Downloaded 12 times











































































![108
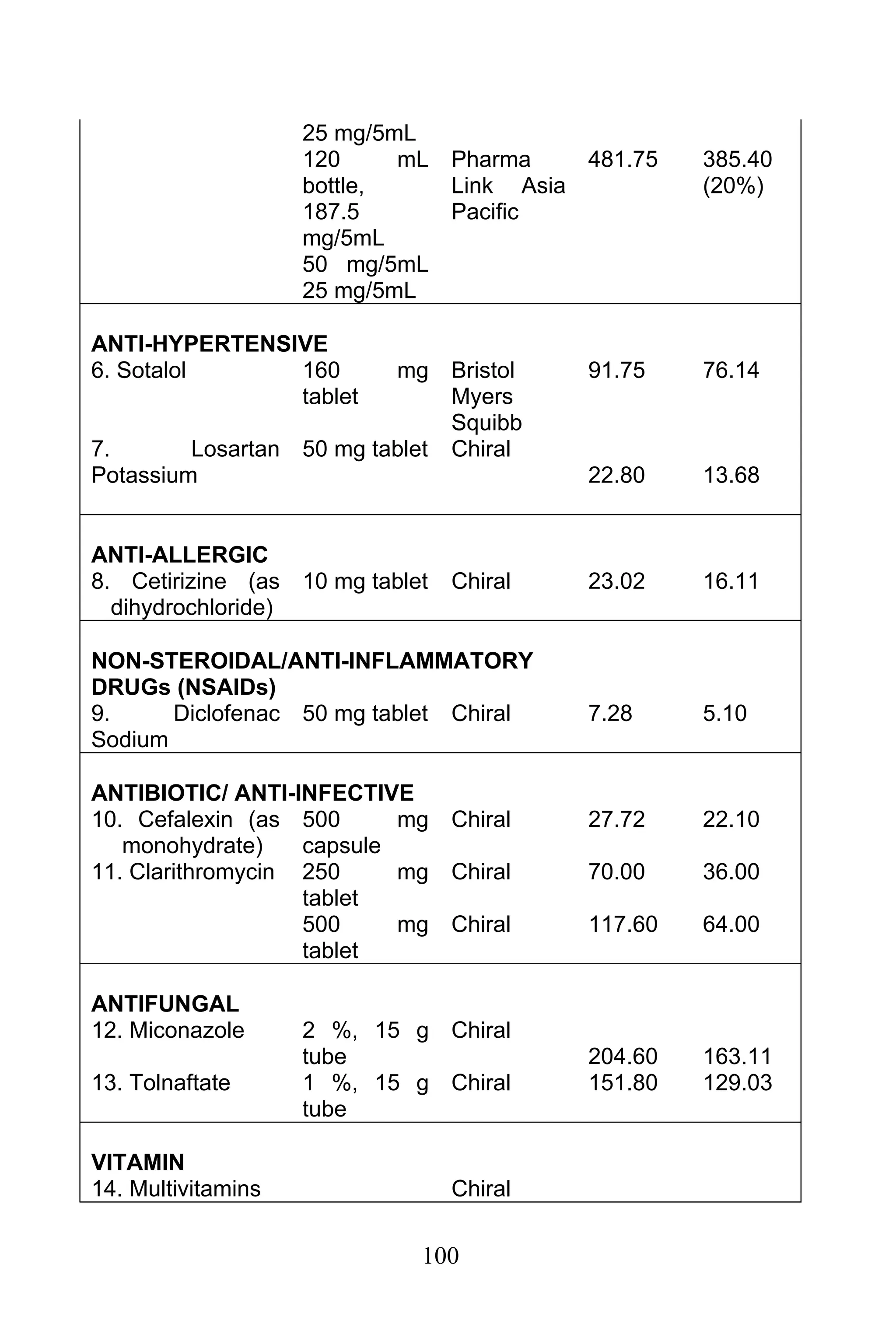
(12) Private hospitals to raise fees to recoup losses from drug
price cut
By Sheila Crisostomo
(The Philippine Star) Updated September 20, 2009 12:00 AM
MANILA, Philippines - Private hospitals will increase their
administrative fees to recoup the losses incurred from the medicine
price cuts.
Private Hospitals Association of the Philippines (PHAP) president Dr.
Rustico Jimenez said this was the consensus of their members
during a meeting yesterday in Clark Freeport, Pampanga where they
discussed how they could sustain their operations despite the losses.
Jimenez said hospitals would charge a fee every time nurses
administer medicine or injection to a patient….
http://www.philstar.com/Article.aspx?articleId=506876&publicationSu
bCategoryId=63
(13) Cheaper drugs law change eyed
Written by Fernan Marasigan & Estrella Torres / Reporters
MONDAY, 21 SEPTEMBER 2009 22:05
BRITISH pharmaceutical companies are appealing for the
amendment of the cheaper-medicines law that significantly reduced
prices of drugs for chronic and life-threatening diseases, according to
Britain’s envoy to the Philippines.
This, as a bill to complement the cheaper-medicines law has been
filed in the House of Representatives, seeking to keep drug costs
down by requiring drug manufacturers to submit annual reports of
their marketing expenses to the secretary of health.
