
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Neoplasia
Similar to Neoplasia (20)
Recently uploaded
Recently uploaded (20)
Neoplasia
- 2. The term ‘neoplasia’ means new growth The new growth produced is called ‘neoplasm’ or ‘tumour’. All ‘new growths’ are not neoplasms Examples - embryogenesis, regeneration and repair, hyperplasia and hormonal stimulation…..
- 3. A mass of tissue formed as a result of abnormal, excessive, uncoordinated, autonomous and purposeless proliferation of cells even after cessation of stimulus for growth which caused it…. BENIGN - when they are slow-growing and localized without causing much difficulty to the host MALIGNANT- when they proliferate rapidly, spread through out the body and may eventually cause death of the host. The common term used for all malignant tumors is cancer of stimulus for growth which caused it.
- 4. Benign as well as Malignant Two basic components Parenchyma: - comprised by proliferating tumour cells; parenchyma determines the nature and evolution of the tumour. Supportive stroma: - composed of fibrous connective tissue and blood vessels; it provides the framework on which the parenchymal tumour cells grow.
- 5. SPECIAL CATEGORIES OF TUMOURS. 1. Mixed tumours: 1. Adenosquamous carcinoma -is the combination of adenocarcinoma and squamous cell carcinoma in the endometrium. 2.Adenoacanthoma- is the mixture of adenocarcinoma and benign squamous elements in the endometrium. 3. Carcinosarcoma - is the rare combination of malignant tumour of the epithelium (carcinoma) and of mesenchymal tissue (sarcoma) such as in thyroid. .
- 6. CONTD… 4. Collision tumour - morphologically two different cancers in the same organ which do not mix with each other. 5. Mixed tumour of the salivary gland (or pleomorphic adenoma) is the term used for benign tumour having combination of both epithelial and mesenchymal tissue elements
- 7. 2. Teratomas. These tumours are made up of a mixture of Arising from totipotent cells derived from the three germ cell layers—ectoderm, mesoderm & endoderm. Most common sites - ovaries & testis (gonadal teratomas). Also occur at extra-gonadal sites as well, mainly in the midline of the body such as - Head and neck region, - Mediastinum, - Retroperitoneum, - Sacrococcygeal region etc. - Teratomas may be benign or mature
- 8. 3. Blastomas (Embryomas). Blastomas or embryomas are a group of malignant tumours which arise from embryonal or partially differentiated cells These tumours occur more frequently in infants and children. (under 5 years of age) Examples: neuroblastoma, nephroblastoma (Wilms’tumour), hepatoblastoma,retinoblastoma,medulloblastoma,pulmonary blastoma.
- 9. CONTD… 4. Hamartoma. Mature but disorganised cells of tissues indigenous to the particular organ .E.g. Hamartoma . 5. Choristoma. choristoma is heterotopia but is not a true tumour, though it sounds like one.
- 10. I. TUMOURS OF ONE PARENCHYMAL CELL TYPE A. Epithelial Tumours BENINGN MALIGNANT 1 . Squamous epithelium: Squamous cell papilloma - Squamous cell (Epidermoid carcinoma) 2. Transitional epithelium : Transitional cell papilloma - Transitional cell carcinoma 3. Glandular epithelium : Adenoma - Adenocarcinoma 4. Basal cell layer skin — : - Basal cell carcinoma 5. Neuroectoderm : Naevus Melanoma - (Melanocarcinoma) 6. Hepatocytes :Liver cell adenoma - Hepatoma (Hepatocellular carcinoma) 7. Placenta (Chorionic epithelium) Hydatidiform mole - Choriocarcinoma
- 11. B. Non-epithelial (Mesenchymal) Tumours: BENINGN MALIGNANT 1. Adipose tissue: Lipoma Liposarcoma 2. Adult fibrous tissue: Fibroma Fibrosarcoma 3. Embryonic fibrous tissue: Myxoma Myxosarcoma 4. Cartilage : Chondroma Chondrosarcoma 5. Bone: Osteoma Osteosarcoma 6. Synovium: Benign synovioma Synovial sarcoma 7. Smooth muscle : Leiomyoma Leiomyosarcoma 8. Skeletal muscle: Rhabdomyoma Rhabdomyosarcoma 9. Mesothelium : Mesothelioma 10. Blood vessels: Haemangioma Angiosarcoma 11. Lymph vessels: Lymphangioma Lymphangiosarcoma 12. Glomus : Glomus tumour 13. Meninges: Meningioma Invasivemeningioma 14. Haematopoietic cells : Leukaemias 15. Lymphoid tissue: Pseudolymphoma Malignant lymphomas 16. Nerve sheath: Neurilemmoma Neurofibroma Neurogenic sarcoma 17. Nerve cells : Ganglioneuroma Neuroblastoma
- 12. II. MIXED TUMOURS BENINGN MALIGNANT Salivary glands : Pleomorphic adenoma - Malignant mixed Salivary Tumour. III. TUMOURS OF MORE THAN ONE GERM CELL LAYER Totipotent cells in gonads or in embryonal rests : Mature teratoma - Immature teratoma
- 13. CHARACTERISTICS OF TUMOURS I. Rate of growth II. Cancer phenotype and stem cells III. Clinical and gross features IV. Microscopic features V. Local invasion (Direct spread) VI. Metastasis (Distant spread).
