Unleashing the Potential of Perioperative Immunotherapy in Resectable NSCLC: Leveraging Science, Enhancing Collaboration, and Improving Outcomes With Neoadjuvant and/or Adjuvant Checkpoint Inhibition
•
0 likes•8 views

Chair, Jessica Donington, MD, David H. Harpole Jr., MD, and Jonathan D. Spicer, MD, PhD, FRCSC, prepared useful Practice Aids pertaining to NSCLC for this CME/MOC/AAPA activity titled “Unleashing the Potential of Perioperative Immunotherapy in Resectable NSCLC: Leveraging Science, Enhancing Collaboration, and Improving Outcomes With Neoadjuvant and/or Adjuvant Checkpoint Inhibition.” For the full presentation, downloadable Practice Aids, and complete CME/MOC/AAPA information, and to apply for credit, please visit us at https://bit.ly/3OtwGAh. CME/MOC/AAPA credit will be available until October 22, 2024.

Recommended
Recommended
More Related Content
Similar to Unleashing the Potential of Perioperative Immunotherapy in Resectable NSCLC: Leveraging Science, Enhancing Collaboration, and Improving Outcomes With Neoadjuvant and/or Adjuvant Checkpoint Inhibition
Similar to Unleashing the Potential of Perioperative Immunotherapy in Resectable NSCLC: Leveraging Science, Enhancing Collaboration, and Improving Outcomes With Neoadjuvant and/or Adjuvant Checkpoint Inhibition (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Unleashing the Potential of Perioperative Immunotherapy in Resectable NSCLC: Leveraging Science, Enhancing Collaboration, and Improving Outcomes With Neoadjuvant and/or Adjuvant Checkpoint Inhibition
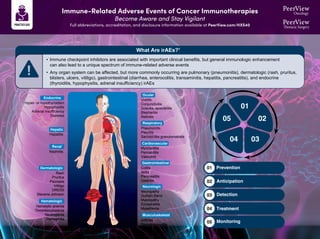
- 1. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant Full abbreviations, accreditation, and disclosure information available at PeerView.com/HXS40 What Are irAEs?1 • Immune checkpoint inhibitors are associated with important clinical benefits, but general immunologic enhancement can also lead to a unique spectrum of immune-related adverse events • Any organ system can be affected, but more commonly occurring are pulmonary (pneumonitis), dermatologic (rash, pruritus, blisters, ulcers, vitiligo), gastrointestinal (diarrhea, enterocolitis, transaminitis, hepatitis, pancreatitis), and endocrine (thyroiditis, hypophysitis, adrenal insufficiency) irAEs Endocrine Hyper- or hypothyroidism Hypophysitis Adrenal insufficiency Diabetes Hepatic Hepatitis Renal Nephritis Dermatologic Rash Pruritus Psoriasis Vitiligo DRESS Stevens-Johnson Hematologic Hemolytic anemia Thrombocytopenia Neutropenia Hemophilia Ocular Uveitis Conjunctivitis Scleritis, episcleritis Blepharitis Retinitis Respiratory Pneumonitis Pleuritis Sarcoid-like granulomatosis Cardiovascular Myocarditis Pericarditis Vasculitis Gastrointestinal Colitis Ileitis Pancreatitis Gastritis Neurologic Neuropathy Guillain Barŕe Myelopathy Encephalitis Myasthenia Musculoskeletal Arthritis Dermatomyositis 01 Prevention 02 Anticipation 03 Detection 04 Treatment 05 Monitoring 01 02 03 04 05
- 2. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant Full abbreviations, accreditation, and disclosure information available at PeerView.com/HXS40 Guidance for Surgeons: Suspect, Detect, and Refer for Treatment2,3 • irAEs frequently occur in the perioperative setting, either before or after surgical intervention • irAEs occurring during neoadjuvant immunotherapy are generally manageable and in most cases should not exclude patients from surgery • The onus is on the surgeon to have a high degree of suspicion for potential toxicities in patients treated with immunotherapy • Vague symptoms should not be dismissed, because nonspecific ailments can be indicative of severe toxicity – Rheumatologic toxicities and endocrinopathies are some of the most difficult to recognize, given their relatively nonspecific presentation » For example, fatigue, poor energy, and low mood could represent hypophysitis or adrenal insufficiency – Other toxicities can be essentially asymptomatic » For example, renal and hepatic toxicity are generally only detected on routine labs – Pneumonitis is another relevant irAE requiring awareness by surgeons, as severe pneumonitis could potentially exclude patients from operative therapy, but significant pneumonitis has been rare in trials to date • A comprehensive workup for irAEs, with a thorough history specifically targeted to potential irAEs, should be conducted • Coordinate and collaborate with oncologists and other multidisciplinary experts to optimally diagnose and manage irAEs in patients who have received/are receiving perioperative immunotherapy • The National Comprehensive Cancer Network (NCCN) and American Society of Clinical Oncology (ASCO) have issued guidelines for recognition and management of immune-related adverse events
