Improving Pediatric Handover
•
1 like•96 views

A standardized handoff tool was implemented between the operating room and pediatric post-anesthesia care unit (PACU) at a hospital to improve communication. Prior to the tool, a review found miscommunication was responsible for up to 85% of hospital errors. Nurses analyzed various handoff methods and created a questionnaire to evaluate current practice. Data collected before and after implementing the tool showed completion of handoff elements increased, particularly around patient allergies, procedures, medications and history. The standardized tool improved interdisciplinary communication within one month and helps ensure efficient, safe and quality patient care during handoffs.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Improving Pediatric Handover
Similar to Improving Pediatric Handover (20)
Improving Pediatric Handover
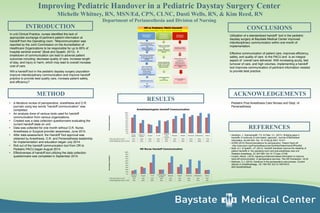
- 1. INTRODUCTION REFERENCES METHOD RESULTS CONCLUSIONS ACKNOWLEDGEMENTS Improving Pediatric Handover in a Pediatric Daystay Surgery Center Michelle Whitney, RN, MSN/Ed, CPN, CLNC, Dusti Wells, RN, & Kim Reed, RN Department of Perianesthesia and Division of Nursing In unit Clinical Practice, nurses identified the lack of appropriate exchange of pertinent patient information at handoff from the Operating room. “Miscommunication was reported by the Joint Commission on the Accreditation of Healthcare Organizations to be responsible for up to 85% of hospital sentinel events” (Boat and Spaeth, 2013). A breakdown of communication can lead to adverse patient outcomes including: decrease quality of care, increase length of stay, and injury or harm, which may lead to overall increase cost of care. Will a handoff tool in the pediatric daystay surgery population improve interdisciplinary communication and improve handoff practice to provide best quality care, increase patient safety, and efficiency? • A literature review of perioperative, anesthesia and O.R. journals using key words “handoff communication” was completed. • An analysis done of various tools used for handoff communication from various organizations. • Created was a data collection questionnaire evaluating the current handoff state on unit. • Data was collected for one month without O.R. Nurse, Anesthesia or Surgical provider awareness, June 2014. • After data assessment, the Handoff Tool approval was obtained by Anesthesia, O.R. and Perianesthesia leadership for implementation and education began July 2014. • Roll out of the handoff communication tool from OR to Pediatric PACU began August 2014. • Effectiveness of handoff tool utilizing the data collection questionnaire was completed in September 2014. • Abraham, J., Kannampallil, T.G. & Patel, V.L. (2011). Bridging gaps in handoffs: A continuity of care based approach. Journal of Biomedical Informatics, 45,240-254. Doi: 10.1016/j.jbi.2001.10.011 • AORN (2012) Recommendations for perioperative Patient Hand-off http://www.aorn.org/PracticeResources/ToolKits/PatientHandOffToolKit/ • Boat, A.C. & Spaeth, J.P. (2013). Handoff checklists improve the reliability of patient handoffs in the operating room and post anesthesia care unit. Pediatric Anesthesia, 23, 647-654. Doi:10.111/pan.12199 • Cooper, Alecia. ( 2010). Applying evidenced-based information to improve hand-off communication in perioperative services. The OR Connection, 18-24. • Kalkman, C.J. (2010). Handover in the perioperative care process. Current Opinion in Anesthesiology, 23: 749-753. Doi:10.1097/ACO. 0b013e3283405ac8 Pediatric Post Anesthesia Care Nurses and Dept. of Perianesthesia Utilization of a standardized handoff tool in the pediatric daystay surgery at Baystate Medical Center improved interdisciplinary communication within one month of implementation. Effective communication of patient care, improves efficiency, safety, and quality of care to the PACU and is an integral aspect of overall care delivered. With increasing acuity, fast turnover of care, and high volumes, implementing a handoff tool improves communication of pertinent information needed to provide best practice. Placed on monitor Oxygen Pt.ID IV (hung and running) Allergies Weight Procedure Medications History Pre June 2014 (n=53) 15% 33% 52% 20% 52% 32% 30% 26% 18% Post September 2014 (n=54) 19% 28% 89% 20% 81% 44% 67% 61% 19% 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% PercentageComplete OR Nurse Handoff Communication Airway History Placed on Monitor Oxygen Pt. ID IV(hung and running) Allergies Weight Procedure Medications History Pre June 2014 (n=53) 77% 49% 45% 34% 58% 70% 74% 81% 85% 77% Post September 2014 (n=54) 91% 65% 41% 63% 63% 85% 96% 89% 100% 96% 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% PercentageComplete Anesthesiologists Handoff Communication