- 14. I. RATE OF GROWTH: The rate at which the tumour enlarges depends upon 2 main factors 1. Rate of cell production, growth fraction and rate of cell loss 2. Degree of differentiation of the tumour. 1. Rate of cell production, growth fraction and rate of cell loss. Rate of growth of a tumour depends upon 3 important parameters: i) Doubling time of tumour cells, ii) number of cells remaining in proliferative pool (growth fraction), iii) rate of loss of tumour cells by cell shedding.
- 15. 2. Degree of differentiation: - Malignant tumour is directly proportionate to the degree of differentiation. - Poorly differentiated tumours show aggressive growth pattern as compared to better differentiated tumours. - Some tumours, after a period of slow growth, may suddenly show spurt in their growth due to development of an aggressive clone of malignant cells. - On the other hand, some tumours may cease to grow after sometime.
- 16. The regulation of tumour growth is under the control of growth factors secreted by the tumour cells. i) Epidermal growth factor (EGF) ii) Fibroblast growth factor (FGF) iii) Platelet-derived growth factor (PDGF) iv) Colony stimulating factor (CSF) v) Transforming growth factors-β (TGF-β) vi) Interleukins (IL) vii) Vascular endothelial growth factor (VEGF)
- 17. II. CANCER PHENOTYPE AND STEM CELLS Cancer cells disobey the growth controlling signals in the body & thus proliferate rapidly. ii) Cancer cells escape death signals and achieve immortality. iii) Imbalance between cell proliferation and cell death in cancer causes excessive growth. iv) Cancer cells lose properties of differentiation and thus perform little or no function. v) Due to loss of growth controls, cancer cells are genetically unstable & develop newer mutations. vi) Cancer cells overrun their neighbouring tissue and invade locally. vii) Cancer cells have the ability to travel from the site of origin to other sites in the body where they colonise and establish distant metastasis.
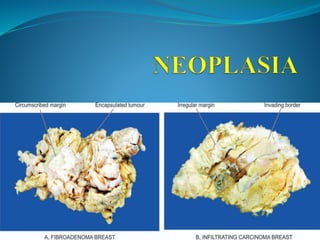
- 18. III. CLINICAL AND GROSS FEATURES Benign tumours : spherical or ovoid in shape. They are encapsulated or well-circumscribed, freely movable, more often firm and uniform, unless secondary changes like hemorrhage or infarction supervene Malignant tumours: Irregular in shape, poorly-circumscribed and extend into the adjacent tissues. Sarcomas arebTypically have fish-flesh like consistency while carcinomas are generally firm.
- 19. IV. MICROSCOPIC FEATURES These features which are appreciated in histologic sections are as under: 1. microscopic pattern 2. cytomorphology of neoplastic cells (differentiation and anaplasia) 3. tumour angiogenesis and stroma and 4. inflammatory reaction.
- 20. 1. Microscopic Pattern The tumour cells may be arranged in a variety of patterns in different tumours as under: The epithelial tumours generally consist of acini, sheets, columns or cords of epithelial tumour cells that may be arranged in solid or papillary pattern . The mesenchymal tumours have mesenchymal tumour cells arranged as interlacing bundles, fasicles or whorls, lying separated from each other usually by the intercellular matrix substance such as hyaline material in leiomyoma.cartilaginous matrix in chondroma, osteoid in osteosarcoma, reticulin network in soft tissue sarcomas etc.. Mixed patterns tumours e.g. teratoma arising from totipotent cells, pleomorphic adenoma of salivary gland (mixed salivary tumour), fibroadenoma of the breast, carcinosarcoma of the uterus and various other combinations of tumour types. Haematopoietic tumours such as leukaemias and lymphomas often have none or little stromal support.