“Lawmakers in the country are bewildered [that] certain medicines
sold in the Philippines by a multinational pharmaceutical company are
priced higher than other countries like India and Pakistan,” said
Lakas-Kampi-CMD Rep. Diosdado “Dato” Arroyo of Camarines Sur,
author of the bill….
http://www.businessmirror.com.ph/home/top-news/16323-cheaper-
drugs-law-change-eyed.html](https://image.slidesharecdn.com/healthchoicesandresponsibilities-130908111852-/75/Health-Choices-and-Responsibilities-120-2048.jpg)
![109
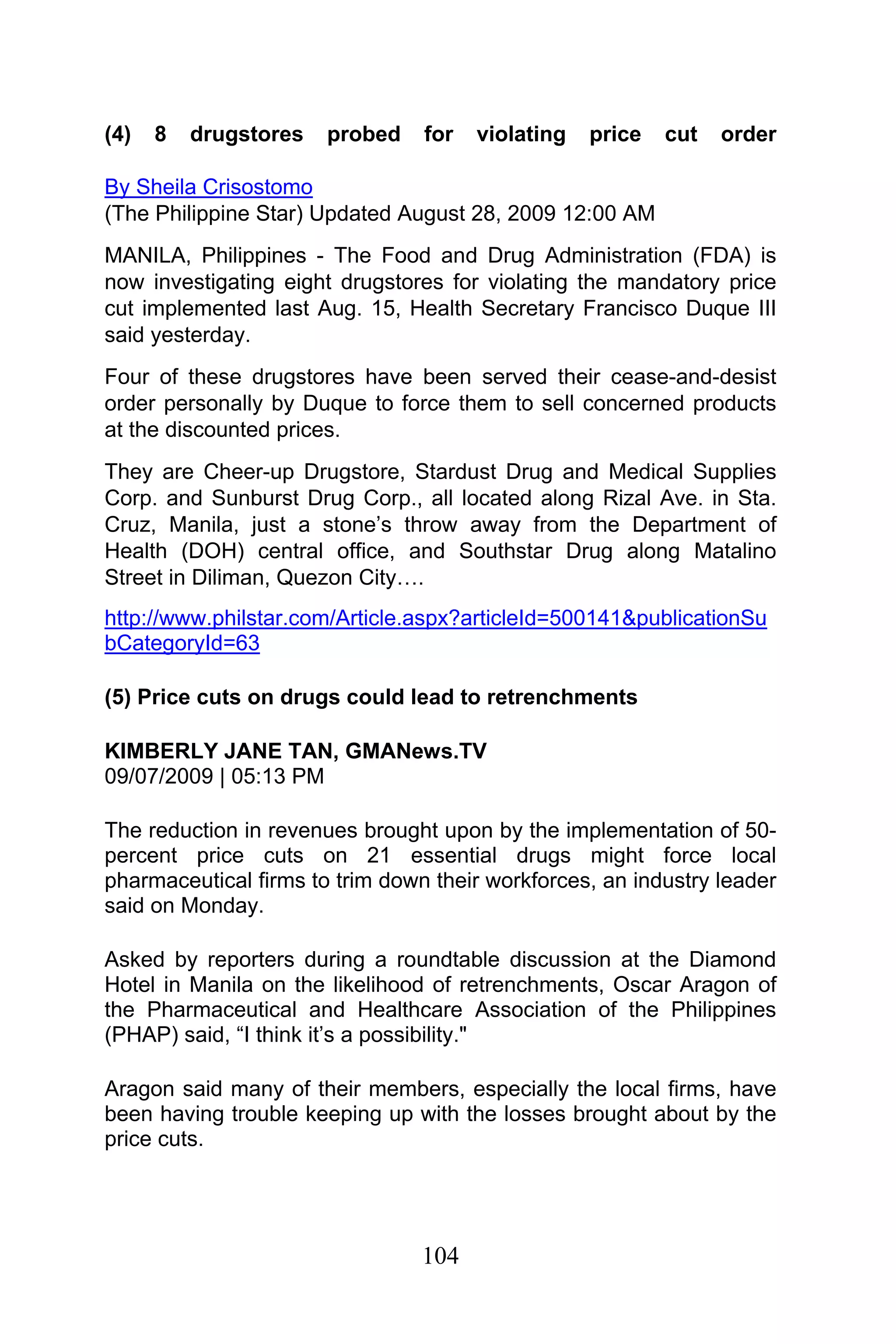
(14) Palace backs DOH on hospital audit
Written by Mia Gonzalez / Reporter
MONDAY, 21 SEPTEMBER 2009 21:58
THE plan of private hospitals to increase their administrative fees,
partly to make up for the shrinking profits from in-house pharmacies
that are now forced to comply with the cheaper- medicines law, has
sparked a dare by the Department of Health (DOH) for them to open
their books to ascertain the urgency of their plan. On Monday, Deputy
Presidential Spokesman Roilo Golez said Malacañang fully supports
the DOH demand.
The Private Hospitals Association of the Philippines (PHAP) said their
move is designed to recoup “losses from the implementation of the
cheaper-medicines law.”
But Golez said the Palace is not fully convinced that is the reason. “It
is possible that [lower-priced] medicine is not the problem. . . . All
stakeholders, including hospital administrations, DOH representatives,
PhilHealth, suppliers and other representatives of the health-care
industry in the country should sit down and have a dialogue.”…
http://www.businessmirror.com.ph/home/top-news/16319-palace-
backs-doh-on-hospital-audit.html
(15) Don’t tax medicines — Pia
September 23, 2009 06:46 PM Wednesday
By: Bernadette E. Tamayo
“There’s a lot that can be done to reduce the cost of health care in
the country if only the private sector and government would work
together,” said Ca-yetano, chairperson of the Senate committee on
social justice….
“Aside from the Cheaper Medicines Law, the government should
consider removing the 12 percent Value Added Tax on essential
medicines and medical equipment. Placing VAT on essential drugs is
like government earning from the sickness of our people,” she said.
