2. ● Posterior malleolar fractures are observed in approximately 14%–44% of all ankle
fractures.
● The most common type of posterior malleolar fracture involves the posterior
tubercle, resulting in an avulsion of the posterior inferior tibiofibular ligament
(PITFL) following a rotational ankle injury
● Posterior malleolus fractures associated with more severe injury and worse
outcome so proper treatments need to be understood (Tejwani J Trauma 2010)
According to AO, a posterior fragment comprising more than 25% of the intra-articular
surface needs to be fixated
However, recent literature seems to suggest otherwise...
Overview
3. Does size affect functional outcomes?
Comparing functional outcome (AOFAS, AAOS, and Weber scores) with
respect to size of the posterior fragment
● Langenhuijsen et al. (2002), n=57, retrospective cohort
● Xu et al. (2012), n=102, retrospective cohort
● Drijfhout et al. (2015), n=131, retrospective cohort
● Evers et al. (2015), n=42, retrospective cohort
Could NOT find a significant difference in function outcome with respect to
different posterior fragment sizes.
4. Does size affect development of arthritis?
● Xu et al. (2012), n=102, retrospective cohort
● Drijfhout et al. (2015), n=131, retrospective cohort
● Verhage et al. (2019), n=169, retrospective cohort
Found NO relation between fragment size and development of osteoarthritis.
6. Intra-articular step-off
Xu et al., Drijfhout et al., and Verhage et al. found that persisting postoperative
intra-articular step-off of the posterior fragment (> 1 mm) was a significant risk
factor for the development of osteoarthritis and worse functional outcome.
Advised to anatomically reduce all posterior fragments with intra-articular
involvement
Fixation is needed to prevent redislocation and thus a persistent postoperative
step-off
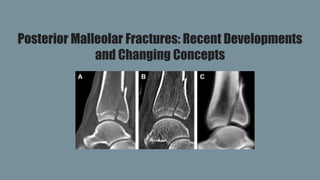
7. Anatomic Location
Bartonicek and Rammelt Three-Dimensional Computed Tomography Classification (2015)
Type 1: Extraincisural fragment
Type 2: Posterolateral fragment
Type 3: Posteromedial, two part fragment
Type 4: Large, posterolateral triangular fragment
8.
9. Treatment recommendations
Type 1 (Extraincisural) : non-operative
Type 2 (Posterolateral): ORIF
Type 3 (Two-part): ORIF
Type 4 (Large triangular): ORIF
10. Why fixating posterior malleolar fractures beneficial
Restoration of articular congruence -> posterior ankle stability
Restoration of the integrity of the fibular notch -> reduction of the distal fibula
● Miller et al. (2010) : With PM reconstruction, the distal fibula is reduced more
accurately into the restored fibular notch
Restoration of the competence of the PITFL -> syndesmotic stability
12. Posterior Malleolus versus Transyndesmal Fixation
As PM fractures should be considered bony avulsions of the PITFL, anatomic reduction of the PM is hypothesized to restore
syndesmotic stability.
Gardner et al. (2006)
70% stiffness of the distal tibiofibular articulation was restored by reducing and stabilizing the posterior malleolus compared
to 40% through the use of a syndesmotic screw.
Miller et al. (2010)
Suggested that fixation of posterior malleolus fracture is more likely to restore stability to the syndesmosis compared to
trans-syndesmotic fixation alone.
Baumbach et al. (2019)
Study demonstrated a 60% decrease in trans-syndesmotic fixation following ORIF of the PM fragment
ORIF of the posterior malleolar fracture, no matter what size, can provide adequate
stabilization of the syndesmosis through the PITFL.
13. What type of fixation for posterior malleolar
fractures?
14. “A to P” Screw vs Posterolateral Plate Fixation
CRIF
-Percutaneous anterior to posterior screw
fixation after closed reduction through
ligamentotaxis
ORIF
-Direct open reduction and fixation via
posterolateral approach with plate fixation
16. Fixation of the posterior malleolus via an open posterolateral approach is superior
to percutaneous anterior-to-posterior fixation
- Radiographically superior with decreased incidence of step-off
- Functionally superior with better AOFAS scores
17. In conclusion
Fixate posterior malleolar fractures regardless of size
Posterior malleolus fixation is superior to transsyndesmotic screws
Fixation of the posterior malleolus via an open posterolateral approach is superior
to percutaneous anterior-to-posterior fixation
18. References
Tejwani NC. The effect of posterior malleolus fracture on outcome after unstable ankle fracture. J Trauma 2010; 69:666-9.
