5.wound healing
•
1 like•117 views

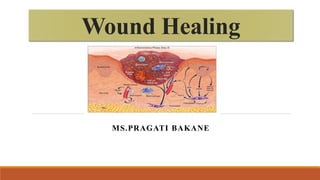
Wound healing is a complex, but well-coordinated process, which attempts to restore the normal structure and function of the injured tissue/organ. A wound is a disruption in the continuity and regulatory process of tissue cell During healing, a complex cascade of cellular events occurs to achieve resurfacing, reconstitution, and restoration of tensile strength of injured tissue.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to 5.wound healing
Similar to 5.wound healing (20)
Recently uploaded
Recently uploaded (20)
5.wound healing
- 2. INTRODUCTION Wound healing is a complex, but well-coordinated process, which attempts to restore the normal structure and function of the injured tissue/organ. A wound is a disruption in the continuity and regulatory process of tissue cell During healing, a complex cascade of cellular events occurs to achieve resurfacing, reconstitution, and restoration of tensile strength of injured tissue.
- 3. DEFINITION Wound healing refers to the body’s replacement of destroyed tissue by living tissue. Can be achieved by 2 processes: tissue regeneration &scar formation. A dynamic balance between these 2 is different in different tissues.
- 4. TYPES AND PROCESS OF WOUND HEALING Healing by Primary union or First intention:- Wounds with opposed edges, which are clean, uninfected and do not involve tissue loss heal by primary union or first intention. The narrow incision causes bleeding into the defect, which gets sealed with clotted blood containing fibrin and blood cells. The surface of clot dries up to form the scab which cover the wound.
- 5. The sequential events that occur in healing by primary union are as follows: Initial hemorrhage: - the incised wound is filled with blood, which then clots and seal the wound. Acute inflammatory response: - occurs within 24 hrs. Of the injury and is characterized by the appearance of neutrophils at the margins of the clot, which are replaced by macrophages by 3rd day. Epithelial changes: - within 24 hrs. Of the injury, mitosis begins to appear in the basal cells of the injured epithelium and the wound is covered by epithelium within 24-48 hrs.
- 6. Granulation tissue formation:-by the 3rd day, granulation tissue begins to form within the wound and fills the entire wound cavity by the 5th day. There is marked neovascularization of the wound with epithelial proliferation. Organization: - the occurs marked fibroblastic proliferation by the 2nd week leading to continuous collagen deposition. By the 4 weeks, the scar tissue is replaced with adult-type I collagen, which is responsible for the wound strength. This is followed by intact epithelium by the 8-10 weeks.
- 7. Healing by Secondary union or second intention:- Wounds, which are wide open due to extensive loss of cells and tissues, heal by secondary intention. Examples of injuries, which heal by secondary intention are infarcts, abscesses and large gaping wounds. The healing is slow and results in a prominent scar as compared to primary union. The sequences of events are as follows:
- 8. Hemorrhage: Wound space is filled with blood and fibrin clot, which dries up and temporarily fills the wound space. Inflammatory response: The inflammatory response is much more intense and pronounced in gaping wounds as the defect is large and there is more necrotic tissue and debris in such wounds.
- 9. Granulation tissue: The amount of granulation tissue formed in healing by secondary intention is much more as compared to healing by primary union. Granulation tissue is formed by the proliferation of fibroblasts and neovascularization from adjoining viable elements. The newly formed granulation tissue is fragile, granular and deep red. On maturation, scar became pale and white due to an increase in collagen and decrease in vascularity.
- 10. Epithelial changes: Proliferating epithelial cells do not cover the surface fully until granulation tissue from base has started filling the wound space. Wound contraction: This is the main differentiating feature between healing by primary and secondary intention. In large gaping wounds, which heal by secondary intention, there is marked wound contracture due to the action of myofibroblasts.
- 11. Infections: Open wounds are more prone to get infected and this delays the process of healing due to release of bacterial toxins that provoke necrosis, suppuration and inflammation.
- 12. FACTORS AFFECTING WOUND HEALING Various physiological and mechanical factors may impair the healing response, resulting in a chronic wound that fails to proceed through the usual stepwise progression of healing and repair. Factors, which affect wound healing are broadly divided into two categories:- Local factors System factors
- 13. LOCAL FACTORS Infection: It is the most important local cause for delay in healing. Size or extent of wound: Small wound due to surgical incision or other injuries heal quickly with less scar formation than large wound. Apposition of edges of wound: The wound edges, which are appropriately approximated heals faster than which do not have adequate apposition of the edges.
- 14. Blood supply: Wound in areas with good blood supply such as the face, heals faster than those with poor blood supply, such as the foot. For example, varicose veins of the legs decrease the venous drainage and can cause non healing of ulcers. Mobility, if the wounded part: Excess movement of wounded area can result in delayed healing. Presence of foreign body in the wound: Unnecessary sutures, fragments of steel, glass, bone or any other foreign particle can delay healing.
- 15. Cellular hypoxia: The cellular hypoxemia decreases the healing process. Exposure to ionizing radiation: The ionizing radiations decrease healing process.
- 16. SYSTEMIC FACTORS Age: Wound healing is rapid in young compared to older individuals. Nutritional status: Protein deficiency, vitamin C deficiency, inhibits collagen synthesis and diminished healing process. Metabolic status: Diabetes mellitus (DM) is associated with delayed healing. Immune status: Poor immunity of an individual contributes to the increased susceptibility for infections and delayed wound healing.
- 17. Systemic circulation: Inadequate blood supply such as atherosclerosis or venous abnormalities like varicose veins that leads to the delayed wound healing. Hormones: Steroids inhibits collagen synthesis, thereby impair wound healing.
- 18. COMPLICATIONS OF WOUND HEALING Some of the common complications of the wound healing are as follows: Secondary infections, which may lead to delayed wound healing and chronic nonhealing ulcers. Deficient scar formation, which may lead to ulceration or wound dehiscence. Excessive formation of granulation tissue and fibrous scar leading to raised swollen scars referred to as keloids.
- 19. Formation of contractures: Minimal wound contracture is a normal part of wound healing. However, in cases of healing by secondary intention, sometimes there is exaggerated contracture of wounds leading to functional deformities and unpleasant scar formation. This is a major complication of wounds, which involve large surface areas of the body e.g. extensive burns.
- 20. REFERENCE S. Lewis, M. Heitkemper, S. Dirksen, P. Obrien and L. Bucher (2007) Medical Surgical Nursing; Assessment and Management of Clinical problems (7th edition). Suresh Sharma “Textbook of pharmacology, pathology and genetics for nurses” volume 1 jaypee publication. K.Swaminathan “Textbook of pathology and genetics for nurses”2nd edition Jaypee publication.