International Study of Comparative Health Effectiveness with Medical and Inva...
Lyons SCCM poster Feb 07
1. Comparison of Impedance Cardiography and Thermodilution
Pulmonary Artery Catheterization in Post-Operative Hemodynamic
Monitoring of Hypervolemic Cardiac Surgery Patients
Lyons, M. Melanie1, Miller, Jim2; White, Marcia2, Crosby, Ivan2, Sonnad, Seema1, Horan, Annamarie1, Burns, Suzanne2, Gracias, Vicente1
1Division of Traumatology and Surgical Critical Care, The Hospital of the University of Pennsylvania, Philadelphia, Pennsylvania,
2Thoracic Cardiovascular Post-Op ICU, University of Virginia Health System, Charlottesville, Virginia
Post-op hemodynamic monitoring using
thermodilution pulmonary artery catheter (TD
PAC) is critical in the immediate hours following
cardiac surgery. The traditional approach
involves thermodilution via a pulmonary artery
catheter (TD PAC). However, the use of TD
PAC may produce complications including
catheter sepsis, bleeding, or pneumothorax,
and death. The second generation modules of
impedance cardiography (ICG) have
consistently shown to be a safe, valid and
reproducible tool of measure in the
management and treatment stratification of
congestive heart failure patients as well as
other subsets of patient population. We
examined the role of ICG in monitoring cardiac
index and stroke volume in the 8 hours
immediately following cardiac surgery.
INTRODUCTION
#215
Hemodynamic measurements obtained from
an ICG device will be as accurate as
measurements from a TD PAC in post-op
cardiac surgery patients.
HYPOTHESIS
§ 20 post-op cardiac surgery patients
were monitored using ICG and TD PAC
simultaneously for 8 hours following
arrival in a cardiac surgery ICU.
§ Cardiac index, stroke volume, fluid
volumes, output, and pre-op and end of
study weights were recorded at 4 time
points during the 8 hours further
analyzed.
§ Pearson and Spearman correlations
were calculated for cardiac index and
stroke volume. A subgroup analysis by
time period and net fluid volume were
also performed.
METHODS
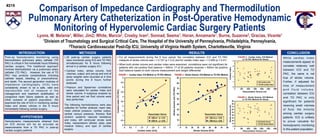
§ For all measurements during the 8 hour period, the correlation between ICG and TD PAC
measure of stroke volume was r = 0.157 (p = 0.2) and for cardiac index was r = 0.469 (p = 0.01).
§ When both stroke volume and cardiac index were examined, correlations were not significant for
patients with net positive fluid balance > 500ml. 17 of 20 patients received > 500ml net positive
fluid balance based on both volume measurement and weight differential.
RESULTS
While cardiac index
measurements appear to
correlate relatively well
between ICG and TD
PAC, the same is not
true of stroke volume.
Further, if adjusted for
time of measurement
a n d f l u i d v o l u m e ,
correlation between ICG
and TD PAC is only
significant for patients
receiving small volumes
of fluid, the minority
among cardiac surgery
patients. ICG is unlikely
to prove valuable for
hemodynamic monitoring
in this patient population.
CONCLUSION
The following hemodynamics were also
collected for further analysis: heart rate,
mean arterial pressure, cardiac output,
central venous pressure, thoracic fluid
content, systemic vascular resistance
and index, left ventricular stroke work
index, vasopressors utilized, peep, past
medical history, and type of cardiac
surgery.
