uncertainty. Internal challenges are capacity of fast deployment, order
management, quality of in-country warehouses and lack of expertise. The
framework shows a direct arrow that goes from the demand uncertainty to the
order management. The reason is that the unknown demand impacts directly the
quantity of products to be ordered. Additionally, another direct arrow goes from
the laws and regulations to the order management. This is because laws and
regulations limit the IHO to procure locally. Besides the logistical challenges
identified by the respondents, some of the participants also provided an
explanation of the main reasons to not deploy medical assistance in emergencies.
5.2.3. The impact of the mission statement
The purpose of every organization is driven by its mission statement. The
representative from organizations that are not involved in medical assistance
confirmed this (Table 1).
30. 23
Reasons for the organizations to not deploy medical assistance in
emergencies
IHO-1 The organization has historically developed its programs based on
other expertise and is already too stretched across other areas to want
to become a medical agency too.
IHO-3 Three main reasons: (1) other INGOs are already covering all medical
needs, (2) Human resources (HR) constraints (lack of available
medical resources in the organization, high turn-over) and, (3) our
mission is not related to medical assistance. Indeed, the organization
has a partnership with other medical related organization. In this way
not just medical programs are supported but also other type of
assistance is provided by us.
IHO-8 The organization is a procurement and logistics provider for all types
of programs, we do not provide medical aid.
Table 1 Reasons from IHO to not deploy medical assistance in emergencies
MSF and the International Committee of Red Cross (ICRC) were indicated by
the participants as the most effective organizations to provide medical assistance
in emergencies, including during armed conflicts. Both organizations have as
mission statement to deliver emergency aid (ICRC, 2008; MSF, 2015a).
Figure 10 presents the strengths of these two organizations as identified by the
respondents. Four main characteristics are shared between the two: expertise in
health emergencies, experience in conflict areas, standardized approaches and
logistics capacity. Furthermore, MSF is distinguished for its independence, its
ability to access remote areas, its medical kits system and its recognition as
vendors by USAID and by the European Commission’s Humanitarian Aid and
Civil Protection (ECHO). ICRC is well-known for its international standing,
financial resources and its global network of people.
31. 24
Figure 10 Strengths of MSF and ICRC identified by the respondents.
6. Conclusions
This study identifies the logistical challenges of the medical assistance in
emergencies. A theoretical framework is developed based on academic and
practitioner literature. The later includes the reports of the logistical challenges
encountered during the response to the Ebola outbreak in 2014. The framework
also comprises the challenges indicated during structured interviews with eight
experts in the field of humanitarian and medical logistics. The logistical
challenges are classified in external and internal to the management of the IHO.
Challenges outside the direct management of the IHO were classified as
external challenges. Within the external challenges, laws and regulations are a
great concern within the IHO. National regulations of importation of drugs are
increasing and pushing the organizations to procure drugs in the local market. By
procuring nationally the shortage of products is more likely to happen. The IHO
have to assure that the national suppliers meet the WHO standards of quality to
avoid counterfeit and substandard products. Furthermore, a competition between
IHO occurs when the number of national wholesalers certificated is not able to
meet the demand. Moreover, this competition derives in a price increase of the
products. Finally, the assistance can be stopped in cases where the organization is
unable to cope with the regulations of the affected country.
32. 25
Demand uncertainty is another external challenge that impacts the assistance
intended to deliver. During the Ebola response, the uncertainty in the demand of
PPEs affected the supply chain and created a bullwhip effect. The manufacturers
of PPEs did not meet the number of items required by the IHO. This prevented
some organizations from opening new Ebola treatment centers because of lack of
protective gears for their healthcare workers.
The weak infrastructure of the affected country also exemplifies another
external challenge. The IHO commonly have to come up with creative solutions
to bring the relief items to the beneficiaries. Indeed, during the Ebola response,
the items were quickly moved from the airports to five different warehouses built
by some organizations in strategic points of the affected country.
Additional to external challenges are the internal challenges. The latter are
directly managed by the IHO. Lack of expertise is a clear example. Hiring an
expert on X-rays that visits field operations given maintenance to the equipment,
exemplifies how the IHO are able to manage this challenge.
Capacity of fast deployment is an internal challenge that affects the
effectiveness of the medical assistance. The speed to deploy and install medical
equipment, medical vehicles, healthcare structures (including electrical and water
installation) is fundamental for the response to an emergency. The medical
assistance given in the first days after a natural disaster differs from the assistance
provided after several weeks.
The cold chain exemplifies another internal challenge. The quality of the drugs
could be highly impacted in cases were the cold chain is not met, therefore, the
temperature plays an important role during the transportation and storage of drugs.
This research has some limitations. First, it is limited to eight interviews. This
was necessary to get an opinion of the major logistical challenges of the medical
assistance in emergencies but it limits the generalization of the findings. Second,
the interviews were conducted to mostly INGOs and one private company.
Further research needs to be extended to donors, governmental organizations and
UN agencies. This limitation arose from the limited time to conclude this study.
33. 26
Finally, concerning our research questions, sub-section 5.1 answers the second
research question (Q2). Hence, we conclude that logistical challenges are part of
the main root-causes that IHO face towards their efforts to provide medical
assistance in emergencies. However in regards to our first research question (Q1),
there is a lack of evidence to determine if a reluctance or disengagement reaction
from the humanitarian actors towards bringing medical assistance in emergencies
exists. Therefore, the first research question (Q1) cannot be answered based on
the conducted analysis. Although, this study suggests a strong relationship
between the mission of the IHO and their involvement in the medical response
(Table 1), further research has to be conducted. In this respect, an analysis of the
humanitarian organizations that stopped deploying medical assistance in
emergencies or/and changed their mission is recommended to be developed.
Interviews to determine the root-causes of this decision could be valuable.
