
Recommended
More Related Content
What's hot
What's hot (20)
Similar to ORGANOPHOSPHATE POISONING
Similar to ORGANOPHOSPHATE POISONING (20)
Recently uploaded
Recently uploaded (20)
ORGANOPHOSPHATE POISONING
- 2. INTRODUCTION Organophosphate compounds are widely used in agricultural sector as PESTICIDES & as chemical war fare. Case fatality following deliberate ingestion is high (15–30%). Easily accessible, hence associated with self poisoning 200,000 /500,00 mortality associated self-poisoning with pesticides in rural Asia. 50-70 % in hospital based study. 15-30% in India Suicidal rate with OPC 20.6- 56.3%. Organophosphates are among the most popular and most widely used insecticides in India.
- 3. • Organophosphates are anti-esterase insecticides, and exert their acute effects by causing overstimulation at cholinergic nerve terminals. This process occurs in both insects and humans.
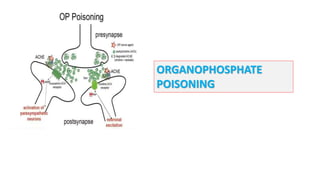
- 4. Normally, acetylcholinesterase catalyzes the degradation of the neurotransmitter acetylcholine in the synapse (yellow panel). Organophosphate pesticides phosphorylate acetylcholine, thereby reducing the ability of the enzyme to break down the neurotransmitter (red panel) Accumulation of (ACH) in cholinergic synapses Overstimulation of (Ach) receptors in postsynaptic neuron
- 5. This produces an accumulation of acetylcholine in the central and peripheral nervous systems, resulting in an acute cholinergic syndrome via continuous neurotransmission. The clinical onset of cholinergic over-stimulation can vary from almost instantaneous to several hours after exposure.
- 6. Mechanism of toxicity OP compounds inactivate acetylcholinesterase (AChE), resulting in the accumulation of acetylcholine (ACh) in cholinergic synapses. After the process (termed ‘ageing’) has taken place, new enzyme needs to be synthesised before function can be restored. The rate of ‘ageing’ is an important determinant of toxicity and is more rapid with dimethyl (3.7 hrs) than diethyl (31 hrs) compounds and especially rapid after exposure to nerve agents (soman in particular), which cause ‘ageing’ within minutes.
- 7. Irreversibly bind to serine-OH group at active site of acetylcholinesterase (AChE) & establish covalent bond (phosphorylation) AGING: loss of alkyl group + strengthening of covalent bond Phosphorylated AChE is very stable Inhibition of enzyme activity accumulation of ACh in the synapse and NMJ Overstimulation of cholinergic receptors
- 8. Toxicokinetics • ■ Organophosphates can be absorbed by any route including Transdermal, Transconjunctival, Inhalational, across the GI and GU mucosa, and through direct injection. • ■ Manifestations usually begin within a few minutes to few hours, but may be delayed upto 12 hours or more in the case of certain compounds (e.g. fenthion, parathion).
- 9. Clinical features • OP poisoning causes an Acute cholinergic phase, Intermediate syndrome, Organophosphate-induced delayed polyneuropathy (OPIDN). • The onset, severity and duration of poisoning depend on the route of exposure and agent involved.
- 10. Acute cholinergic syndrome • This usually starts within a few minutes of exposure and nicotinic or muscarinic features may be present.( within first 24 hrs)
- 11. • Garlic-like odor • Vomiting and profuse Diarrhoea are typical following ingestion. • Bronchoconstriction, Bronchorrhoea and Salivation may cause severe Respiratory compromise. • Excess Sweating and Miosis are characteristic and the presence of muscular fasciculation strongly suggests the diagnosis, although this feature is often absent, even in serious poisoning. • Subsequently, Generalized flaccid paralysis may develop and affect Respiratory and Ocular muscles, resulting in Respiratory failure. • Ataxia, Coma, Convulsions, Cardiac repolarization abnormalities and torsades de pointes may occur.
- 13. Cholinergic features in poisoning Muscarinic Nicotinic Respiratory Bronchorrhoea, bronchoconstriction Reduced ventilation Circulation Bradycardia, hypotension, Tachycardia, hypertension Higher mental function Anxiety, delirium, psychosis Muscle - Fasciculation, paralysis Temperature Fever - Eyes Diplopia, miosis, lacrimation Mydriasis Abdomen Vomiting, profuse diarrhoea - Mouth Salivation - Skin Sweating - Complications Coma, seizures, respiratory depression
- 15. Intermediate syndrome • About 20% of patients with OP poisoning develop weakness that spreads rapidly from the ocular muscles to those of the head and neck, proximal limbs and the muscles of respiration, resulting in ventilatory failure. • Onset : 24-96 hrs after poisoning, after the cholinergic phase settles. Mechanism: Excess Ach at NMJ causes down regulation of nicotinic receptors and muscles affected.
- 16. Intermediate syndrome: Features: Characterized by proximal neck muscles leading to respiratory distress and failure without muscarinic signs, without intervention, cyanosis ,coma and death occurs rapidly. Duration: Lasts for few days to about 3 weeks. There is no specific treatment and supportive care is needed, including maintenance of airway and ventilation.