- 3. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant Full abbreviations, accreditation, and disclosure information available at PeerView.com/HXS40 General Recommendations for Treating irAEs4-7 Increasing intensity of treatment required Grade 2 Grade 1 Grade 3 Grade 4 Moderate Mild Severe Very severe Symptomatic & supportive therapy Stop treatment Oral steroids Intravenous steroids. ------------> • Referral to specialist • Strong immune suppressive treatment Increasing grade of irAE intravenous steroids Steroids (PO/IV): 1-2 mg/kg/d prednisone or equivalent, slowly taper over 4-6 weeks For some AEs, treatment can be restarted after resolution (eg, rash); generally, ICI can be continued with endocrinopathies once managed Managed in outpatient/ community setting Generally requires hospital admission
- 4. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant Full abbreviations, accreditation, and disclosure information available at PeerView.com/HXS40 Hold immunotherapy and reassess in 1-2 weeks Pulse oximetry rest and ambulation Consider chest imaging with CT (with contrast preferred) Repeat in 3-4 weeks Moderate (grade 2): 25%-50% lung involved Severe (grade 3-4) Grade 3: all lobes of lung or >50% of lung parenchyma; limited ADLs, oxygen requirement Grade 4: life threatening Hold immunotherapy Infectious workup (nasal swab, sputum, blood) Consider bronchoscopy and BAL Chest imaging with CT contrast Repeat in 3-4 weeks Consider empiric antibiotics Refractory: methylprednisolone 1-2 mg/m2 /day; if no response in 3-4 days, treat as grade 3 Permanently discontinue immunotherapy and move to inpatient care Infectious workup (nasal swab, sputum, blood) Pulmonary and infectious disease consultation Bronchoscopy with BAL Empiric antibiotics Methylprednisolone 1-2 mg/m2 /day; when grade 1, taper over 6 weeks Refractory: infliximab, mycophenolate, or IVIG How Should Pulmonary irAEs Be Diagnosed and Managed?4,8 Pneumonitis: focal or diffuse inflammation of the lung parenchyma (typically identified on CT imaging) Diagnostic work-up: CXR, CT, pulse oximetry; for grade ≥2, may include infectious work-up Mild (grade 1): <25% lung involved Additional considerations • GI and pneumocystis prophylaxis may be offered to patients on prolonged steroid use (>12 weeks) • Consider calcium and vitamin D supplementation with prolonged steroid use • Bronchoscopy and biopsy; if clinical picture is consistent with pneumonitis, no need for biopsy Supportive care: smoking cessation and vaccinations (influenza, pneumococcal)
- 5. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant Full abbreviations, accreditation, and disclosure information available at PeerView.com/HXS40 1. Champiat S et al. Ann Oncol. 2016;27:559-574. 2. Helmink BA et al. Ann Surg Oncol. 2020;27:1533-1545. 3. Stiles BM et al. J Thorac Cardiovasc Surg. 2020;160:1376-1382. 4. Brahmer JR et al. J Clin Oncol. 2018;36:1714-1786. 5. https://www.esmo.org/content/ download/124130/2352601/1/ESMO-Patient-Guide-on-Immunotherapy-Side-Effects.pdf. 6. https://www.nccn.org/professionals/physician_gls/pdf/immunotherapy.pdf. 7. Puzanov I et al. J Immunother Cancer. 2017;5:95. 8. Provided courtesy of Marianne Davies, DNP, ACNP, AOCNP, FAAN, 2021; adapted from AIM with Immunotherapy, NCCN, and CTCAE. 9. https://ascopubs.org/doi/full/10.1200/JCO.21.01440. 10. https://www.esmo.org/content/download/124130/2352601/1/ESMO-Patient-Guide-on-Immunotherapy-Side-Effects.pdf. 11. https://www.nccn.org/professionals/physician_gls/pdf/immunotherapy.pdf. 12. https://www.sitcancer.org/research/cancer-immunotherapy-guidelines/irae/immune-checkpoint-inhibitor-related-adverse-events. Additional Guideline Recommendations for Treating irAEs9-12