34. 27
Appendices
Appendix A. Summary of interviews
Date Organization Activity
June 3,2015
IHO-1
Completed questionnaire
received via email
June 11,2015 IHO-2 Interview
June 23,2015 IHO-3 Interview
June 4,2015 IHO-4 Interview
June 5,2015 IHO-5 Interview
June 19,2015 IHO-6 Interview
June 19,2015 IHO-7 Interview
June 19,2015
IHO-8
Completed questionnaire
received via email
Appendix B. Summary of modifications to the questionnaire
Date Modifications
June 4, 2015 The word “constraint” was changed to “challenge” in all the
questions
June 12, 2015 Question 5: the word “INGOs” was changed to
“international humanitarian organizations”
June 18, 2015 Question 11.A. was added.
June 22, 2015 Question 11.B. was added.
35. 28
Appendix C. Introduction letter
PROVIDING MEDICAL ASSISTANCE IN EMERGENCY SITUATIONS:
LOGISTICAL CHALLENGES
Numerous studies have been conducted regarding the diverse processes involved
in the logistics of the humanitarian sector. Practitioners and academics have
investigated some of the main constraints and obstacles triggering the complexity
of these processes. The practical expertise combined with the academic
knowledge have been put together to help the humanitarian community improve
the accuracy and effectiveness of its support.
Major humanitarian crises that occurred during the past decade have required a
large-scale emergency response aiming at providing medical assistance to affected
people. However, there have been some critics to international organizations
regarding lack of sufficient response when it comes to:
Treat infected populations during to an outbreak: e.g., the Haiti Cholera
outbreak in 2010- where access was opened and funding was given to re-build
the country and the estimated 80% of the cases were attended by just two
organizations during the first three months of the outbreak (Biquet, 2014).
While providing healthcare assistance during a conflict, as it was the case in
North Kivu, Democratic Republic of Congo in 2012 where “many agencies’
programmes evaporated as soon as the emergencies occurred” (Healy et al.
2014, p. 32).
While organizing healthcare structures during an acute phase of malnutrition
of large displacement of populations: during the response to Maban County in
South Sudan in 2012 many humanitarian agencies were too slow to respond to
the increasing number of malnourished people (Begum, 2013). Additionally,
the slowness on the implementation of healthcare structures influenced the
mortality rate reported of 1.79 deaths per 10,000 per day during April and
May 2012 (Healy et al., 2014).
Aiming to better understand the characteristics of the medical assistance in
emergency situations and the corresponding obstacles, we need to collect
information from hands on humanitarian organizations that are involved in health.
Through the interviews, we hope to determine whether some of the stakeholders
are more inclined to bring first-aid medical assistance than others and if the
operational choices of the humanitarian response are influenced by logistics
constraints or not. The study will also attempt to highlight if there is any higher
reluctance and gradual disengagement reaction of main international aid actors
towards the medical assistance in emergencies.
36. 29
Appendix C (Continued)
General Objective –
Ultimately, the goal of this research is to identify the major obstacles and
challenges related to medical logistics in order to provide some guidance to the
humanitarian community to overcome these obstacles and provide a more
effective and impactful response to future crises.
Scope of the research –
The selection of the interviewees has been done according to the following
criteria:
International emergency deployment: although the national response capacity
– public and private – is an essential ‘first responder’, the survey is focusing
on improving the speed and appropriateness of the response of international
organizations when national stakeholders are not able to meet the medical
needs of the affected population;
Humanitarian professional response: interviews are addressed to the work of
organizations which provide humanitarian assistance at the very core of their
activities. Contributions from commercial companies, military actors and civil
societies (diaspora, faith-based activism, etc.) are very significant; however,
they are also engaged in one-shot response with limited possibility for
benchmarking with international NGOs.
Direct assistance: the survey is targeting humanitarian organizations that
provide direct assistance to affected populations – i.e., engaging their legal
responsibility towards the patients (e.g., INGOs, the Red Cross and Red
Crescent Movement) – before considering improvement of the work of
humanitarian agencies that are mandated to support them and will hardly ever
be on the first line response (e.g., donors).
The research aims at improving the performance of logistics services in charge of
the deployment, maintenance and the supply of emergency medical programs. It
includes the opening and relocation of temporary and semi-permanent health
structures (Ebola/cholera treatment centers, field hospitals and health centers,
vaccination sites) and the logistical support to mobile activities (Mobile clinics,
1staid medical assistance during Search & Rescue operations, Ambulance
services, etc.).
Research questions –
1. Investigate whether there is a reluctance and disengagement process of the
international aid actors regarding emergency medical assistance.
2. Identify if logistics and supply chain constraints are part of the main root-
causes that donors and international aid organizations face towards the
effort to provide a medical assistance in emergency situation.
37. 30
Appendix C (Continued)
Anonymity of the interviewee –
The identity of the interviewee will remain anonymous and after each interview
the answers and comments collected will be emailed to the interviewee in order
for him/her to approve them.
Structure of the questionnaire –
The questionnaire has a total of 15 questions; 12 questions are multiple choice and
3 are open questions.
References –
Begum, S. (2013). Upper Nile Refugee Crisis: Avoiding past mistakes in the
coming year. Briefing Paper. Retrieved from
http://www.nhsmun.org/sites/default/files/Upper%20Nile%20Refugee%20Crisis
%20%20Avoiding%20Past%20Mistakes%20in%20the%20Coming%20Year.pdf
Biquet, J.-M. (2014). Haiti: Between Emergency and Reconstruction: An
inadequate response. Retrieved from http://poldev.revues.org/pdf/1600
Healy, S., & Tiller, S. (2014). Where is everyone? Responding to emergencies in
the most difficult places: A review of the humanitarian aid system's response to
displacement emergencies in conflict context in South Sudan, eastern Democratic
Republic of Congo and Jordan, 2012-13. Medecins Sans Frontieres. Retrieved
from http://www.msf.org/sites/msf.org/files/msf-whereiseveryone_-def-lr_-
_july.pdf
38. 31
Appendix D. Interviewer-administered questionnaire
Reference number: _____
MEDICAL ASSISTANCE IN EMERGENCIES: LOGISTICAL
CHALLENGES. QUESTIONNAIRE.