She said the government should also consider reducing or removing](https://image.slidesharecdn.com/healthchoicesandresponsibilities-130908111852-/75/Health-Choices-and-Responsibilities-121-2048.jpg)




![117
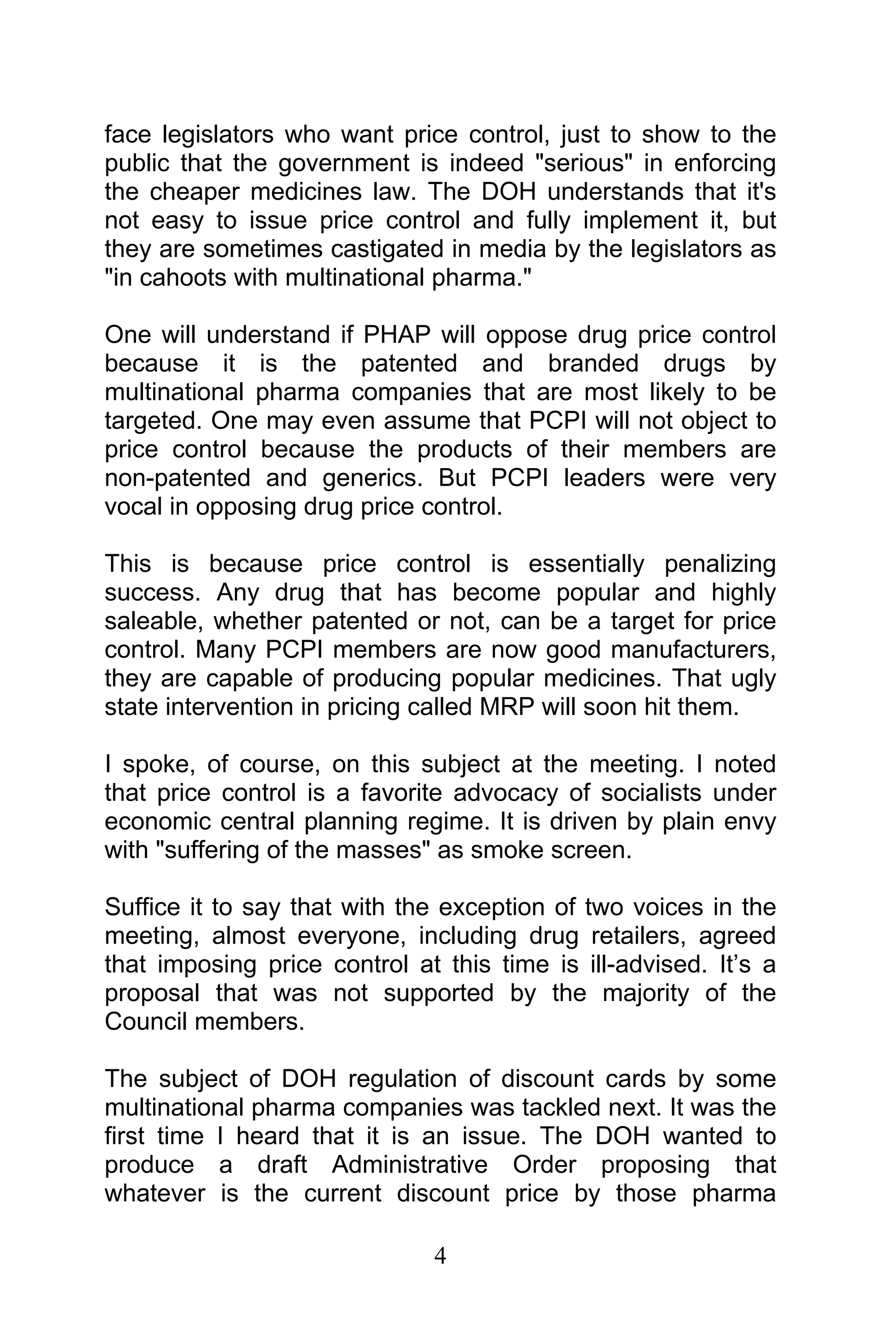
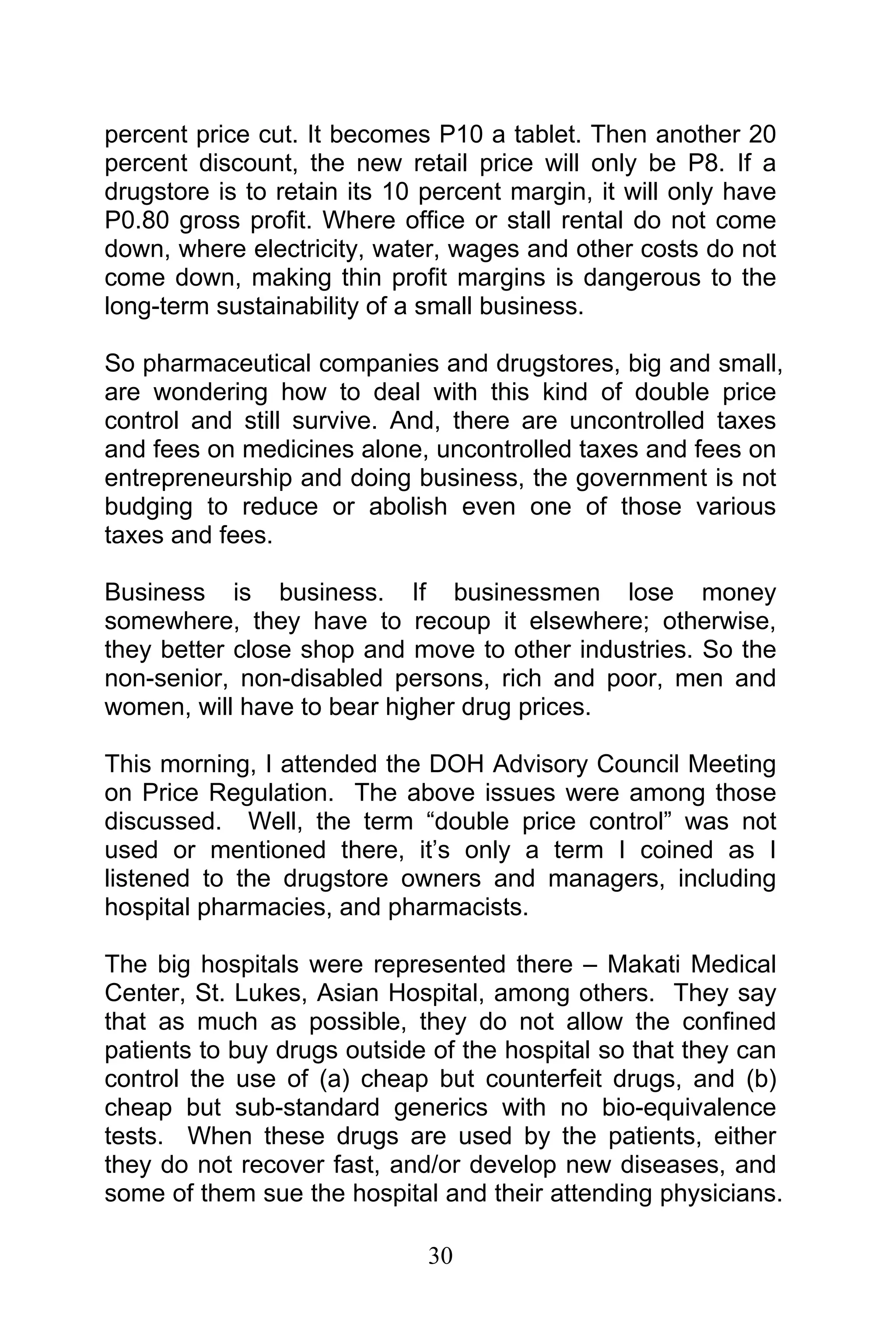
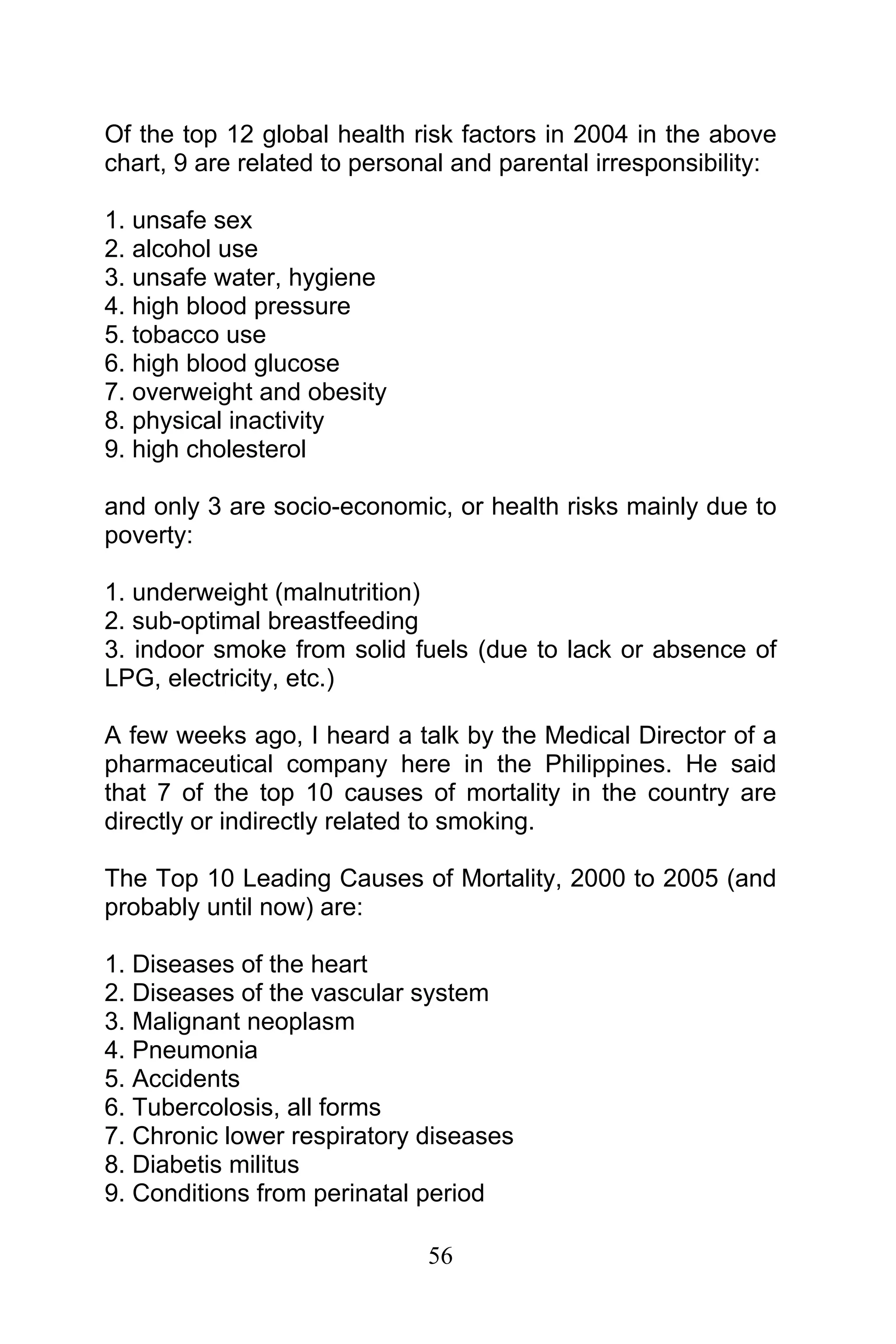
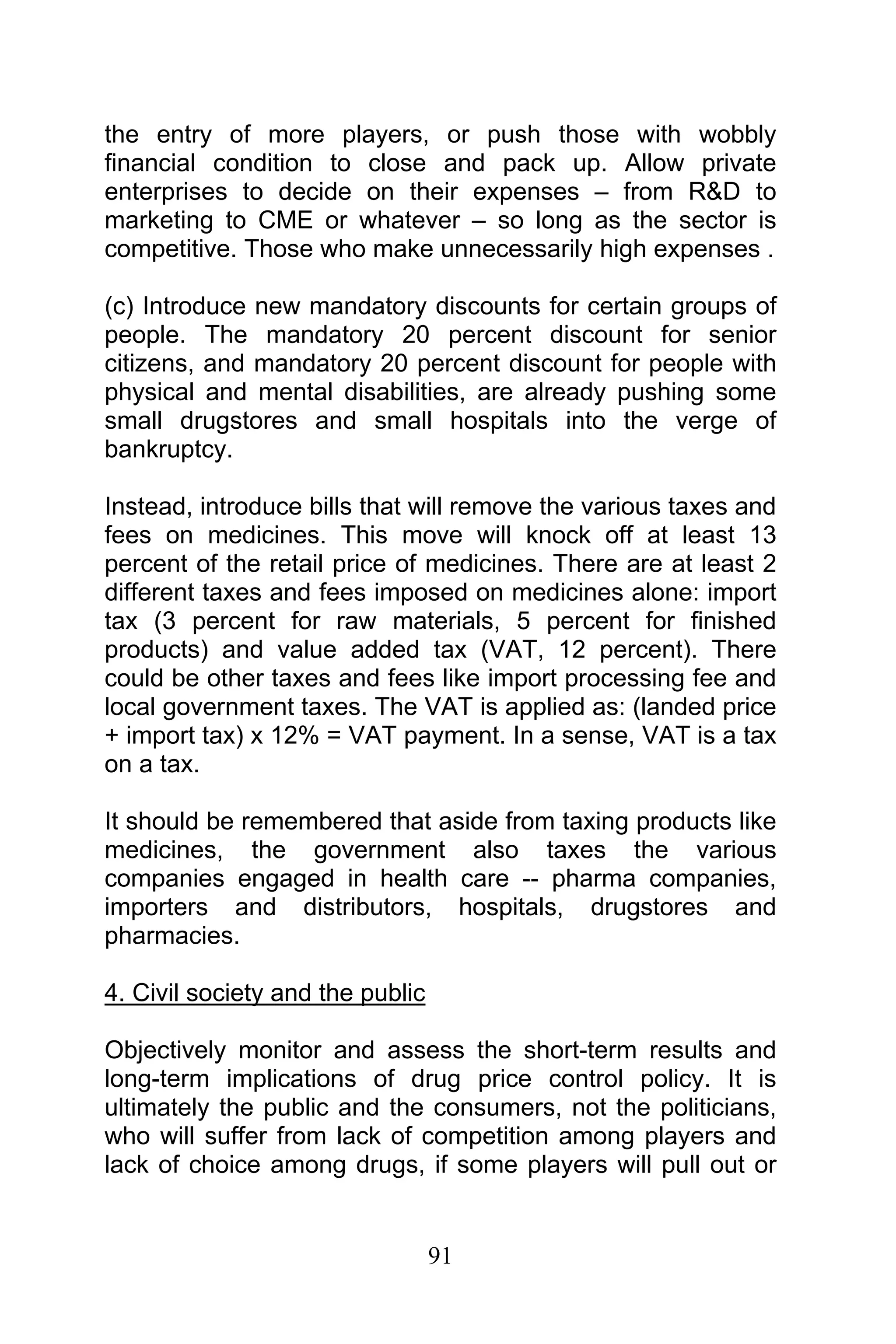
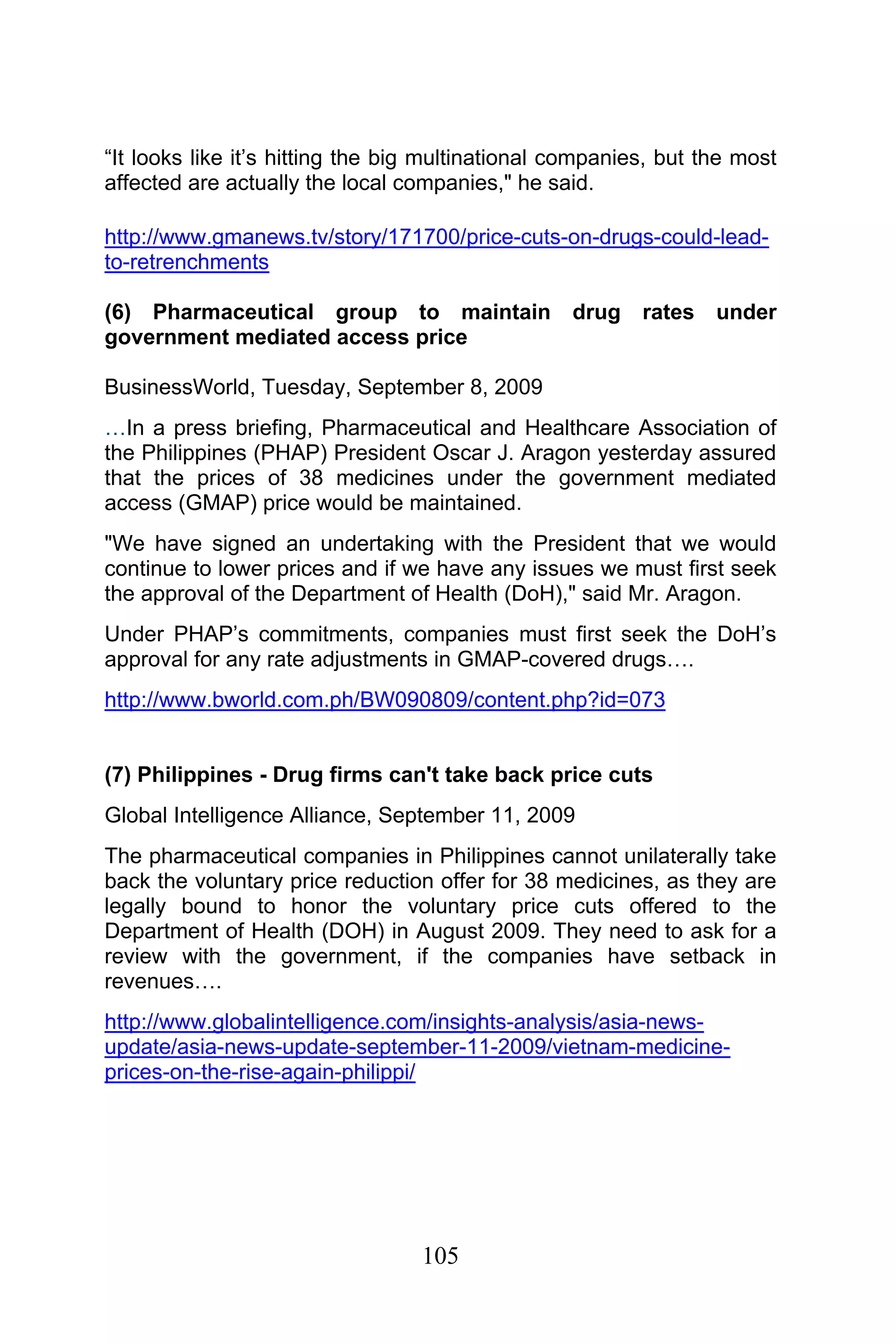
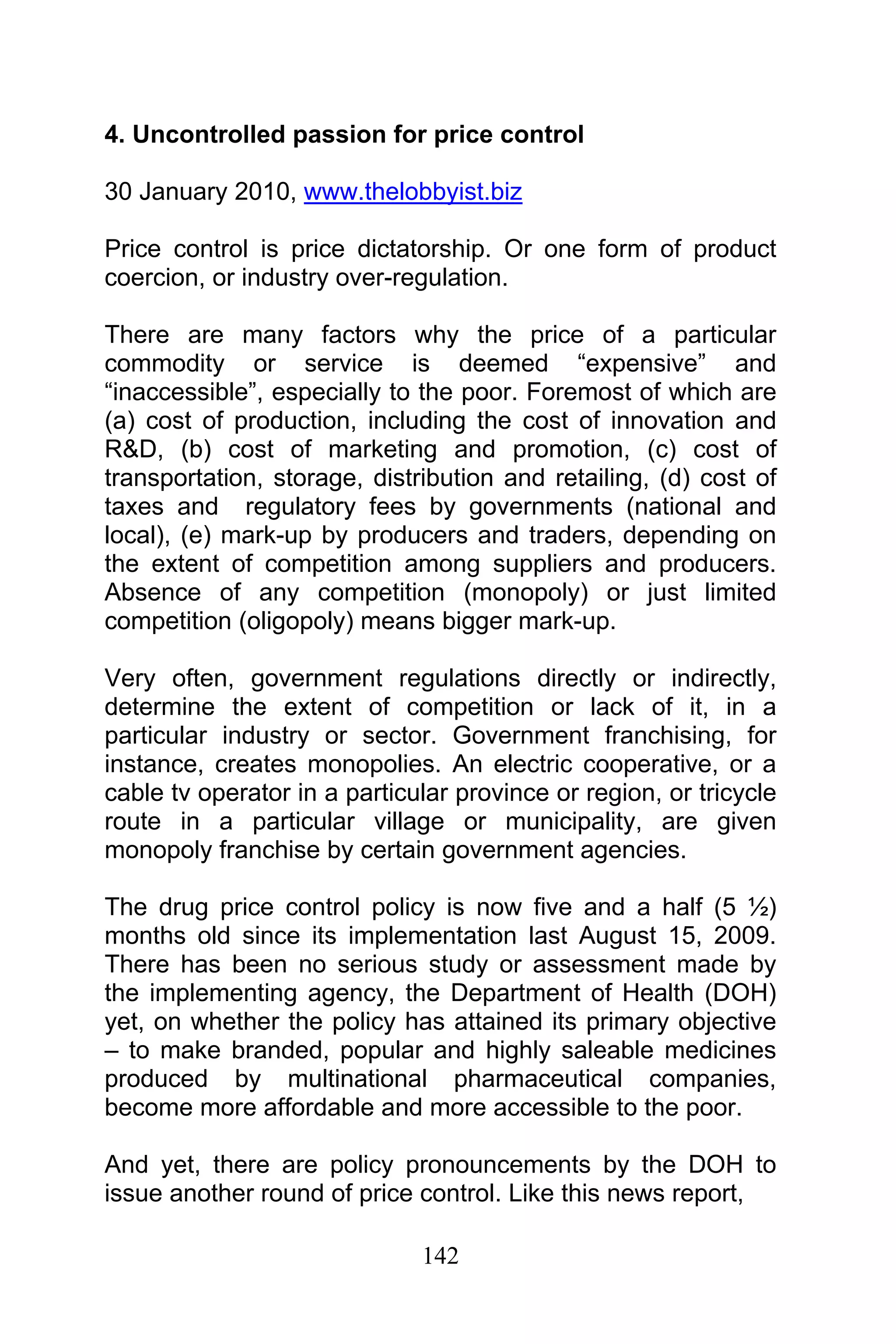