- 22. 2. Cytomorphology of Neoplastic Cells : (Differentiation & Anaplasia) Differentiation : Extent of morphological and functional resemblance of parenchymal tumour cells to or responding normal cells. Poorly differentiated’, ‘undifferentiated’ or ‘dedifferentiated’ are synonymous terms for poor structural and functional resemblance to corresponding normal cell. Anaplasia : Lack of differentiation and is a characteristic feature of most malignant tumours. Depending upon the degree of differentiation, the extent of anaplasia is also variable i.e. poorly differentiated malignant tumours have high degree of anaplasia.
- 23. Poorly differentiated malignant tumours have high degree of anaplasia. As a result of anaplasia, noticeable morphological and functional alterations in the neoplastic cells are observed. 1.Loss of polarity 2.Pleomorphism 3.N:C ratio 4.Anisonucleosis 5.Hyperchromatism 6.Nucleolar changes. 7.Mitotic figures. 8.Tumour giant cells 9.Functional changes
- 25. 3. Tumour Angiogenesis and Stroma i) Microvascular density. The new capillaries add to the vascular density of the tumour which has been used as a marker to assess the rate of growth of tumours and hence grade the tumours. This is done by counting microvascular density in the section of the tumour. ii) Central necrosis. If the tumour outgrows its blood supply as occurs in rapidly growing tumours or tumour angiogenesis fails, its core undergoes ischaemic necrosis. TUMOUR STROMA. If the epithelial tumour is almost entirely composed of parenchymal cells, it is called medullary e.g. medullary carcinoma of the breast, medullary carcinoma of the thyroid. If there is excessive connective tissue stroma in the epithelial tumour, it is referred to as desmoplasia and the tumour is hard or scirrhous e.g. infiltrating duct carcinoma Breast, linitis plastica of the stomach.
- 26. 4. Inflammatory Reaction Prominent inflammatory reaction is present in and around the tumours. It could be the result of ulceration in the cancer when there is secondary infection. The inflammatory reaction in such instances may be acute or chronic. The examples of such reaction are: Seminoma testis ,malignant melanoma of the skin, lymphoepithelioma of the throat, medullary carcinoma of the breast, choriocarcinoma, Warthin’s tumour of salivary glands etc
- 27. V. LOCAL INVASION (DIRECT SPREAD) BENIGN TUMOURS. Most benign tumours form encapsulated or circumscribed masses that expand and push aside the surrounding normal tissues without actually invading, infiltrating or metastasising. Malignant tumours: - Malignant tumours also enlarge by expansion and some well- differentiated tumours may be partially encapsulated as well e.g. follicular carcinoma thyroid. - Often, cancers extend through tissue spaces, permeate lymphatic's, blood vessels, perineural spaces and may penetrate a bone by growing through nutrient foramina. More commonly, the tumours invade thin walled capillaries and veins than thick- walled arteries
- 28. VI. METASTASIS (DISTANT SPREAD) Metastasis (meta = transformation, stasis = residence) Routes of Metastasis: Cancers may spread to distant sites by following pathways: 1. Lymphatic spread 2. Haematogenous spread 3. Spread along body cavities and natural passages (Transcoelomic spread, along epithelium-lined surfaces, spread via cerebrospinal fluid, implantation).
- 29. LYMPHATIC SPREAD. In general, carcinomas metastasis by lymphatic route while sarcomas favour haematogenous route. I) Lymphatic permeation. The walls of lymphatics are readily Invaded by cancer cells and may form a continuous growth in the lymphatic channels called lymphatic permeation. ii) Lymphatic emboli. Alternatively, the malignant cells may detach to form tumour emboli so as to be carried along the lymph to the next draining lymph node. The tumour emboli enter the lymph node at its convex surface and are lodged in the subcapsular sinus where they start growing Virchow’s lymph node: Is nodal metastasis preferentially to supraclavicular lymph node from cancers of abdominal organs e.g. cancer stomach, colon, and gall bladder.
- 30. 2. HAEMATOGENOUS SPREAD. Blood-borne metastasis is The common route for sarcomas but certain carcinomas alsofrequently metastasise by this mode, especially those of the lung,breast, thyroid, kidney, liver, prostate and ovary. The sites where blood-borne metastasis commonly occurs are: the liver, lungs, brain, bones, kidney and adrenals, all of which provide ‘good soil’ for the growth of ‘good seeds’ (seed-soil theory). 1.SYSTEMIC VEINS 2.PORTAL VEINS 3.ARTERIAL SPREAD 4.RETROGRADE SPREAD
- 31. 3. SPREAD ALONG BODY CAVITIES AND NATURAL PASSAGES. i) Transcoelomic spread. a) Carcinoma of the stomach seeding to both ovaries(Krukenberg tumour). b) Carcinoma of the ovary spreading to the entire peritonea cavity without infiltrating the underlying organs ii) Spread along epithelium-lined surfaces. iii) Spread via cerebrospinal fluid. iv) Implantation.