1. Is your organization regularly involved in medical assistance during its
response to emergency situation?
☐Yes ☐No
A. If yes, what kind of medical activities your organization can provide
independently without relying on local/diaspora organizations or/and
affected government?
☐Hospital activities ☐Surgical care
☐Reproductive care ☐Primary healthcare
☐Mobile clinics ☐Mental Healthcare
☐Therapeutic nutrition center ☐Health promotion
☐Vaccination campaign during an outbreak (meningitis, polio, measles,
etc.)
☐Treatment of communicable diseases (cholera or Ebola centers, etc.)
☐Treatment of non-communicable disease (diabetes, cancer, etc.)
☐Other
B. If yes, what was the average budget your organization has dedicated to
medical assistance in 2014?
☐Less than 25% ☐50% to 70%
☐25% to 50% ☐More than 70%
C. If no, what are the main reasons for not deploying regular medical
assistance?
☐Other INGOs are already covering all medical needs.
☐Financial constraints (medical operation are too expensive, lack of
private funding, etc.)
☐Donors constraints (heavy reporting system, lack of funding for medical
stocks, etc.)
☐HR constraints (lack of available medical resources in the organizations,
high turn-over, etc.)
39. 32
Appendix D (Continued)
☐Logistics constraints (complex supply chains, heavy maintenance for
biomedical equipment, lack of central pharmaceutical procurement/stock
capacity, cold chain, expired drugs, etc.)
☐Security constraints (medical assistance often targeted)
☐Lack of WHO support (little technical support/donation in terms of
medical products and warehousing compare to other UN agencies)
☐Lack of medical inter-agency coordination (regular overlap or
uncovered gaps)
☐Others.
2. Has your organization managed emergency healthcare structures to admit sick,
wounded, or pregnant people during the following emergency situations?
Without partnership12
With partnership
(No use of 3rd party org., local/diaspora NGOs)
Pakistan earthquake – 2005 ☐ ☐
Myanmar cyclone – 2008 ☐ ☐
China earthquake – 2008 ☐ ☐
Gaza war – 2009 ☐ ☐
Zimbabwe cholera – 2010 ☐ ☐
Haiti earthquake – 2010 ☐ ☐
Haiti cholera outbreak – 2010/11 ☐ ☐
Libya conflict - 2011 ☐ ☐
Syria conflict – from 2011 ☐ ☐
CAR conflict – 2011 ☐ ☐
Philippines cyclone – 2013 ☐ ☐
West Africa Ebola outbreak – 2014 ☐ ☐
Gaza war- 2014 ☐ ☐
Nepal earthquake – 2015 ☐ ☐
Yemen conflict – 2015 ☐ ☐
12
Direct assistance with no use of third party organization, local/diaspora NGOs, governmental
structure, etc.
40. 33
Appendix D (Continued)
3. What are the main reasons your organization usually prefers to develop
partnership for medical response in emergency?
☐Local actors/public organizations know better how to respond
☐Partners have appropriate medical HR resources
☐Type of medication and protocols are more adapted to the patients
☐Faster implementation
☐Other
Explain
4. What kind of medical deployment does your organization usually develop in
emergency?
☐Direct assistance with permanent presence of international health
workers (no third party involved)
☐Remote control management (direct assistance but no permanent
presence of the international health workers)
☐Partnership (bilateral agreement with private/public healthcare structure,
field hospital, etc.)
☐Support (medical donation, financial support, medical training, etc.)
☐Other.
Explain
5. From your field experience, what are the main logistical challenges that the
international humanitarian organizations (INGOs, governmental organizations,
UN agencies) are facing when deploying medical programs in emergency
situation?
☐Supply chain (procurement, warehousing, shipping, etc.);
☐Healthcare structure / site management (design and maintenance of field
hospitals, cholera treatment center, vaccination site, etc.);
☐Equipment management (maintenance of bio-medical equipment,
diagnostic imaging equipment, etc.);
41. 34
Appendix D (Continued)
☐Fleet management (ambulance services, med air operations; Search &
Rescue, mobile clinics);
☐Electrical and water installations for healthcare structures;
☐Medical disposal, waste management;
☐Other.
6. What do you think are the main challenges for your organization to provide
medical assistance in emergency? What should be done to improve the situation?
Explain
7. When it comes to the supply of healthcare goods in emergencies, what do you
consider are the main challenges?
☐Order management (too many items can be ordered, codification of
items, etc.)
☐Procurement (pharmaceutical purchase capacity, license-regulatory
issues, quality assurance, quality control, etc.)
☐Warehousing management (temperature/humidity constraints, expiring
product, cold chain, etc.)
☐Shipping (cold chain issue, etc.)
☐Importation and exportation (customs constraints, national legislations
and regulations, etc.)
☐Supply HR capacity – skills
☐Other
8. In emergency, what kind of international/regional supply chain structure your
organization usually relies on?
☐Internal integrated pharmaceutical supply center (in-house international
procurement unit, internal warehousing /shipping service, etc.);
☐Outsourced supply center (outsourcing part or all the international
supply chain to private sector or/and UNHRD);
☐Direct delivery from pharmaceutical companies;
42. 35
Appendix D (Continued)
☐Combined integrated and outsourced system;
☐Local procurement capacity only (no international supply center);
☐Other
Explain
9. At local level, what department is in charge of the medical supply chain in your
organization?
Logistics/supply Another department
Department (describe)
Medical ordering ☐ ☐ _______________
Pharmaceutical procurement ☐ ☐ _______________
Medical warehousing ☐ ☐ _______________
Medical shipping ☐ ☐ _______________
Custom clearance for medical items ☐ ☐ _______________
Maintenance of medical structure ☐ ☐ _______________
Maintenance of medical equipment ☐ ☐ _______________
Transport of patient ☐ ☐ _______________
Medical disposal ☐ ☐ _______________
Explain
10. Do you believe that logistics/supply chain challenges are the main obstacles
for the international humanitarian organizations to deploy medical assistance in
emergencies?