Miller AN. Posterior malleolar stabilization of syndesmotic injury is the equivalent to screw fixation. CORR 2010;268:1129-35.
Gardner MJ. Fixation of posterior malleolar fractures provides greater syndesmotic stability. CORR 2006;447:165-171.
Macko VW. The Joint-Contact Area of the Ankle. JBJS 1991; 73:347-351.
Raasch WG. Assessment of the posterior malleolus as a restraint to posterior subluxation of the ankle. JBJS 1992; 74 (8): 1201 -1206.
Jaskulka RA. Fractures of the posterior tibial margin: their role in the prognosis of malleolar fractures. J Trauma 1989;29(11):1565–70.
Langenhuijsen JF. Results of ankle fractures with involvement of the posterior tibial margin. J Trauma. 2002 Jul;53(1):55-60.
Gardner MJ. Surgeon practices regarding operative treatment of posterior malleolus fractures. FAI 2011; 32(4):385–93.
Xu HL, Li X, Zhang DY, et al. A retrospective study of posterior malleolus fractures. Int Orthop. 2012;36(9):1929–1936.
Baumbach SF, Herterich V, Damblemont A, Hieber F, Bocker W, Polzer, H. Open Reduction and Internal Fixation of the Posterior Malleolus Fragment Frequently
Restores Syndesmotic Stability. Injury. 2019 Feb;(50)2:564–570.
Verhage, SM, Krijnen P, Schipper IB, & Hoogendoorn JM. Perisistent postoperative step-off of the posterior malleolus leads to higher incidence of posttraumatic
osteoarthritis in trimalleolar fractures. Arch Orthop Trauma Surg. 2019 Mar; 139(3):323–329.
19. Ferries JS. Plain radiographic interpretation in trimalleolar ankle fractures poorly assesses posterior fragment size. JOT 1994;8(4):328–31.
Ebraheim NA. External rotation-lateral view of the ankle in the assessment of the posterior malleolus. FAI 1999; 20(6):379–83.
Black EM. Role of preoperative computed tomography scans in operative planning for malleolar ankle fractures. FAI 2013 May;34(5):697-704.
Haraguchi N. Pathoanatomy of posterior malleolar fractures of the ankle. JBJS 2006;88(5):1085–92.
O’Connor TJ. “A to P” screw versus posterolateral plate for posterior malleolus fixation in trimalleolar ankle fractures. JOT 2015;29(4):e151–6.
Evers J. Size matters: the influence of the posterior fragment on patient outcomes in trimalleolar ankle fractures. Injury 2015; 46(Suppl 4):S109–13.
Drijfhout van Hooff CC. Influence of fragment size and postoperative joint congruency on long-term outcome of posterior malleolar fractures. FAI
2015;36(6):673–8.
Donken CC. The outcome at 20 years of conservatively managed isolated posterior malleolar fractures of the ankle: a case series. JBJS Br 2011;93-
B:1621-5.
Bartonicek J, Rammelt S, Tucek M. Posterior malleolar fractures: changing concepts and recent developments. Foot Ankle Clin. 2017;22(1):125–145.
doi: 10.1016/j.fcl.2016.09.009.
Shi H, Xiong J, Chen Y, et al. Comparison of the direct and indirect reduction techniques during the surgical management of posterior malleolar
fractures. BMC Musculoskelet Disord. 2017;14(1):109.
Huber M, Stutz PM, Gerber C. Open reduction and internal fixation of the posterior malleolus with a posterior antiglide using a posterolateral
approach, a preliminary report. Foot Ankle Surg. 1996;2(2):95–103.
Editor's Notes
Review of current litetarure
Verhage 2018
Functional outcome assessed with AOFAS, AAOS, and Weber scores
Large cohorts that had a mean follow up time of 6 years