- 17. OP-Induced Delayed Polyneuropathy (OPIDN) Onset: Occurs 2-4 weeks after exposure & associated with demyelination of axons. Mechanism: Due to degeneration of long myelinated nerve fibers. Pure motor or sensor-motor. Not caused by cholinesterase inhibition but rather by neuropathy target esterase (NTE) inhibition. Features: Characterized by cramps in the legs , numbness and paresthesia in the distal upper and lower limbs , shuffling gait , foot and wrist drop. Other features: wasting, DTR reduced/absent, pyramidal tract signs absent.
- 18. Involves distal muscles with relative sparing of neck muscles, cranial nerves, & proximal muscles. • Delayed mixed sensorimotor peripheral neuropathies. • C/o: Symmetric, peripheral neuropathies. Motor > sensory • Ataxia, gait disturbances. • • Fate – self-resolution / persistent deficits. • Recovery is incomplete.
- 19. • Diagnosis of organophosphate poisoning Clinical diagnosis : severity of organophosphorus poisoning (Dreisbach`s) Grade Symptoms Mild Nausea. Moderate Lacrimation, salivation , miosis , fasciculation. Severe Incontinence, apneic spells ,ARDS , Areflexia seizures, coma.
- 20. Laboratory: Red cell cholinesterase. Plasma cholinesterase (Pseudo, Butyryl(Bu)). ECG : The most common Ecg abnormality was prolonged QTc and sinus tachycardia. ABG : Hypoxemia.
- 21. Patients at risk • • Poisoning due to OPs with delayed metabolism. • • Severe poisoning. • • Elevated muscle enzymes. • • Delayed or inadequate oxime therapy.
- 22. Management of OP Poisoning Hospitalization/ ICU • 1. Initial stabilization. • 2. Reduction of exposure. • 3. Administration of specific antidote. • 4. Supportive treatment. Initial Stabilization of the patient. • Clear airway and • Adequate ventilation because the patient with acute organophosphate poisoning (ACC) commonly presents with respiratory distress. • Oxygen- Circulation- iv access- intubation. AIM: A systolic BP 80mmhg and urine output >30ml/hr.
- 23. • Decontamination • • Dermal spills—wash pesticide spills from the patient with soap and water and remove and discard contaminated clothes, shoes and any other material made from leather. • • Gastric lavage —consider for presentations within 1 or 2 hours, when the airway is protected. A single aspiration of the gastric contents may be as useful as lavage. • • Activated charcoal —50 g may be given orally or nasogastrically to patients who are cooperative or intubated, particularly if they are admitted within one or two hours or have severe toxicity.
- 24. • Antidotes in the treatment of OP poisoning. • • Atropine- Reverses the muscarinic features. • • Oxime- Reactivate cholinesterase and reverses the nicotinic features.
- 25. Suggested symptom based treatment recommendations for organophosphorus poisoning Sign or symptom Recommended therapy Excessive salivation ,lacrimation, nausea and vomiting, diarrhea Atropine, Glycopyrrolate Bronchorrhoea, Bronchospasm Atropine, Ipratropium, Glycopyrrolate Hypotension Fluids, Atropine, Vasopressors, Inotropes Bradycardia Atropine, Glycopyrrolate Eye pain Mydriatics, Cycloplegics Muscle weakness Oximes Respiratory failure Intubation and Ventilation, Oximes Seizures Benzodiazepines
- 26. Atropine • • Initial dose: 1.8-3 mg IV every 5-10min until atropinisation. • • Continuous infusion (8mg atropine in 100ml NS) at rate of 0.02- 0.08mg/kg/hr (0.25-1.0 ml/kg/hr) with additional 1-5mg bolus. • • May require about 40-1500mg/day. • • For at least 5-7days. • • Watch out for OVER ATROPINIZATION. Early use of sufficient doses of atropine is potentially life- saving in patients with severe toxicity.
- 27. Target end points for atropine therapy • • Clear chest on auscultation with no wheeze. • • Heart rate> 80/min. • • Pupils no longer pin point (does not imply that pupils must be dilated). • • Dry axilla. • • Systolic BP > 80 mm Hg. • Dilated pupils is not a reliable sign of initial atropinisation or end point for atropine therapy.
- 28. Pralidoxime (2-PAM) • An oxime that reactivates phosphorylated cholinesterase. • Effects: skeletal-neuromuscular junctions (counteracts weakness, fasciculation and respiratory depression). • Administration within 48 hours of poison ingestion. PAM must be given by infusion. Go slow ,both for bolus and maintenance. A fast infusion can cause vomiting ,hypertension, cardiac arrhythmias or cardiac arrest.