☐Yes ☐No
Explain
11. From your field experience, how do you believe the logistical challenges to
provide medical assistance in emergency are changing?
☐Increasing challenges
☐Stable challenges
☐Decreasing challenges
43. 36
Appendix D (Continued)
Explain
A. Base on your perception, how the medical programs have evolved or change
over the past 5 and 10 years?
Explain
5 years-
10 years-
B. How do you consider the number of international humanitarian organizations
responding to medical emergencies has changed over the past 5 years?
☐The number has increased
☐The number is stable and remains the same
☐The number has decreased
Explain
12. During the West Africa outbreak, was your organization engaged in treating
patients infected by the Ebola virus?
☐Yes ☐No
A. If yes, what would you do to improve the logistics/supply set-up for a
future Ebola response?
B. If no, why? (If the answer is because the INGO has never operated in
Ebola context, please explain.)
13. Some criticism inside and outside the humanitarian community has arisen
regarding the late medical response to the last year’s Ebola outbreak.
A. Comment on your own operation. What would you have done differently?
44. 37
Appendix D (Continued)
B. Have you implemented some changes in your supply chain caused by the
Ebola outbreak or are you planning to perform some changes? Specify the
changes and the expected results.
14. In case of future large-size humanitarian outbreak or earthquake without major
access/security constraints, how quickly can your organization deploy a ready-to-
use healthcare structure?
☐Cholera Treatment Unit (50 beds) Mini. Delays: days
☐Ebola Treatment Unit (50 beds) Mini. Delays: days
☐Field hospital with surgical capacity
(50 beds) Mini. Delays: days
☐Mobile clinics (10 teams) Mini. Delays: days
☐Maternity (10 beds) Mini. Delays: days
☐Therapeutic nutrition center Mini. Delays: days
☐Set-up for vaccination campaign
(300.000 target pop.) Mini. Delays: days
Comment
15. From your perspective, what are the three most effective international
humanitarian organizations when it comes to providing direct medical assistance
in emergencies? Could you explain why?
#1 Main strengths:
#2 Main strengths:
#3 Main strengths:
We sincerely appreciate your time and collaboration for the achievement of this
study. We will send you the transcripts of your answers shortly via email. Feel
free to correct and comment on them.
In case of any questions or comments please email Sara Guerrero to
sara.guerrero@gl.the-klu.org
45. 38
Appendix E. Completed questionnaire: IHO-1
Reference number: IHO-1
MEDICAL ASSISTANCE IN EMERGENCIES: LOGISTICAL
CHALLENGES. QUESTIONNAIRE.
1. Is your organization regularly involved in medical assistance during its
response to emergency situation?
☐Yes ☒No
A. If yes, what kind of medical activities your organization can provide
independently without relying on local/diaspora organizations or/and affected
government?
☐Hospital activities ☐Surgical care
☐Reproductive care ☐Primary healthcare
☐Mobile clinics ☐Mental Healthcare
☐Therapeutic nutrition center ☐Health promotion
☐Vaccination campaign during an outbreak (meningitis, polio, measles,
etc.)
☐Treatment of communicable diseases (cholera or Ebola centers, etc.)
☐Treatment of non-communicable disease (diabetes, cancer, etc.)
☐Other
B. If yes, what was the average budget your organization has dedicated to
medical assistance in 2014?
☐Less than 25% ☐50% to 70%
☐25% to 50% ☐More than 70%
C. If no, what are the main reasons for not deploying regular medical
assistance?
☐Other INGOs are already covering all medical needs.
☐Financial constraints (medical operation are too expensive, lack of
private funding, etc.)
☐Donors constraints (heavy reporting system, lack of funding for medical
stocks, etc.)
☐HR constraints (lack of available medical resources in the organizations,
high turn-over, etc.)
46. 39
Appendix E (Continued)
☐Logistics constraints (complex supply chains, heavy maintenance for
biomedical equipment, lack of central pharmaceutical procurement/stock
capacity, cold chain, expired drugs, etc.)
☐Security constraints (medical assistance often targeted)
☐Lack of WHO support (little technical support/donation in terms of
medical products and warehousing compare to other UN agencies)
☐Lack of medical inter-agency coordination (regular overlap or
uncovered gaps)
☐Others. The organization has historically developed its programs based
on other expertise and is already too stretched across other areas to want
to become a medical agency too.
2. Has your organization managed emergency healthcare structures to admit sick,
wounded, or pregnant people during the following emergency situations?
Without partnership13
With partnership
(No use of 3rd party org., local/diaspora NGOs)
Pakistan earthquake – 2005 ☐ ☐
Myanmar cyclone – 2008 ☐ ☐
China earthquake – 2008 ☐ ☐
Gaza war – 2009 ☐ ☐
Zimbabwe cholera – 2010 ☐ ☐
Haiti earthquake – 2010 ☐ ☐
Haiti cholera outbreak – 2010/11 ☐ ☐
Libya conflict - 2011 ☐ ☐
Syria conflict – from 2011 ☐ ☐
CAR conflict – 2011 ☐ ☐
Philippines cyclone – 2013 ☐ ☐
West Africa Ebola outbreak – 2014 ☐ ☐
Gaza war- 2014 ☐ ☐
Nepal earthquake – 2015 ☐ ☐
Yemen conflict – 2015 ☐ ☐
13
Direct assistance with no use of third party organization, local/diaspora NGOs, governmental
structure, etc.
47. 40
Appendix E (Continued)
3. What are the main reasons your organization usually prefers to develop
partnership for medical response in emergency?