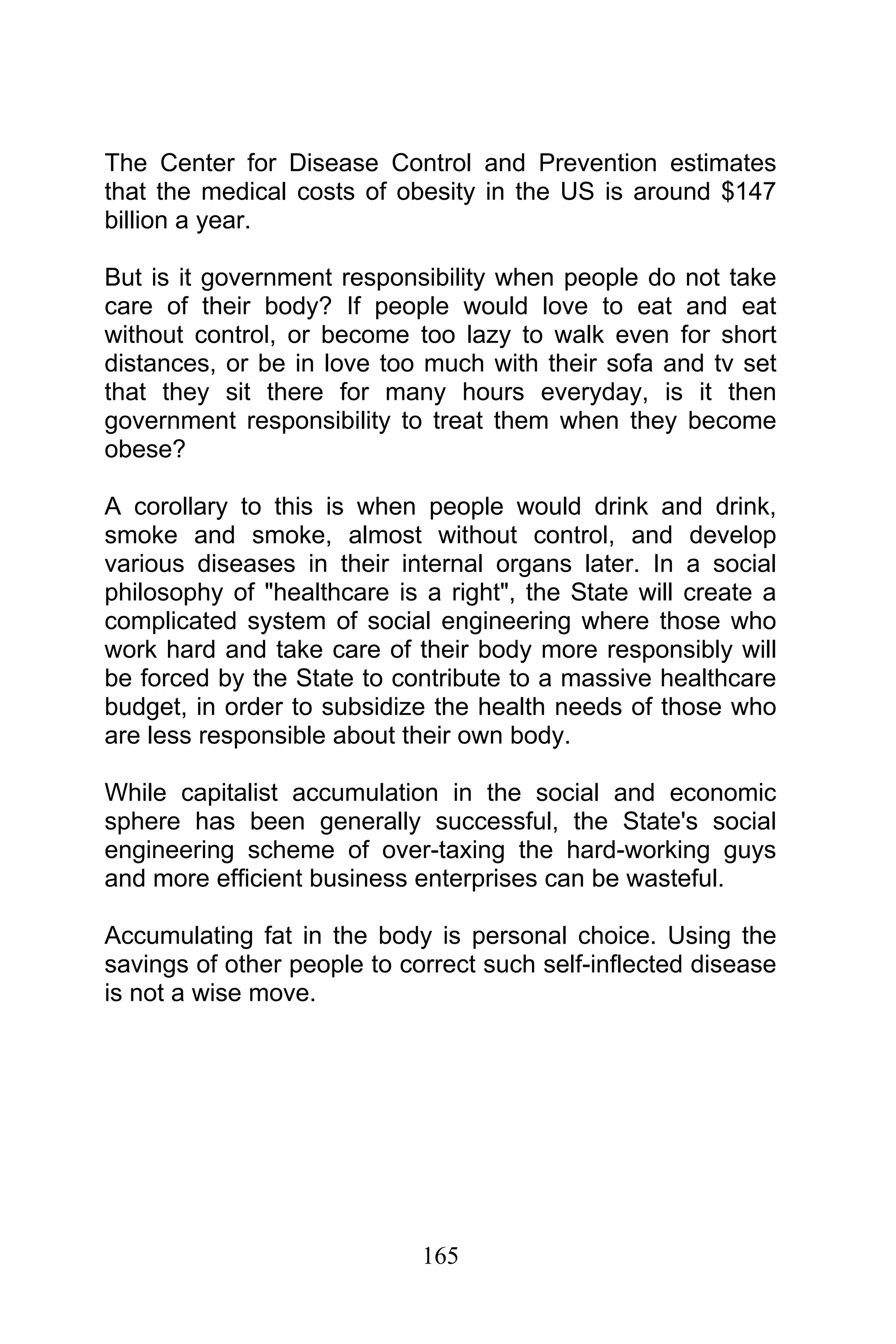
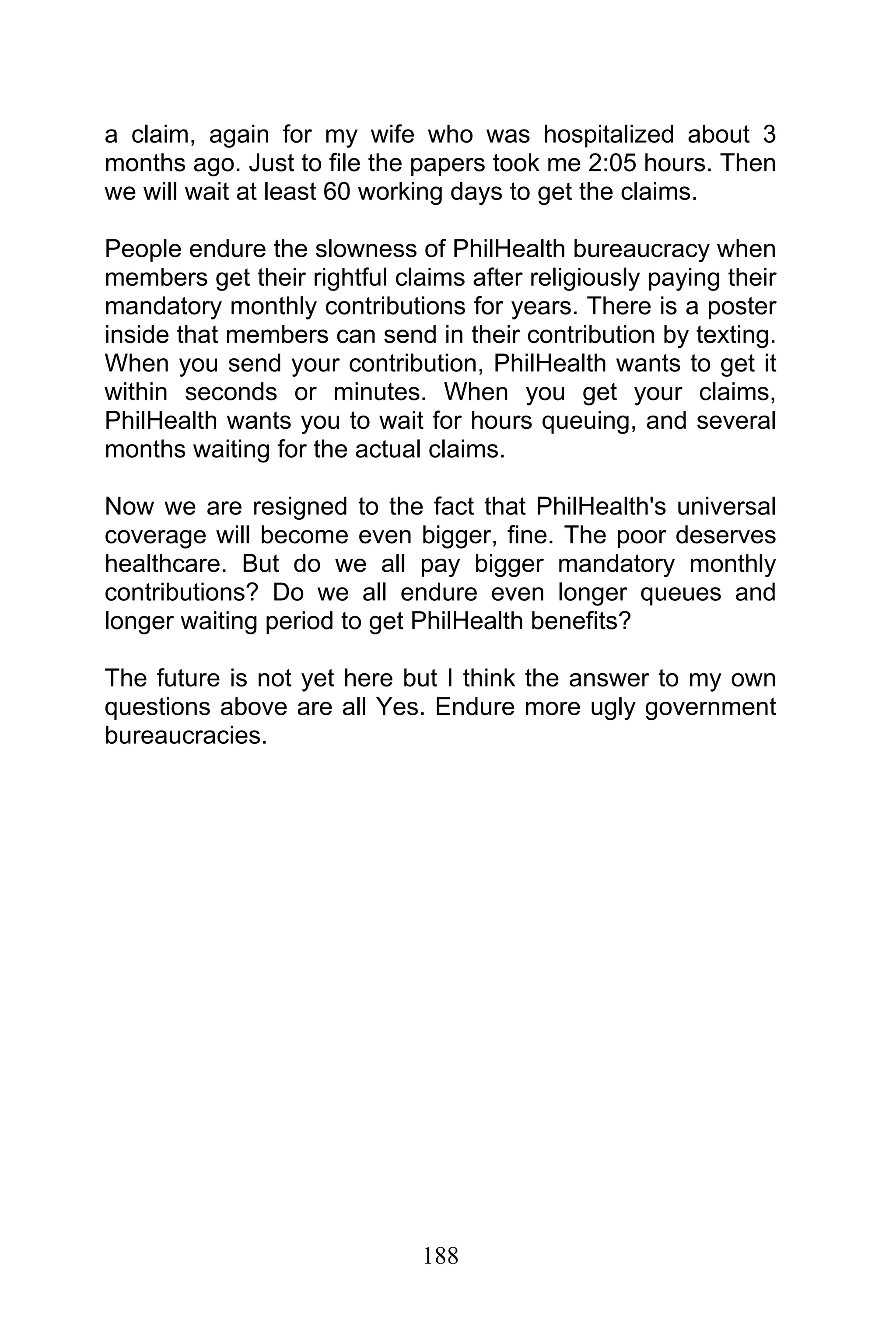
Annex 7. DOH Initial List for Drugs Price Freeze
(After the calamity caused by typhoon “Ondoy” last September 25;
this list was released by the DOH last October 6, 2009)
1. Ascorbic acid 500 mg tablet
2. Ascorbic acid 100 mg/5 mL syrup, 60 mL bottle
3. Cefalexin 250 mg/ 5 mL granules/powder for syrup/suspension,
60 mL (as monohydrate)
4. Cefalexin 500 mg capsule (as monohydrate)
5. Chloramphenicol 125 mg/5 mL suspension, 60 mL (as
palmitate)
6. Chloramphenicol 500 mg tablet
7. Cloxacillin 125 mg/5 mL powder for suspension, 60 mL bottle
(as sodium salt)