- 6. The AATS 2023 Expert Consensus Recommendations for the Management of Patients With Early-Stage NSCLC1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/HXS40 Levels of Evidence2 C-EO (Expert Opinion) C-LD (Limited Data) B-NR (Nonrandomized) B-R (Randomized) A • Randomized or nonrandomized observational or registry studies with limitations of design or execution; meta- analyses of such studies • Physiological or mechanistic studies in human subjects • Consensus of expert opinion based on clinical experience • Moderate-quality evidence from ≥1 well-designed, well- executed nonrandomized studies, observational studies, or registry studies; meta- analyses of such studies • Moderate-quality evidence from ≥1 randomized controlled trials • Meta-analyses of moderate- quality randomized controlled trials • High-quality evidence from >1 randomized controlled trial • Meta-analyses of high-quality randomized controlled trials • ≥1 randomized controlled trials corroborated by high-quality registry studies Class of Recommendation2 III: Harm (Strong) III: No Benefit (Moderate) IIb (Weak) IIa (Moderate) I (Strong) Benefit < Risk Benefit = Risk Benefit ≥ Risk Benefit >> Risk Benefit >>> Risk Recommendations for Optimal Diagnosis and Staging Level of Evidence Class of Recommendation Recommendations B-R I B-R I A I Appropriate staging of patients with newly diagnosed lung cancer should include CT and PET imaging. In addition, brain imaging and invasive mediastinal staging should be performed where clinically indicated. Thorough lymph node assessment is imperative for accurate pathologic staging and optimal oncologic outcomes. Intraoperative lymphadenectomy should include at least 3 mediastinal stations and 1 hilar nodal station. Lobectomy remains the SOC resection strategy for operable patients. However, anatomic sublobar resection may be acceptable for tumors determined to be low risk for nodal involvement based on size or radiographic/histopathologic features. It may also be an acceptable approach for patients who are high risk for lobectomy. A I Early initiation of molecular sequencing and other biomarker analyses is recommended to select optimal preoperative and postoperative treatment regimens in locally advanced patients.
- 7. The AATS 2023 Expert Consensus Recommendations for the Management of Patients With Early-Stage NSCLC1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/HXS40 Levels of Evidence2 C-EO (Expert Opinion) C-LD (Limited Data) B-NR (Nonrandomized) B-R (Randomized) A • Randomized or nonrandomized observational or registry studies with limitations of design or execution; meta- analyses of such studies • Physiological or mechanistic studies in human subjects • Consensus of expert opinion based on clinical experience • Moderate-quality evidence from ≥1 well-designed, well- executed nonrandomized studies, observational studies, or registry studies; meta- analyses of such studies • Moderate-quality evidence from ≥1 randomized controlled trials • Meta-analyses of moderate- quality randomized controlled trials • High-quality evidence from >1 randomized controlled trial • Meta-analyses of high-quality randomized controlled trials • ≥1 randomized controlled trials corroborated by high-quality registry studies Class of Recommendation2 III: Harm (Strong) III: No Benefit (Moderate) IIb (Weak) IIa (Moderate) I (Strong) Benefit < Risk Benefit = Risk Benefit ≥ Risk Benefit >> Risk Benefit >>> Risk Recommendations for Neoadjuvant Therapy Level of Evidence Class of Recommendation Recommendations B-NR IIA For medically operable patients with oncologically resectable stage III NSCLC with N2 disease for whom surgery is planned, preoperative systemic therapy without radiotherapy is recommended. For those patients with superior sulcus tumors and no evidence of N2 disease, neoadjuvant concurrent chemoradiotherapy is preferred. B-R I Platinum-based chemotherapy doublet in combination with immunotherapy is the preferred neoadjuvant regimen for medically operable patients with resectable stage II and III NSCLC, lacking EGFR and ALK alterations, regardless of PD-L1 status. Neoadjuvant platinum-based chemotherapy doublet alone is recommended for patients with a contraindication to immunotherapy. C-EO IIA For eligible patients with resectable and medically operable stage II and III NSCLC without EGFR or ALK alterations, neoadjuvant platinum-based chemotherapy with immunotherapy is preferred over adjuvant therapy.
