Emerging Biomarkers, New Targets, and Rational Combinations: Are We on the Verge of the Next Generation of Immuno-Oncology?
•
1 like•788 views

Naiyer Rizvi, MD, Omid Hamid, MD, Solange Peters, MD, PhD, Thomas Powles, MBBS, MRCP, MD, and Nadeem Riaz, MD, MSc, prepared useful Practice Aids pertaining to immuno-oncology for this CME activity titled "Emerging Biomarkers, New Targets, and Rational Combinations: Are We on the Verge of the Next Generation of Immuno-Oncology?" For the full presentation, monograph, complete CME information, and to apply for credit, please visit us at http://bit.ly/2H2s92Y. CME credit will be available until June 17, 2019.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Emerging Biomarkers, New Targets, and Rational Combinations: Are We on the Verge of the Next Generation of Immuno-Oncology?
Similar to Emerging Biomarkers, New Targets, and Rational Combinations: Are We on the Verge of the Next Generation of Immuno-Oncology? (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Emerging Biomarkers, New Targets, and Rational Combinations: Are We on the Verge of the Next Generation of Immuno-Oncology?
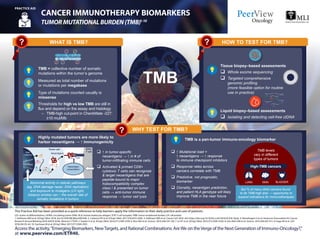
- 1. CD: cluster of differentiation; ctDNA: circulating tumor DNA; HLA: human leukocyte antigen; TCR: T-cell receptor; TMB: tumor mutational burden; UV: ultraviolet. 1. Hellmann MD et al. N Engl J Med. 2018. doi:10.1056/NEJMoa1801946. 2. Carbone DP et al. N Engl J Med. 2017:376;2415-2426. 3. Hellmann MD et al. Cancer Cell. 2018. doi: https://doi.org/10.1016/j.ccell.2018.03.018. Epub. 4. Ramalingam S et al. American Association for Cancer Research Annual Meeting 2018 (AACR 2018). Abstract CT078. 5. Snyder A et al. N Engl J Med. 2014;371:2189-2199. 6. Rizvi NA et al. Science. 2015;348:124-128. 7. Le DT et al. N Engl J Med. 2015;372:2509-2520. 8. Van Allen EM et al. Science. 2015;350:207-211. 9. Hugo W et al. Cell. 2016;165:35-44. 10. Yarchoan M et al. N Engl J Med. 2017;377:2500-2501. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. CANCER IMMUNOTHERAPY BIOMARKERS TUMORMUTATIONALBURDEN(TMB)1-10 PRACTICE AID Access the activity,“Emerging Biomarkers, NewTargets, and Rational Combinations: AreWe on theVerge of the Next Generation of Immuno-Oncology?,” at www.peerview.com/ETR40. WHAT IS TMB? TMB = collective number of somatic mutations within the tumor’s genome Highly mutated tumors are more likely to harbor neoantigens → ↑ immunogenicity TMB HOW TO TEST FOR TMB? WHY TEST FOR TMB? Tissue biopsy–based assessments q Whole exome sequencing q Targeted comprehensive genomic profiling (more feasible option for routine use in practice) Liquid biopsy–based assessments q Isolating and detecting cell-free ctDNA q ↑ in tumor-specific neoantigens → ↑ in # of tumor-infiltrating immune cells q Activated & primed CD8+ cytotoxic T cells can recognize & target neoantigens that are peptide-bound to major histocompatibility complex class I & presented on tumor cells → anti-tumor immune response → tumor cell lysis q ↑ Mutational load = ↑ neoantigens → ↑ response to immune checkpoint inhibitors q Response rates across cancers correlate with TMB q Predictive, not prognostic, biomarker q Clonality, neoantigen prediction, and patient HLA genotype will likely improve TMB in the near future Abnormal activity in cellular pathways (eg, DNA damage repair, DNA replication) and exposure to mutagens (UV light, tobacco smoke) can ↑ the overall rate of somatic mutations in tumors Neoantigens TCR Neoantigen presentation Tumor cell Killer T cellDNA mutations HLA 1 2 3 4 5 6 78 9 10 11 12 13 14 15 16 17 18 19 20 21 22 TMB is a pan-tumor immuno-oncology biomarker Measured as total number of mutations or mutations per megabase Type of mutations counted usually is missense Thresholds for high vs low TMB are still in flux and depend on the assay and histology – TMB-high cut-point in CheckMate -227: ≥10 mut/Mb TMB levels vary in different types of tumors LUNG SKIN BLADDER High-TMB cancers But % of many other cancers found to be TMB-high also → opportunity to expand indications for immunotherapies