☐Local actors/public organizations know better how to respond
☐Partners have appropriate medical HR resources
☐Type of medication and protocols are more adapted to the patients
☐Faster implementation
☐Other
Explain
4. What kind of medical deployment does your organization usually develop in
emergency?
☐Direct assistance with permanent presence of international health
workers (no third party involved)
☐Remote control management (direct assistance but no permanent
presence of the international health workers)
☐Partnership (bilateral agreement with private/public healthcare structure,
field hospital, etc.)
☐Support (medical donation, financial support, medical training, etc.)
☐Other.
Explain
5. From your field experience, what are the main logistical challenges that the
international humanitarian organizations (INGOs, governmental organizations,
UN agencies) are facing when deploying medical programs in emergency
situation?
☐Supply chain (procurement, warehousing, shipping, etc.);
☐Healthcare structure / site management (design and maintenance of field
hospitals, cholera treatment center, vaccination site, etc.);
☐Equipment management (maintenance of bio-medical equipment,
diagnostic imaging equipment, etc.);
48. 41
Appendix E (Continued)
☐Fleet management (ambulance services, med air operations; Search &
Rescue, mobile clinics);
☐Electrical and water installations for healthcare structures;
☐Medical disposal, waste management;
☐Other.
6. What do you think are the main challenges for your organization to provide
medical assistance in emergency? What should be done to improve the situation?
Explain
7. When it comes to the supply of healthcare goods in emergencies, what do you
consider are the main challenges?
☐Order management (too many items can be ordered, codification of
items, etc.)
☐Procurement (pharmaceutical purchase capacity, license-regulatory
issues, quality assurance, quality control, etc.)
☐Warehousing management (temperature/humidity constraints, expiring
product, cold chain, etc.)
☐Shipping (cold chain issue, etc.)
☐Importation and exportation (customs constraints, national legislations
and regulations, etc.)
☐Supply HR capacity – skills
☐Other
8. In emergency, what kind of international/regional supply chain structure your
organization usually relies on?
☐Internal integrated pharmaceutical supply center (in-house international
procurement unit, internal warehousing /shipping service, etc.);
☐Outsourced supply center (outsourcing part or all the international
supply chain to private sector or/and UNHRD);
☐Direct delivery from pharmaceutical companies;
49. 42
Appendix E (Continued)
☐Combined integrated and outsourced system;
☐Local procurement capacity only (no international supply center);
☐Other
Explain
9. At local level, what department is in charge of the medical supply chain in your
organization?
Logistics/supply Another department
Department (describe)
Medical ordering ☐ ☐ ______________
Pharmaceutical procurement ☐ ☐ ______________
Medical warehousing ☐ ☐ ______________
Medical shipping ☐ ☐ ______________
Custom clearance for medical items ☐ ☐ ______________
Maintenance of medical structure ☐ ☐ ______________
Maintenance of medical equipment ☐ ☐ ______________
Transport of patient ☐ ☐ ______________
Medical disposal ☐ ☐ ______________
Explain
10. Do you believe that logistics/supply chain challenges are the main obstacles
for the international humanitarian organizations to deploy medical assistance in
emergencies?
☐Yes ☐No
Explain
11. From your field experience, how do you believe the logistical challenges to
provide medical assistance in emergency are changing?
☐Increasing challenges
☐Stable challenges
☐Decreasing challenges
50. 43
Appendix E (Continued)
Explain
A. Base on your perception, how the medical programs have evolved or change
over the past 5 and 10 years?
Explain
5 years-
10 years-
B. How do you consider the number of international humanitarian organizations
responding to medical emergencies has changed over the past 5 years?
☐The number has increased
☐The number is stable and remains the same
☐The number has decreased
Explain
12. During the West Africa outbreak, was your organization engaged in treating
patients infected by the Ebola virus?
☐Yes ☐No
A. If yes, what would you do to improve the logistics/supply set-up for a future
Ebola response?
B. If no, why? (If the answer is because the INGO has never operated in Ebola
context, please explain.)
13. Some criticism inside and outside the humanitarian community has arisen
regarding the late medical response to the last year’s Ebola outbreak.
A. Comment on your own operation. What would you have done differently?
51. 44
Appendix E (Continued)
B. Have you implemented some changes in your supply chain caused by the Ebola
outbreak or are you planning to perform some changes? Specify the changes and
the expected results.
14. In case of future large-size humanitarian outbreak or earthquake without major
access/security constraints, how quickly can your organization deploy a ready-to-
use healthcare structure?
☐Cholera Treatment Unit (50 beds) Mini. Delays: days
☐Ebola Treatment Unit (50 beds) Mini. Delays: days
☐Field hospital with surgical capacity
(50 beds) Mini. Delays: days
☐Mobile clinics (10 teams) Mini. Delays: days
☐Maternity (10 beds) Mini. Delays: days
☐Therapeutic nutrition center Mini. Delays: days
☐Set-up for vaccination campaign
(300.000 target pop.) Mini. Delays: days
Comment
15. From your perspective, what are the three most effective international
humanitarian organizations when it comes to providing direct medical assistance
in emergencies? Could you explain why?
#1 Main strengths:
#2 Main strengths:
#3 Main strengths:
We sincerely appreciate your time and collaboration for the achievement of this
study. We will send you the transcripts of your answers shortly via email. Feel
free to correct and comment on them.
In case of any questions or comments please email Sara Guerrero to
sara.guerrero@gl.the-klu.org
52. 45
Appendix F. Completed questionnaire: IHO-2
Reference number: IHO-2
MEDICAL ASSISTANCE IN EMERGENCIES: LOGISTICAL
CHALLENGES. QUESTIONNAIRE.
1. Is your organization regularly involved in medical assistance during its
response to emergency situation?
☐Yes ☐No
A. If yes, what kind of medical activities your organization can provide
independently without relying on local/diaspora organizations or/and
affected government?
