Technique for Placement of Oxidized Titanium Implants by Oded Bahat
EAO Stockholm easygraft
1. Background: Socket grafting without primary wound closure is proposed as a
minimally invasive technique that prevents the loss of both soft and hard tissues
after tooth extraction, while minimizing patient morbidity and surgical time.
Aim: To study and present the soft tissue secondary intention healing cascade
over post-extraction sockets grafted with in situ hardening alloplastic bone
substitutes, without achieving primary wound closure.
In 30 patients, 30 single extraction sites were grafted with an in situ hardening
alloplastic bone substitute (GUIDOR easy-graft CLASSIC, Sunstar, Etoy,
Switzerland) after atraumatic extraction without raising a flap. The material
consists of beta tricalcium phosphate (b-TCP) granules coated with poly(lactic-co-
glycolic acid; PLGA). Sites were covered with a hemostat sponge and a cross-
mattress suture was loosely placed over to stabilize the wound without obtaining
primary closure. Soft tissue healing over the grafted area was evaluated and
documented with clinical photographs in a regular basis for an average of 14
weeks. In 2 cases histological analysis of the newly-formed soft tissue was
possible.
In parallel, bone regeneration of the sites was evaluated radiologically and also
clinically at re-entry for placing the implant. Those data will be included in the
forthcoming publication of the study.
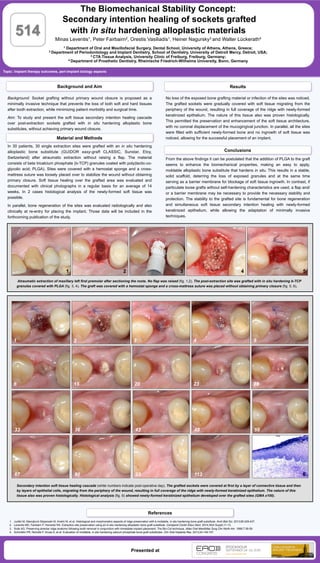
Atraumatic extraction of maxillary left first premolar after sectioning the roots. No flap was raised (fig. 1,2). The post-extraction site was grafted with in situ hardening b-TCP
granules covered with PLGA (fig. 3, 4). The graft was covered with a hemostat sponge and a cross-mattress suture was placed without obtaining primary closure (fig. 5, 6).
Material and Methods
Topic: Implant therapy outcomes, peri-implant biology aspects
The Biomechanical Stability Concept:
Secondary intention healing of sockets grafted
with in situ hardening alloplastic materials
Minas Leventis1, Peter Fairbairn2, Orestis Vasiliadis1, Heiner Nagursky3 and Walter Lückerath4
1 Department of Oral and Maxillofacial Surgery, Dental School, University of Athens, Athens, Greece;
2 Department of Periodontology and Implant Dentistry, School of Dentistry, University of Detroit Mercy, Detroit, USA;
3 CTA Tissue Analysis, University Clinic of Freiburg, Freiburg, Germany;
4 Department of Prosthetic Dentistry, Rheinische Friedrich-Wilhelms University, Bonn, Germany
514
References
Conclusions
1. Jurišić M, Manojlović-Stojanoski M, Andrić M, et al. Histological and morphometric aspects of ridge preservation with a moldable, in situ hardening bone graft substitute. Arch Biol Sci. 2013;65:429-437.
2. Leventis MD, Fairbairn P, Horowitz RA. Extraction site preservation using an in-situ hardening alloplastic bone graft substitute. Compend Contin Educ Dent. 2014;35(4 Suppl):11-13.
3. Sclar AG. Preserving alveolar ridge anatomy following tooth removal in conjunction with immediate implant placement. The Bio-Col technique. Atlas Oral Maxillofac Surg Clin North Am. 1999;7:39-59.
4. Schmidlin PR, Nicholls F, Kruse A, et al. Evaluation of moldable, in situ hardening calcium phosphate bone graft substitutes. Clin Oral Implants Res. 2013;24:149-157.
Background and Aim Results
Presented at
No loss of the exposed bone grafting material or infection of the sites was noticed.
The grafted sockets were gradually covered with soft tissue migrating from the
periphery of the wound, resulting in full coverage of the ridge with newly-formed
keratinized epithelium. The nature of this tissue also was proven histologically.
This permitted the preservation and enhancement of the soft tissue architecture,
with no coronal displacement of the mucogingival junction. In parallel, all the sites
were filled with sufficient newly-formed bone and no ingrowth of soft tissue was
noticed, allowing for the successful placement of an implant.
From the above findings it can be postulated that the addition of PLGA to the graft
seems to enhance the biomechanical properties, making an easy to apply,
moldable alloplastic bone substitute that hardens in situ. This results in a stable,
solid scaffold, deterring the loss of exposed granules and at the same time
serving as a barrier membrane for blockage of soft tissue ingrowth. In contrast, if
particulate loose grafts without self-hardening characteristics are used, a flap and/
or a barrier membrane may be necessary to provide the necessary stability and
protection. The stability to the grafted site is fundamental for bone regeneration
and simultaneous soft tissue secondary intention healing with newly-formed
keratinized epithelium, while allowing the adaptation of minimally invasive
techniques.
Secondary intention soft tissue healing cascade (white numbers indicate post-operative day). The grafted sockets were covered at first by a layer of connective tissue and then
by layers of epithelial cells, migrating from the periphery of the wound, resulting in full coverage of the ridge with newly-formed keratinized epithelium. The nature of this
tissue also was proven histologically. Histological analysis (fig. 6) showed newly-formed keratinized epithelium developed over the grafted sites (GMA x100).
1 2 3 4 5
1 2 3 4 5
6 15 20 23 28
33 36 43 48 59
67 80 93 113 6