8. Cloxacillin 500 mg capsule (as sodium salt)
9. Cotrimoxazole: 200 mg sulfamethazole + 40 mg trimethoprim
per 5 mL suspension, 60 mL bottle
10. Cotrimoxazole: 400 mg sulfamethazole + 80 mg trimethoprim
per tablet
11. Cotrimoxazole: 800 mg sulfamethazole + 160 mg trimethoprim
per tablet
12. Lagundi 300 mg tablet {Vitex negundo, L. Fam (Verbenaceae)}
13. Lagundi 300 mL/5 mL syrup, 60 mL bottle {Vitex negundo, L.
Fam (Verbenaceae)}
14. Mefenamic acid 500 mg capsule
15. Metronidazole 125 mg base/5 mL (200 mg/mL as benzoate)
suspension, 60 mL bottle
16. Metronidazole 500 mg tablet
17. Metroprolol 100 mg capsule (as tartrate)
18. Nifedipine 5 mg capsule
19. Paracetamol 250 mg/5 mL syrup, 60 mL bottle (alcohol free)
20. Paracetamol 500 mg tablet
21. Paracetamol 120 mg/5 mL (125 mg/5 mL) syrup/suspension,
60 mL bottle (alcohol free)
22. Povidone iodine 10% topical solution, 60 mL bottle
23. Salbutamol 2 mg tablet (as sulfate)
24. Salbutamol 2 mg/5 mL syrup, 60 mL bottle (as sulfate)
25. Salbutamol 1 mg/mL (2.5 mL) respiratory solution (for
nebulization) unit dose (as sulfate)
26. Sambong [Blumea balsamifera, L. DC (Fam. Compositea)]
27. Vitamin B1 B6 B12 (100 mg + 5 mg + 50 mcg) tablet/capsule](https://image.slidesharecdn.com/healthchoicesandresponsibilities-130908111852-/75/Health-Choices-and-Responsibilities-129-2048.jpg)



















































![199
According to "New medicines in development",
http://innovation.org/index.cfm/FutureofInnovation/NewMedic
inesinDevelopment,
Today, over 2,950 new medicines are in development.
Many of these potential new medicines will fail in
clinical trials, but some may represent tomorrow's new
treatments. Bringing each new medicine to patients will
require, on average, 10 to 15 years of testing and
review.[i]
This database includes medicines currently in clinical
trials or at FDA for review. The information contained
in this database was derived from Wolters Kluwer
Health's database
http://www.wolterskluwerpharma.com/ and is published
with permission under license with Wolters Kluwer
Health.
That is something that many patients can look up to. There
are old, cheaper drugs and treatment that are available from
competing generics producers. And there will be new,
patented and more expensive drugs that will be made
available by a few innovator companies. Price will definitely
be an issue, no question about that. But it's saving the life of
a loved one that is the bigger issue.](https://image.slidesharecdn.com/healthchoicesandresponsibilities-130908111852-/75/Health-Choices-and-Responsibilities-211-2048.jpg)








![215
companies have fewer product offerings and do not have
other market avenues."
On the other hand, it appears that foreign firms are likely to
grow in the long run. Although their product prices are
affected as well, the Philippine market is considerably small
(about 5% of the global sales of multinational corporations)
and, these companies can afford to divert their attention to
other markets. They already hold a lead in manufacturing
and retail revenue, according to 2008 PHAP figures. Foreign
firms garnered total sales of PHP71.12 billion ($1.46 billion)
compared to local ones at PHP32.46 billion ($0.69 million).
Oplas believes that foreign drug manufacturers should feel
encouraged to remain on Filipino soil to help develop the
local pharmaceutical industry. The majority of MNCs in the
country are focused on drug discovery, which can, in turn,
create opportunities for local firms to produce generic
versions when innovator-drug patents expire….
Ultimately, patients are the losers. "We are likely to expect a
fall in the number of generics companies and medicines in
the country, which in turn, limits treatment options for doctors
and patients," says Oplas. "Also, it is also possible that a
black market emerges when storage, dispensation, and sale
of essential medicines are no longer transparent [or
competitive]. This paves the way for the entry of counterfeit
drugs that are perfect substitutes for effective and expensive
medicines."](https://image.slidesharecdn.com/healthchoicesandresponsibilities-130908111852-/75/Health-Choices-and-Responsibilities-227-2048.jpg)





The DOH Advisory Council on Price Regulation discussed several important issues regarding the implementation of the Cheaper Medicines Law: 1) There was debate around imposing price controls on drugs, with most council members opposed due to concerns it could penalize successful companies and discourage innovation. 2) The council discussed pharmaceutical discount cards and a DOH proposal to make discount prices universal, which Nonoy Oplas argued could penalize companies offering discounts. 3) Updates were provided on drugs recommended for maximum retail price issuance by the President and a proposed administrative order to implement price controls.



































