☐Hospital activities ☐Surgical care
☐Reproductive care ☐Primary healthcare
☐Mobile clinics ☐Mental Healthcare
☐Therapeutic nutrition center ☐Health promotion
☐Vaccination campaign during an outbreak (meningitis, polio, measles,
etc.)
☐Treatment of communicable diseases (cholera or Ebola centers, etc.)
☐Treatment of non-communicable disease (diabetes, cancer, etc.)
☐Other
B. If yes, what was the average budget your organization has dedicated to
medical assistance in 2014?
☐Less than 25% ☐50% to 70%
☐25% to 50% ☐More than 70%
C. If no, what are the main reasons for not deploying regular medical
assistance?
☐Other INGOs are already covering all medical needs.
☐Financial constraints (medical operation are too expensive, lack of
private funding, etc.)
☐Donors constraints (heavy reporting system, lack of funding for medical
stocks, etc.)
☐HR constraints (lack of available medical resources in the organizations,
high turn-over, etc.)
53. 46
Appendix F (Continued)
☐Logistics constraints (complex supply chains, heavy maintenance for
biomedical equipment, lack of central pharmaceutical procurement/stock
capacity, cold chain, expired drugs, etc.)
☐Security constraints (medical assistance often targeted)
☐Lack of WHO support (little technical support/donation in terms of
medical products and warehousing compare to other UN agencies)
☐Lack of medical inter-agency coordination (regular overlap or
uncovered gaps)
☐Others.
2. Has your organization managed emergency healthcare structures to admit sick,
wounded, or pregnant people during the following emergency situations?
Without partnership14
With partnership
(No use of 3rd party org., local/diaspora NGOs)
Pakistan earthquake – 2005 ☐ ☐
Myanmar cyclone – 2008 ☐ ☐
China earthquake – 2008 ☐ ☐
Gaza war – 2009 ☐ ☐
Zimbabwe cholera – 2010 ☐ ☐
Haiti earthquake – 2010 ☐ ☐
Haiti cholera outbreak – 2010/11 ☐ ☐
Libya conflict - 2011 ☐ ☐
Syria conflict – from 2011 ☐ ☐
CAR conflict – 2011 ☐ ☐
Philippines cyclone – 2013 ☐ ☐
West Africa Ebola outbreak – 2014 ☐ ☐
Gaza war- 2014 ☐ ☐
Nepal earthquake – 2015 ☐ ☐
Yemen conflict – 2015 ☐ ☐
14
Direct assistance with no use of third party organization, local/diaspora NGOs, governmental
structure, etc.
54. 47
Appendix F (Continued)
3. What are the main reasons your organization usually prefers to develop
partnership for medical response in emergency?
☐Local actors/public organizations know better how to respond
☐Partners have appropriate medical HR resources
☐Type of medication and protocols are more adapted to the patients
☐Faster implementation
☐Other
Explain
4. What kind of medical deployment does your organization usually develop in
emergency?
☐Direct assistance with permanent presence of international health
workers (no third party involved)
☐Remote control management (direct assistance but no permanent
presence of the international health workers)
☐Partnership (bilateral agreement with private/public healthcare structure,
field hospital, etc.)
☐Support (medical donation, financial support, medical training, etc.)
☐Other.
Explain
5. From your field experience, what are the main logistical challenges that the
international humanitarian organizations (INGOs, governmental organizations,
UN agencies) are facing when deploying medical programs in emergency
situation?
☒Supply chain (procurement, warehousing, shipping, etc.);
☒Healthcare structure / site management (design and maintenance of field
hospitals, cholera treatment center, vaccination site, etc.);
☒Equipment management (maintenance of bio-medical equipment,
diagnostic imaging equipment, etc.);
55. 48
Appendix F (Continued)
☐Fleet management (ambulance services, med air operations; Search &
Rescue, mobile clinics);
☐Electrical and water installations for healthcare structures;
☐Medical disposal, waste management;
☐Other.
6. What do you think are the main challenges for your organization to provide
medical assistance in emergency? What should be done to improve the situation?
Explain
7. When it comes to the supply of healthcare goods in emergencies, what do you
consider are the main challenges?
☒Order management (too many items can be ordered, codification of
items, etc.)
☒Procurement (pharmaceutical purchase capacity, license-regulatory
issues, quality assurance, quality control, etc.)
☐Warehousing management (temperature/humidity constraints, expiring
product, cold chain, etc.)
☐Shipping (cold chain issue, etc.)
☒Importation and exportation (customs constraints, national legislations
and regulations, etc.)
☐Supply HR capacity – skills
☒Other. Demand analysis, forecasting and inventory control- highly
variable and erratic demand.
8. In emergency, what kind of international/regional supply chain structure your
organization usually relies on?
☐Internal integrated pharmaceutical supply center (in-house international
procurement unit, internal warehousing /shipping service, etc.);
☐Outsourced supply center (outsourcing part or all the international
supply chain to private sector or/and UNHRD);
☐Direct delivery from pharmaceutical companies;
56. 49
Appendix F (Continued)
☐Combined integrated and outsourced system;
☐Local procurement capacity only (no international supply center);
☐Other
Explain
9. At local level, what department is in charge of the medical supply chain in your
organization?
Logistics/supply Another department
Department (describe)
Medical ordering ☐ ☐ ________________
Pharmaceutical procurement ☐ ☐ ________________
Medical warehousing ☐ ☐ ________________
Medical shipping ☐ ☐ ________________
Custom clearance for medical items ☐ ☐ ________________
Maintenance of medical structure ☐ ☐ ________________
Maintenance of medical equipment ☐ ☐ ________________
Transport of patient ☐ ☐ ________________
Medical disposal ☐ ☐ ________________
Explain
10. Do you believe that logistics/supply chain challenges are the main obstacles
for the international humanitarian organizations to deploy medical assistance in
emergencies?
☒Yes ☐No
Explain
Yes, if you want to provide high quality products to a high quality medical
program on time, then it is a challenge.