- 2. CRC: colorectal cancer; dMMR: mismatch repair deficient; EXO: exonuclease; IHC: immunohistochemistry; MLH1: mutL homolog 1; MLH3: mutL homolog 3; MMR: mismatch repair; MSH2: mutS homolog 2; MSH3: mutS homolog 3; MSH6: mutS homolog 6; MSI: microsatellite instability; MSI-H: microsatellite instability high; NGS: next-generation sequencing; PCR: polymerase chain reaction; POL: polymerase. 1. Vilar E, Gruber SB. Nat Rev Clin Oncol. 2010;7:153-162. 2. Hause RJ et al. Nat Med. 2016;22:1-9. 3. Bogaert J, Prenen H. Ann Gastroenterol. 2014;27:9-14. 4. Giannakis M et al. Cell Rep. 2016;15:857-865. 5. McGranahan N et al. Science. 2016;351:1463-1469. 6. https://www.fda.gov/Drugs/ InformationOnDrugs/ApprovedDrugs/ucm569366.htm. Accessed April 5, 2018. 7. https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm560040.htm. Accessed April 5, 2018. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. Access the activity,“Emerging Biomarkers, NewTargets, and Rational Combinations: AreWe on theVerge of the Next Generation of Immuno-Oncology?,” at www.peerview.com/ETR40. CANCER IMMUNOTHERAPY BIOMARKERS MICROSATELLITEINSTABILITY(MSI)/MISMATCHREPAIR(MMR)1-7 PRACTICE AID WHAT IS MSI/MMR? Microsatellite instability high or deficient mismatch repair (MSI-H/dMMR) status MSI-H/dMMR tumors → ↑ neoantigens → ↑ immunogenicity HOW TO TEST FOR MSI/MMR? WHY TEST FOR MSI/MMR? MSI status q Polymerase chain reaction (PCR) Indicators of genomic instability q MSI-H: Change in # of nucleotide repeats in DNA sequences → different number of repeats than in inherited DNA q dMMR: Loss of function in the MMR pathway, a key DNA repair system MMR status q Immunohistochemistry (IHC) MSI-H/dMMR status predicts benefit from immune checkpoint inhibitors; FDA-approved options: Alternative method q Next-generation sequencing (NGS) q Patients ≥12 yrs with MSI-H or dMMR metastatic CRC that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan Nivolumab q Unresectable/metastatic MSI-H or dMMR solid tumors that have progressed following prior treatment and who have no satisfactory alternative treatment options q MSI-H or dMMR CRC that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan Adult and pediatric patients with: EXO 3’ → 5’ EXO proofreading 3’ → 5’ EXO proofreading SlippageMispair POL error (10-4 -10-5 ) Error extension (slow) MMR MMR POL Apoptosis DNA damage PMS2MLH1 MSH2 MutSα MSH6 PMS2MLH1 MSH2 MutSα MSH6 MLH3MLH1 MSH2 MutSβ or or MSH3 MSI-H/dMMR tumors have high mutational burden Pembrolizumab MSI MMR ↑ neoantigens → ↑ T-cell activation & immune cell infiltration of tumor microenvironment
- 3. IHC: immunohistochemistry; PD-1: programmed cell death protein 1; PD-L1: programmed death ligand 1; PD-L2: programmed death-ligand 2. 1. Gatalica Z et al. Cancer Epidemiol Biomarkers Prev. 2014;23:2965-2970. 2. Taube JM et al. Clin Cancer Res. 2014;20:5064-5074. 3. Kerr KM et al. J Thorac Oncol. 2015;10:985-989. 4. Topalian SL et al. Nat Rev Cancer. 2016;16:275-287. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. Access the activity,“Emerging Biomarkers, NewTargets, and Rational Combinations: AreWe on theVerge of the Next Generation of Immuno-Oncology?,” at www.peerview.com/ETR40. CANCER IMMUNOTHERAPY BIOMARKERS PROGRAMMEDDEATH-LIGAND1(PD-L1)EXPRESSION1-4 PRACTICE AID WHAT IS PD-L1? PD-L1: a ligand for the immune checkpoint receptor programmed cell death protein 1 (PD-1) expressed on the surface of cytotoxic T cells HOW TO TEST FOR PD-L1? WHAT ARE THE PITFALLS OF PD-L1 TESTING? PD-L1 expression can be measured by an immunohistochemistry (IHC) assay and detected on tumor and immune cells Between 0% and 100% of tumor cells within a sample can express PD-L1 q Focal PD-L1 expression in some tumors may be missed in small biopsy specimens q PD-L1 expression among multiple tumor lesions from individual patients can vary over time and by anatomical site q PD-L1 expression in tumor biopsies collected months or years earlier might not accurately reflect PD-L1 status at the time of treatment initiation q Antibodies used for PD-L1 detection have different affinities and specificities q PD-L1 epitopes detected by some antibodies can be unstable with prolonged specimen fixation or inadequate tissue handling q PD-L1 protein expression can be membranous and/or cytoplasmic, but only membranous PD-L1 is functionally relevant when in contact with PD-1+ T cells q PD-L1 can be expressed by multiple cell types within the tumor microenvironment, which makes scoring and interpretation challenging DRUG DIAGNOSTIC Complementary: PD-L1 IHC 28-8 pharmDx test PD-L1 expression Nivolumab Companion: PD-L1 IHC 22C3 pharmDx test Pembrolizumab Complementary: Ventana PD-L1 SP142 assay Atezolizumab Complementary: Ventana PD-L1 SP263 assay Durvalumab PD-L1 PD-L2 PD-1 T cell Tumor cell