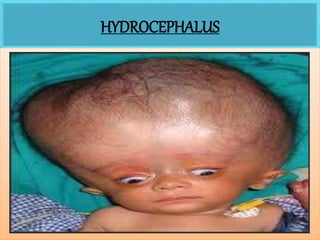
2. HYDROCEPHALUS
DEFINITION:
Hydrocephalus is defined as an imbalance between
the production and absorption of cerebrospinal
fluid.
It is characterized by abnormal increase in the
volume of cerebrospinal fluid within the intracranial
cavity resulting in enlargement of the infant's head.
2
3. INCIDENCE:
3-4 per 1000 live births.
NORMAL PATHWAY OF CSF:
CSF is produced by choroid plexus in lateral ventricles of brain
3rd ventricle
4th ventricle
Cisterna of subarachnoid space
CSF is finally reabsorbed into venous sinuses by Arachnoid villi
Through foramen of monro
Through Aqueduct of sylvius
Through foramen of Luschka & Megendie
Base of brain, into cortical sulci
3
5. CLASSIFICATION:
a) Non- communicating or obstructive hydrocephalus
b) Communicating or non- obstructive hydrocephalus
Non- communicating or obstructive hydrocephalus:
In this type, there is obstruction in the flow of CSF,
within the ventricles and subarachnoid space. This
occurs due to two reasons:
1) Congenital causes (Stenosis of aqueduct of sylvius,
meningomyelocele, Dandy- walker syndrome,
Arnold- chiari malformation)
5
6. 2) Acquired causes (Infection caused by rubella,
cytomegalovirus and toxoplasmosis, intracranial
hemorrhage, medulloblastoma,
craniopharyngioma, head injury)
Communicating or non- obstructive hydrocephalus:
The causes responsible for communicating
hydrocephalus are:
• Subarachnoid hemorrhage
• Meningitis
• Toxoplasmosis or cytomegalovirus infection
• Disease of connective tissue like Hurler’s syndrome
6
7. CLINICAL FEATURES:
Clinical features in infants:
There is accumulation of CSF in ventricles
Sutures become widely separated
Delayed closure of anterior fontanele
Tense bulging fontanele
“Cracked pot” sound is heared on percussion
(Macewen’s sign)
Sun setting sign (visible sclera above the iris)
7
9. Clinical features in older children:
Headache on awakening
Nausea and vomiting
Irritability and high pitch cry
Lethargy
Apathy
Confusion
Impaired judgment and reasoning skills
9
11. MANAGEMENT:
Management of hydrocephalus is directed towards:
a) Reducing intracranial pressure
b) Prevention and management of complication
c) Managing problems caused by the problem
Medical management include use of diuretic
(Acetazolamide & Frusemide), these medicine
provide temporary relief, but the main
management is surgery i.e Insertion of Shunt.
11
12. Four types of shunts are available:
1) Ventriculoperitoneal shunt
2) Ventriculoatrial shunt (from ventricles to left
atrium)
3) Ventriculopleural shunt (from ventricles to the
pleural cavity)
4) Ventriculoureteric shunt (from ventricles to the
ureter)
12
14. NURSING MANAGEMENT:
Pre- operative care:
a) Measure the head circumference daily
b) Palpate the fontanele for evidence of increased
intracranial pressure.
c) Assess the pupillary response and level of
consiousness.
d) Monitor vital signs regularly.
e) Provide calm and quiet environment.
f) Prevent the child from nosocomial infection.
g) Change the infant position frequently.
14
15. Post- operative care:
a) Place the infant in flat position to prevent rapid
CSF drainage.
b) Check vital signs every 15—30 minutes in
immediate post- operative period.
c) Assess the neurological status.
d) Assess the head circumference regularly.
e) Oral rehydration must be started after the bowel
sound reappears.
f) Check dressings for any drainage.
g) Teach parents about care of the child at home.
15