11. From your field experience, how do you believe the logistical challenges to
provide medical assistance in emergency are changing?
☒Increasing challenges
☐Stable challenges
☐Decreasing challenges
57. 50
Appendix F (Continued)
Explain
The logistical challenges are increasing due to national legislations and
regulations. However in terms of armed conflicts, access and security remain the
biggest constraints.
A. Base on your perception, how the medical programs have evolved or change
over the past 5 and 10 years?
Explain
5 years-
10 years-
B. How do you consider the number of international humanitarian organizations
responding to medical emergencies has changed over the past 5 years?
☐The number has increased
☐The number is stable and remains the same
☐The number has decreased
Explain
12. During the West Africa outbreak, was your organization engaged in treating
patients infected by the Ebola virus?
☐Yes ☐No
A. If yes, what would you do to improve the logistics/supply set-up for a future
Ebola response?
B. If no, why? (If the answer is because the INGO has never operated in Ebola
context, please explain.)
13. Some criticism inside and outside the humanitarian community has arisen
regarding the late medical response to the last year’s Ebola outbreak.
58. 51
Appendix F (Continued)
A. Comment on your own operation. What would you have done differently?
B. Have you implemented some changes in your supply chain caused by the
Ebola outbreak or are you planning to perform some changes? Specify the
changes and the expected results.
14. In case of future large-size humanitarian outbreak or earthquake without major
access/security constraints, how quickly can your organization deploy a ready-to-
use healthcare structure?
☐Cholera Treatment Unit (50 beds) Mini. Delays: days
☐Ebola Treatment Unit (50 beds) Mini. Delays: days
☐Field hospital with surgical capacity
(50 beds) Mini. Delays: days
☐Mobile clinics (10 teams) Mini. Delays: days
☐Maternity (10 beds) Mini. Delays: days
☐Therapeutic nutrition center Mini. Delays: days
☐Set-up for vaccination campaign
(300.000 target pop.) Mini. Delays: days
Comment
15. From your perspective, what are the three most effective international
humanitarian organizations when it comes to providing direct medical assistance
in emergencies? Could you explain why?
#1 MSF Main strengths: Emergency response capacity. Highly standardized
approach of medical kits system. Experience and capacity to work in conflict
areas.
#2 UNICEF Main strengths: Cold chain logistics on a large scale (supplying
entire countries).
#3 ICRC Main strengths: Highly standardized approach. Range of resources and
international standing. Experience and capacity to work in conflict areas.
We sincerely appreciate your time and collaboration for the achievement of this
study. We will send you the transcripts of your answers shortly via email. Feel
free to correct and comment on them.
In case of any questions or comments please email Sara Guerrero to
sara.guerrero@gl.the-klu.org
59. 52
Appendix G. Completed questionnaire: IHO-3
Reference number: IHO-3
MEDICAL ASSISTANCE IN EMERGENCIES: LOGISTICAL
CHALLENGES. QUESTIONNAIRE.
1. Is your organization regularly involved in medical assistance during its
response to emergency situation?
☐Yes ☒No
A. If yes, what kind of medical activities your organization can provide
independently without relying on local/diaspora organizations or/and
affected government?
☐Hospital activities ☐Surgical care
☐Reproductive care ☐Primary healthcare
☐Mobile clinics ☐Mental Healthcare
☐Therapeutic nutrition center ☐Health promotion
☐Vaccination campaign during an outbreak (meningitis, polio, measles,
etc.)
☐Treatment of communicable diseases (cholera or Ebola centers, etc.)
☐Treatment of non-communicable disease (diabetes, cancer, etc.)
☐Other
B. If yes, what was the average budget your organization has dedicated to
medical assistance in 2014?
☐Less than 25% ☐50% to 70%
☐25% to 50% ☐More than 70%
C. If no, what are the main reasons for not deploying regular medical
assistance?
☒Other INGOs are already covering all medical needs.
☐Financial constraints (medical operation are too expensive, lack of
private funding, etc.)
☐Donors constraints (heavy reporting system, lack of funding for medical
stocks, etc.)
☒HR constraints (lack of available medical resources in the organizations,
high turn-over, etc.)
60. 53
Appendix G (Continued)
☐Logistics constraints (complex supply chains, heavy maintenance for
biomedical equipment, lack of central pharmaceutical procurement/stock
capacity, cold chain, expired drugs, etc.)
☐Security constraints (medical assistance often targeted)
☐Lack of WHO support (little technical support/donation in terms of
medical products and warehousing compare to other UN agencies)
☐Lack of medical inter-agency coordination (regular overlap or
uncovered gaps)
☐Others. Our mission is not related to medical assistance. Indeed, the
organization has a partnership with other medical related organization. In
this way not just medical programs are supported but also other type of
assistance is provided by us.
2. Has your organization managed emergency healthcare structures to admit sick,
wounded, or pregnant people during the following emergency situations?
Without partnership15
With partnership
(No use of 3rd party org., local/diaspora NGOs)
Pakistan earthquake – 2005 ☐ ☐
Myanmar cyclone – 2008 ☐ ☐
China earthquake – 2008 ☐ ☐
Gaza war – 2009 ☐ ☐
Zimbabwe cholera – 2010 ☐ ☐
Haiti earthquake – 2010 ☐ ☐
Haiti cholera outbreak – 2010/11 ☐ ☐
Libya conflict - 2011 ☐ ☐
Syria conflict – from 2011 ☐ ☐
CAR conflict – 2011 ☐ ☐
Philippines cyclone – 2013 ☐ ☒
West Africa Ebola outbreak – 2014 ☐ ☒
Gaza war- 2014 ☐ ☒
Nepal earthquake – 2015 ☐ ☒
Yemen conflict – 2015 ☐ ☐
15
Direct assistance with no use of third party organization, local/diaspora NGOs, governmental
structure, etc.
61. 54
Appendix G (Continued)
3. What are the main reasons your organization usually prefers to develop
partnership for medical response in emergency?