- 29. Bolus dose: 30mg/kg (1-2gm) in 100ML of NS over 30min (at a rate not exceeding 200mg/min), repeat in 1 hour if muscle weakness persist, then at 8- 12 hours interval if cholinergic signs recur. Maintenance dose :continuous infusion og 8-12mg/kg per hour. • Severe case: IV infusion 500mg/hr (max 12gm in 24hours). • Started after maximal atropinisation. In severe poisoning requiring atropine, an oxime such as pralidoxime chloride or obidoxime is generally recommended
- 30. BENZODIAZEPINES: Agitation and seizure : Diazepam 10mg slow IV push ,repeated as necessary . Upto 30 to 40 mg diazepam per 24 hrs can be given. Ventilator: Ventilatory support should be started before the patients develops resoiratory failure.
- 31. Other therapies Magnesium sulfate –blocks ligand-gated calciumchannels ,resulting in reduced acetylcholine release from presynaptic terminals, thus improving function at neuromuscular junction, and reduced CNS over stimulation mediated via NMDA receptors activation. Sodium bicarbonate in place of oximes. Alpha2- adrenergic receptors agonist clonidine also reduces acetylcholine synthesis and release from presynaptic terminal. Hemodialysis and Hemofiltration.
- 32. Treatment of IMS • • Mainly supportive treatment. • • Complete recovery in 4-18 days if adequate Ventilator support is Provided. • • Oximes – Preventive.
- 34. • Exam Important • Muscarinic signs of OPC poisoning can be remembered as SLUDGE- DUMBEELLS: Salivation, Lacrimation, Urination, Defecation, Gastric upset, Emesis, etc.. • Delayed onset polyneuropathy after organophosphorous poisoning is seen after 2-4 weeks. • Fatality rate of organophosphorous poisoning in India is 15-30%. • In organophosphorous compound poisoning, organophosphorous compound is a Phosphorylated enzyme irreversibly inhibit cholinesterase. • Most specific test for organophosphorous poisoning is Plasma cholinestrase level. • Organophosphate inhibits Esteratic site of AchEs. • Antidote for organophosphorous poisoning is Atropine
- 36. CHRONIC POISONING: • It usually occurs as an occupational hazard in agriculturists, especially those who are engaged in pesticide spraying of crops. • Route of exposure is usually inhalation or contamination of skin.
- 37. CHRONIC POISONING… • The following features— Polyneuropathy: paraesthesias, muscle cramps, weakness, gait disorders. CNS Effects : drowsiness, confusion, irritability, anxiety. Sheep Farmer’s Disease : psychiatric manifestations encountered in sheep farmers involved in long-term sheep-dip operations. Organophosphate poisoning has been associated with a variety of subacute or delayed onset chronic neurological, neurobehavioural, or psychiatric syndromes.
- 39. CARBAMATE POISONING Medicinal forms include Physostigmine , Pyridostigmine and Neostigmine . Cholinesterase inhibitors that are STRUCTURALLY RELATED TO ORGANOPHOSPHATES. Transiently and reversibly inhibit cholinesterase (<6hrs). Regeneration of enzyme occurs within minutes to hours, therefore aging dose not occur.
- 40. CARBAMATE POISONING… Symptoms of intoxication are similar to organophosphates , but are of shorter duration. Carbamates do not effectively penetrate into CNS , so LESS CENTRAL TOXICITY and no seizures. Atropine therapy usually not needed for longer than 6-12 hours. Avoid PRALIDOXIME (2-PAM): Since irreversible binding dose not occur, it is not occur, it is not needed, and potentially can worsen some carbamate poisonings.
- 43. ORGANOCHLORINE: Acute organochlorine poisoning Prodromal symptoms: tremor, ataxia , myoclonus , dizziness, confusion, paresthesia of mouth , nausea, vomiting. Typical presentation : STATUS EPILEPTICUS , followed by respiratory failure ,cardiac arrhythmias , rhabdomyolysis and acute renal failure. Treatment :- Control seizure- the same ways as status epilepticus. - Benzodiazepines, Phenobarbital, Phenytoin. Prevent complications
- 44. Sub acute organochlorine poisoning Hyperexcitability stage : Tachycardia , Tremor, Hyper reflexia. Treatment: Symptomatic treatment - Anxiolytic. Enhance elimination – cholestyramine.
- 45. Chronic organochlorine poisoning: Organochlorine insecticides interfere with endocrine and reproductive systems. Individuals who work with the insecticides show low sperm count and motility , infertility and abortion. The insecticides can be carcinogenic to animals.
- 47. • Signs of organophosphorous poisoning are all EXCEPT: A Bradycardia B Salivation C Miosis D Bronchodilatation
- 48. • Delayed onset polyneuropathy after organophosphorous poisoning is seen after a period of A 1-2 weeks B 2-4 weeks C 4-6 weeks D 6-8 weeks
- 49. Most specific test for organophosphorous poisoning is: A RBC cholinesterase level B Plasma cholinestrase level C RBC uroporphyrin level D Measurment of serum level of organophosphorous
- 50. • Asthma like symptoms is seen in … poisoning? • What is the case fatality rate of organophosphorous poisoning in India? • A 20 yrs aged patient, presents in coma with pin point pupils and fasciculations but no fever. Most probable diagnosis ? • Antidote for organophosphorous poisoning is?
- 51. • Best indicator for beneficial effect of atropine in a patient with organophosphorous poisoning ?