- 32. MECHANISM AND BIOLOGY OF INVASION AND METASTASIS: 1. Aggressive clonal proliferation and angiogenesis. The first step in the spread of cancer cells is the development of rapidly proliferating clone of cancer cells. This is explained on the basis of tumour heterogeneity. 2. Tumour cell loosening. Normal cells remain glued to each other due to presence of cell adhesion molecules (CAMs)i.e.E (epithelial)-cadherin. In epithelial cancers, there is either loss or inactivation of E-cadherin and also other CAMs of immunoglobulin super family, all of which results in loosening of cancer cells. 3. Tumour cell-ECM interaction. Loosened cancer cells are now attached to ECM proteins, mainly laminin and fibronectin.This attachment is facilitated due to profoundness of receptors on the cancer cells for both these proteins. There is also loss of integrins, the transmembrane receptors, further favoring invasion. 4. Degradation of ECM. Tumour cells over express proteases and matrix-degrading enzymes,metalloproteinases, thatincludes collagenases and gelatinase, while the inhibitors of metalloproteinases are decreased. Another protease,cathepsin D, is also increased in certain cancers. These enzymes bring about dissolution of ECM—firstly base mentmembrane of tumour itself, then make way for tumour cells through the interstitial matrix, and finally dissolve the basement membrane of the vessel wall.
- 33. 5. Entry of tumour cells into capillary lumen. The tumour cells after degrading the basement membrane are ready to migrate into lumen of capillaries or venules for which the following mechanisms play a role: i) Autocrine motility factor (AMF) is a cytokine derived from tumour cells and stimulates receptor-mediated motility of tumour cells. ii) Cleavage products of matrix components which are formed following degradation of ECM have properties of tumourcell chemotaxis, growth promotion and angiogenesis in the cancer. 6.Thrombus formation. The tumour cells protruding in the lumen of the capillary are now covered with constituents of the circulating blood and form the thrombus. Thrombus provides nourishment to the tumour cells and also protects them from the immune attack by the circulating host cells. 7. Extravasation of tumour cells. Tumour cells in the circulation (capillaries, venules, lymphatics) may mechanically block these vascular channels and attach to vascular endothelium. 8. Survival and growth of metastatic deposit. The extravasated malignant cells on lodgments in the right environment grow further under the influence of growth factors produced by host tissues, tumour cells and by cleavage products of matrix components. These growth factors in particular include: PDGF, FGF, TGF-β and VEGF.
- 34. Grading of cancer Grade I: Well-differentiated (less than 25% anaplastic cells). Grade II: Moderately-differentiated (25-50% anaplastic cells). . Grade III: Moderately-differentiated (50-75% anaplastic cells). . Grade IV: Poorly-differentiated or anaplastic (more than 75% anaplastic cells).
- 35. Staging The extent of spread of cancers can be assessed by 3 ways— - clinical examination, - investigations, - pathologic examination of the tissue removed. Two important staging systems currently followed are: - TNM - AJC TNM staging. (T for primary tumour, N for regional nodal involvement, & M for distant metastases) Developed by the UICC (Union Internationale Contre Cancer, Geneva. T0 to T4: In situ lesion to largest and most extensive primary tumour. N0 to N3: No nodal involvement to widespread lymph node involvement. M0 to M2: No metastasis to disseminated haematogenous metastases. AJC staging. American Joint Committee staging divides: American Joint Committee staging divides all cancers into stage 0 to IV 3 components of the preceding system - primary tumour - nodal involvement - distant metastases in each stage. TNM and AJC staging systems can be applied for staging most malignant tumours.
- 36. Five Most Common Primary Cancers in the World. Men Women Children (Under 20) 1. Lung Breast Acute leukemia (oral cavity in India) (cervix in India) 2. Prostate Lung CNS tumour 3. Colorectal Colorectal Bone sarcoma 4. Urinary bladder Endometrial Endocrine 5. Lymphoma Lymphoma Soft tissue sarcoma In general, most common cancers in the developed an developing countries are as under: Developed world: lung, breast, prostate & colorectal. Developing world: liver, cervical and oesophageal.