☒Local actors/public organizations know better how to respond
☐Partners have appropriate medical HR resources
☐Type of medication and protocols are more adapted to the patients
☒Faster implementation
☒Other
Explain
In this way my organization can access to resources that my partner has and we
do not have. We work as a team with other organization and we believe in the
win-win situation for both organizations.
4. What kind of medical deployment does your organization usually develop in
emergency?
☐Direct assistance with permanent presence of international health
workers (no third party involved)
☐Remote control management (direct assistance but no permanent
presence of the international health workers)
☐Partnership (bilateral agreement with private/public healthcare structure,
field hospital, etc.)
☐Support (medical donation, financial support, medical training, etc.)
☒Other.
Explain
My organization supports or covers health related emergency contexts without
providing direct medical assistance. We provide trainings to the people, for
example immunization, as support to healthcare programs.
5. From your field experience, what are the main logistical challenges that the
international humanitarian organizations (INGOs, governmental organizations,
UN agencies) are facing when deploying medical programs in emergency
situation?
☒Supply chain (procurement, warehousing, shipping, etc.);
☐Healthcare structure / site management (design and maintenance of field
hospitals, cholera treatment center, vaccination site, etc.);
☒Equipment management (maintenance of bio-medical equipment,
diagnostic imaging equipment, etc.);
62. 55
Appendix G (Continued)
☐Fleet management (ambulance services, med air operations; Search &
Rescue, mobile clinics);
☒Electrical and water installations for healthcare structures;
☐Medical disposal, waste management;
☐Other.
6. What do you think are the main challenges for your organization to provide
medical assistance in emergency? What should be done to improve the situation?
Explain
Shortage of logisticians with medical experience, as we do not have an in-house
guidance in dealing with medical items. Also since we do not focus entirely in
medical assistance, there is a lack of experience in emergencies response,
specifically in medical programs.
7. When it comes to the supply of healthcare goods in emergencies, what do you
consider are the main challenges?
☒Order management (too many items can be ordered, codification of
items, etc.) The quantity of items to be ordered is determined by the
demand. If the demand is highly variable then it is impossible to be
accurate in the order.
☒Procurement (pharmaceutical purchase capacity, license-regulatory
issues, quality assurance, quality control, etc.)
☐Warehousing management (temperature/humidity constraints, expiring
product, cold chain, etc.)
☐Shipping (cold chain issue, etc.)
☒Importation and exportation (customs constraints, national legislations
and regulations, etc.)
☐Supply HR capacity – skills
☒Other. Governments’ policies- national customs and the allowance from
the Ministry of Health in terms of medicines and equipment. In some
cases, during the State of emergency the help from the government to
bring the medicines inside the country is very slow or not provided.
63. 56
Appendix G (Continued)
8. In emergency, what kind of international/regional supply chain structure your
organization usually relies on?
☐Internal integrated pharmaceutical supply center (in-house international
procurement unit, internal warehousing /shipping service, etc.);
☒Outsourced supply center (outsourcing part or all the international
supply chain to private sector or/and UNHRD);
☐Direct delivery from pharmaceutical companies;
☐Combined integrated and outsourced system;
☐Local procurement capacity only (no international supply center);
☒Other
Explain
Our relief items come from in-kind donations and purchased items from different
suppliers. The organization has also procured locally, however not always.
9. At local level, what department is in charge of the medical supply chain in your
organization?
Logistics/supply Another department
Department (describe)
Medical ordering ☒ ☐ Procurement officer
Pharmaceutical procurement ☒ ☐ Procurement officer
Medical warehousing ☒ ☐ Procurement officer
Medical shipping ☒ ☐ Procurement officer
Custom clearance for medical items ☐ ☐ N/A
Maintenance of medical structure ☐ ☐ N/A
Maintenance of medical equipment ☐ ☐ N/A
Transport of patient ☐ ☐ N/A
Medical disposal ☐ ☐ N/A
Explain
10. Do you believe that logistics/supply chain challenges are the main obstacles
for the international humanitarian organizations to deploy medical assistance in
emergencies?
☐Yes ☒No
64. 57
Appendix G (Continued)
Explain
Access to the people who need the assistance either in conflicts or in natural
disasters. In armed conflicts, the government or the power that is ruling can
prevent the access of humanitarian or medical assistance to the affected people.
In conflict situations, if injured people are treated they can become a threat to the
ones in powerful positions. This situation becomes a political problem rather than
a humanitarian emergency. In natural disaster, the access to affected people will
be difficult because roads are not accessible and sometimes you just reach the
people by helicopter. In some countries even if roads are not much affected, there
would remote areas difficult to reach.
11. From your field experience, how do you believe the logistical challenges to
provide medical assistance in emergency are changing?
☐Increasing challenges
☐Stable challenges
☒Decreasing challenges
Explain
The IHO are currently doing emergency preparedness and identifying the
potential challenges (access to the affected country, potential items to be sourced
locally). All operational and strategical aspects are considered during this
preparedness. Furthermore the United Nations Humanitarian Response Depot is
part of this process.
A. Base on your perception, how the medical programs have evolved or change
over the past 5 and 10 years?
Explain
5 years- It has evolved and cover more aspects of an emergency. The
manufacturers are aware of the growing opportunity in providing suppliers,
services and equipment for the humanitarian sector. There are, every year, some
commercial expositions of medical goods for the humanitarian sector in Brussels,
Washington D.C., Bangkok and Dubai. Also IFRC, UNICEF and MSF are
becoming humanitarian procurement centers and extending their supply chain
system to be available by other organizations. As we can procure from them, this
is a good opportunity for my organization since we just pay to use their system
and we do not have to re-invent the wheel. This means and evolution.
10 years-
B. How do you consider the number of international humanitarian organizations
responding to medical emergencies has changed over the past 5 years?
☒The number has increased
☐The number is stable and remains the same
☐The number has decreased