- 8. The AATS 2023 Expert Consensus Recommendations for the Management of Patients With Early-Stage NSCLC1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/HXS40 Levels of Evidence2 C-EO (Expert Opinion) C-LD (Limited Data) B-NR (Nonrandomized) B-R (Randomized) A • Randomized or nonrandomized observational or registry studies with limitations of design or execution; meta- analyses of such studies • Physiological or mechanistic studies in human subjects • Consensus of expert opinion based on clinical experience • Moderate-quality evidence from ≥1 well-designed, well- executed nonrandomized studies, observational studies, or registry studies; meta- analyses of such studies • Moderate-quality evidence from ≥1 randomized controlled trials • Meta-analyses of moderate- quality randomized controlled trials • High-quality evidence from >1 randomized controlled trial • Meta-analyses of high-quality randomized controlled trials • ≥1 randomized controlled trials corroborated by high-quality registry studies Class of Recommendation2 III: Harm (Strong) III: No Benefit (Moderate) IIb (Weak) IIa (Moderate) I (Strong) Benefit < Risk Benefit = Risk Benefit ≥ Risk Benefit >> Risk Benefit >>> Risk Recommendations for Adjuvant Therapy Level of Evidence Class of Recommendation Recommendations A I All patients with NSCLC with pathologic stage IB-III (eighth edition) should be referred to medical oncology for discussion of adjuvant systemic therapy after lung resection. C-LD IIa/IIb For resected patients with NSCLC without pathologic nodal disease, high-risk features (lymphovascular invasion, visceral pleural invasion, larger tumor size, positive margin, inadequate nodal sampling) should prompt consideration of medical oncology referral and adjuvant therapy. A I All resected stage IB-IIIA lung adenocarcinomas should undergo comprehensive testing for molecular alterations, and all patients with resected stage II-IIIA should undergo tumor PD-L1 staining. A I All resected stage II-IIIA lung squamous cell carcinomas should undergo PD-L1 staining. B-R I All patients with resected IB-IIIA lung adenocarcinoma and with EGFR mutations should be referred to medical oncology for discussion of adjuvant osimertinib, whether or not adjuvant cytotoxic chemotherapy is considered possible/desired. B-R I All patients with resected II-IIIA NSCLC patients with PD-L1 staining ≥1% should be referred to medical oncology for consideration of adjuvant immunotherapy after adjuvant chemotherapy. A I Postoperative radiation therapy to the mediastinum should not be routinely given to resected patients with NSCLC with incidental/unforeseen (ie, “surprise”) pathologic N2 disease. 1. Kidane B et al. J Thorac Cardiovasc Surg. 2023;166:637-654. 2. Bakaeen FG et al. J Thorac Cardiovasc Surg. 2017;153:999-1005.
- 9. Strategies for implementation of immunotherapy in resectable NSCLC Postoperative setting Preoperative setting Perioperative setting Biological Rationale for Immune Checkpoint Inhibitor (ICI)–Based Treatment of Patients With Resectable NSCLC Postoperative ICIs Postoperative chemotherapy (optional) Cancer cell T cell Postoperative ICIs Postoperative chemotherapy (optional) Cancer cell T cell Postoperative ICIs Postoperative chemotherapy (optional) Cancer cell T cell PD-L1 PD-1 TCR MHC II Cancer cell T cell Postoperative ICIs Postoperative chemotherapy (optional) T cell repertoire A broad spectrum of activated T cells eliminate micrometastatic disease T cell repertoire A broad spectrum of activated T cells eliminate micrometastatic disease Cancer cells T cell Activated T cells eliminate micrometastatic disease CD8+ T cell DC Macrophage NK cell • The presence of the whole tumor enables triggering of a broader repertoire of antitumor CD8+ T cells • Preoperative tumor shrinkage facilitates complete resection CD8+ T cell DC Macrophage NK cell • The presence of the whole tumor enables triggering of a broader repertoire of antitumor CD8+ T cells • Preoperative tumor shrinkage facilitates complete resection Prostaglandins Catecholamines TNF IL-6/IL-8/IL-10 TAM Treg cell MDSC Activation and expansion Postsurgical stress Surgical resection Neoadjuvant setting Adjuvant setting Perioperative Immunotherapy for Resectable NSCLC: Biologic Rationale, Outcomes, and Key Clinical Trials1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/HXS40
- 10. Perioperative Immunotherapy for Resectable NSCLC: Biologic Rationale, Outcomes, and Key Clinical Trials1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/HXS40 Main Outcomes of Clinical Trials Evaluating Neoadjuvant Immunotherapy or Chemoimmunotherapy Strategies ICIs Without Chemotherapy ICIs With Chemotherapy Nivolumab CheckMate -159 0 25 50 75 100 95 45 10 10 7 7 14 0 0 21 88 97 93 7 11 4 89 5 19 10 86 15 30 10 90 6 31 13 100 10 27 13 95 2730 17 95 0 50 25 92 19 38 29 81 22 22 9 96 20 41 11 93 19 9 7 LCMC3 PRINCEPS IONESCO Gao et al. NEOSTAR NEOpredict-Lung EAST ENERGY Pembrolizumab + ramucirumab NeoCOAST Atezolizumab Durvalumab Sintilimab Nivolumab Nivolumab + ipilimumab Durvalumab Nivolumab Nivolumab + relatlimab Durvalumab + oleclumab Durvalumab + monalizumab Durvalumab + danvatirsen Surgery ORR MPR pCR Nivolumab + chemotherapy NADIM 0 25 50 75 100 89 83 63 76 4643 20 54 58 62 18 82 NR 33 17 81 NR 49 25 82 NR 30 18 82 63 57 33 87 54 37 24 83 74 52 36 91 NADIM II CheckMate -816 Shu et al. Neotorch AEGEAN KEYNOTE-671 Pembrolizumab + chemotherapy SAKK 16/14 Zhang et al. Nivolumab + chemotherapy Nivolumab + chemotherapy Atezolizumab + chemotherapy Sintilimab + chemotherapy Toripalimab + chemotherapy Chemotherapy → durvalumab Durvalumab + chemotherapy Surgery ORR MPR pCR
- 11. Perioperative Immunotherapy for Resectable NSCLC: Biologic Rationale, Outcomes, and Key Clinical Trials1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/HXS40 Ongoing Clinical Trials Evaluating ICIs in Resectable NSCLC Endpoints Clinical Trial Evaluating Perioperative Immunotherapy Phase • pCR • Safety NeoCOAST-2 II • EFS CheckMate -77T III • EFS IMpower030 • EFS • MPR RATIONALE-315 • pCR NCT05157776 R Chemotherapy + durvalumab + oleclumab (4 cycles) Chemotherapy + durvalumab + monalizumab (4 cycles) Durvalumab + oleclumab (1 year) Durvalumab + monalizumab (1 year) Surgery R Chemotherapy + nivolumab Chemotherapy Q3W (3 cycles) Nivolumab (1 year) Placebo (1 year) Surgery R Chemotherapy + atezolizumab Chemotherapy + placebo Q3W (4 cycles) Atezolizumab (1 year) Placebo (1 year) Surgery R Chemotherapy + tislelizumab Chemotherapy + placebo Q3W (3-4 cycles) Tislelizumab (8 cycles) Placebo (12 cycles) Surgery R Chemotherapy + sintilimab Q3W (2 cycles) Chemotherapy + sintilimab Q3W (4 cycles) Chemotherapy + sintilimab Q3W (2 cycles; optional) Placebo (39 weeks) Surgery
- 12. Perioperative Immunotherapy for Resectable NSCLC: Biologic Rationale, Outcomes, and Key Clinical Trials1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/HXS40 Ongoing Clinical Trials Evaluating ICIs in Resectable NSCLC Endpoints Clinical Trial Evaluating Adjuvant ICIs • DFS PEARLS • DFS in PD-L1+ and overall populations BR31 • DFS • OS ANVIL • DFS in PD-L1+, stage II-IIIA and ITT populations IMpower010 • Investigator-assessed DFS CANOPY-Aa R Pembrolizumab (1 year) Placebo R Durvalumab (1 year) Placebo R Nivolumab (1 year) Observaation R Atezolizumab (1 year) Best supportive care R Canakinumab (1 year) Placebo a Patients had stage II-IIIB disease according to the eighth edition of the TNM classification. 1. Mountzios G et al. Nat Rev Clin Oncol. 2023;20:664-677.