- 37. EPIDEMIOLOGIC FACTORS About one-third of all cancers worldwide are attributed to 9 modifiable life- style factors: Tobacco use, alcohol consumption, obesity, physical inactivity, low fiber diet, unprotected sex, polluted air, indoor household smoke, and contaminated injections. Besides the etiologic role of some agents discussed later, the pattern and incidence of cancer depends upon the following: A) A large number of predisposing epidemiologic factors or cofactors which include a number of endogenous host factors and exogenous environmental factors. B) Chronic non-neoplastic (pre-malignant) conditions. C) Role of hormones in cancer.
- 38. A. Predisposing Factors 1. FAMILIAL AND GENETIC FACTORS. i) Retinoblastom ii) Familial polyposis coli. iii)Multiple endocrine neoplasia (MEN). iv) Neurofibromatosis or von Recklinghausen’s disease. v) Cancer of the breast. vi) DNA-chromosomal instability syndromes.
- 39. 2. RACIAL AND GEOGRAPHIC FACTORS. i) White Europeans and Americans develop most commonly malignancies of the lung, breast, and colon. Liver cancer is uncommon in these races. Breast cancer is uncommon in Japanese women but is more common in American women. ii) Black Africans, on the other hand, have more commonly cancers of the skin, penis, cervix and liver. iii) Japanese have five times higher incidence of carcinoma of the stomach than the Americans.. .iv) South-East Asians, especially of Chinese origin develop nasopharyngeal cancer more commonly. v) Indians of both sexes have higher incidence of carcinomaof the oral cavity and upper aero digestive tract, while in females carcinoma of uterine cervix and of the breast run parallel in incidence. Cancer of the liver in India is more often due to viral hepatitis (HBV and HCV) and subsequent cirrhosis, while in western populations it is more often due to alcoholic cirrhosis.
- 40. 3. ENVIRONMENTAL AND CULTURAL FACTORS. i) Cigarette smoking ii) Alcohol abuse iii) Alcohol and tobacco together iv) Cancer of the cervix v) Penile cancer vi) Betel nut cancer viii) Certain constituents of diet vii) A large number of industrial and environmental substances 4. AGE. The most significant risk factor for cancer is age. Generally, cancers occur in older individuals past 5th decade of life (two-third of all cancers occur above 65 years of age),though there are variations in age incidence in different forms of cancers. other tumours in infancy and childhood are: neuroblastoma, nephroblastoma (Wilms’tumour), retinoblastoma, hepatoblastoma, rhabdomyosarcoma, Ewing’s sarcoma, teratoma and CNS tumours.
- 41. 5. SEX. Apart from the malignant tumours of organs peculiar to each sex, most tumours are generally more common in men than in women except cancer of the breast,gall bladder, thyroid and hypopharynx B.Chronic Non-neoplastic-Pre-malignant Conditions: Premalignant lesions are a group of conditions which predispose to the subsequent development of cancer. 1. Carcinoma in situ (intraepithelial neoplasia). When the cytological features of malignancy are present but the malignant cells are confined to epithelium without invasion across the basement membrane, it is called as carcinoma in situ or intraepithelial neoplasia (CIN). The common sites are as under: i) Uterine cervix at the junction of ecto- and endocervix ii) Bowen’s disease of the skin iii) Actinic or solar keratosis iv) Oral leukoplakia v) Intralobular and intraductal carcinoma of the breast.
- 42. 2. Some benign tumours. Commonly, benign tumours donot become malignant. However, there are some exceptions i) Multiple villous adenomas of the large intestine have high incidence of developing adenocarcinoma. ii) Neurofibromatosis (von Recklinghausen’s disease) may develop into sarcoma 3. Miscellaneous conditions. Certain inflammatory and hyperplastic conditions are prone to development of cancer, i) Patients of long-standing ulcerative colitis are predisposed to develop colorectal cancer. ii) Cirrhosis of the liver has predisposition to develop hepatocellular carcinoma. iii) Chronic bronchitis in heavy cigarette smokers may develop cancer of the bronchus. iv) Chronic irritation from jagged tooth or ill-fitting denture may lead to cancer of the oral cavity. v) Squamous cell carcinoma developing in an old burn scar(Marjolin’s ulcer).
- 43. C. Hormones and Cancer 1. OESTROGEN. 2. CONTRACEPTIVE HORMONES. 3. ANABOLIC STEROIDS. 4. HORMONE-DEPENDENT TUMOURS. A few examples of such phenomena are seen in humans: i) Prostatic cancer usually responds to the administration of oestrogens. ii) Breast cancer may regress with oophorectomy, hypophysectomy or on administration of male hormones. iii) Thyroid cancer may slow down in growth with administration of thyroxine that suppresses the secretion of TSH by the pituitary.