FIGURE 1 - Cardiac Index: ICG Method vs TD PAC Method FIGURE 2 - Stroke Volume: ICG Method vs TD PAC Method
Cardiac Index (ICG)
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
0 0.5 1 1.5 2 2.5 3 3.5 4
CardiacIndex(TDPAC) <500 ml *p = 0.01
>500 ml p > 0.05
Resuscitation Volume
Stroke Volume (ICG)
0
10
20
30
40
50
60
70
80
90
0 10 20 30 40 50 60 70 80
StrokeVolume(ml)(TDPAC)
< 500 ml p > 0.05
> 500 ml p > 0.05
Resuscitation Volume
FIGURE 4 - Stroke Volume: ICG Method
vs TD PAC Method All Values
FIGURE 3 - Cardiac Index: ICG Method
vs TD PAC Method All Values
0
1
2
3
4
5
0 500 1000 1500 2000 2500 3000
Resuscitation Volume (ml)
CardiacIndex
ICG Cardiac Index
TD PAC Cardiac Index
0
10
20
30
40
50
60
70
80
90
0 500 1000 1500 2000 2500 3000
Resuscitation Volume (ml)
StrokeVolume(ml)
ICG-Stroke Volume
TD PAC Stroke Volume
2. Comparison of Impedance Cardiography and Thermodilution
Pulmonary Artery Catheterization in Post-Operative Hemodynamic
Monitoring of Hypervolemic Cardiac Surgery Patients
Lyons, M. Melanie1, Miller, Jim2; White, Marcia2, Crosby, Ivan2, Sonnad, Seema1, Horan, Annamarie1, Burns, Suzanne2, Gracias, Vicente1
1Division of Traumatology and Surgical Critical Care, The Hospital of the University of Pennsylvania, Philadelphia, Pennsylvania,
2Thoracic Cardiovascular Post-Op ICU, University of Virginia Health System, Charlottesville, Virginia
Post-op hemodynamic monitoring using
thermodilution pulmonary artery catheter (TD
PAC) is critical in the immediate hours following
cardiac surgery. The traditional approach
involves thermodilution via a pulmonary artery
catheter (TD PAC). However, the use of TD
PAC may produce complications including
catheter sepsis, bleeding, or pneumothorax,
and death. The second generation modules of
impedance cardiography (ICG) have
consistently shown to be a safe, valid and
reproducible tool of measure in the
management and treatment stratification of
congestive heart failure patients as well as
other subsets of patient population. We
examined the role of ICG in monitoring cardiac
index and stroke volume in the 8 hours
immediately following cardiac surgery.
INTRODUCTION
#215
Hemodynamic measurements obtained from
an ICG device will be as accurate as
measurements from a TD PAC in post-op
cardiac surgery patients.
HYPOTHESIS
§ 20 post-op cardiac surgery patients
were monitored using ICG and TD PAC
simultaneously for 8 hours following
arrival in a cardiac surgery ICU.
§ Cardiac index, stroke volume, fluid
volumes, output, and pre-op and end of
study weights were recorded at 4 time
points during the 8 hours further
analyzed.
§ Pearson and Spearman correlations
were calculated for cardiac index and
stroke volume. A subgroup analysis by
time period and net fluid volume were
also performed.
METHODS
§ For all measurements during the 8 hour period, the correlation between ICG and TD PAC
measure of stroke volume was r = 0.157 (p = 0.2) and for cardiac index was r = 0.469 (p = 0.01).
§ When both stroke volume and cardiac index were examined, correlations were not significant for
patients with net positive fluid balance > 500ml. 17 of 20 patients received > 500ml net positive
fluid balance based on both volume measurement and weight differential.
RESULTS
While cardiac index
measurements appear to
correlate relatively well
between ICG and TD
PAC, the same is not
true of stroke volume.
Further, if adjusted for
time of measurement
a n d f l u i d v o l u m e ,
correlation between ICG
and TD PAC is only
significant for patients
receiving small volumes
of fluid, the minority
among cardiac surgery
patients. ICG is unlikely
to prove valuable for
hemodynamic monitoring
in this patient population.
CONCLUSION
The following hemodynamics were also
collected for further analysis: heart rate,
mean arterial pressure, cardiac output,
central venous pressure, thoracic fluid
content, systemic vascular resistance
and index, left ventricular stroke work
index, vasopressors utilized, peep, past
medical history, and type of cardiac
surgery.
FIGURE 1 - Cardiac Index: ICG Method vs TD PAC Method FIGURE 2 - Stroke Volume: ICG Method vs TD PAC Method
Cardiac Index (ICG)
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
0 0.5 1 1.5 2 2.5 3 3.5 4
CardiacIndex(TDPAC) <500 ml *p = 0.01
>500 ml p > 0.05
Resuscitation Volume
Stroke Volume (ICG)
0
10
20
30
40
50
60
70
80
90
0 10 20 30 40 50 60 70 80
StrokeVolume(ml)(TDPAC)
< 500 ml p > 0.05
> 500 ml p > 0.05
Resuscitation Volume
FIGURE 4 - Stroke Volume: ICG Method
vs TD PAC Method All Values
FIGURE 3 - Cardiac Index: ICG Method
vs TD PAC Method All Values
0
1
2
3
4
5
0 500 1000 1500 2000 2500 3000
Resuscitation Volume (ml)
CardiacIndex
ICG Cardiac Index
TD PAC Cardiac Index
0
10
20
30
40
50
60
70
80
90
0 500 1000 1500 2000 2500 3000
Resuscitation Volume (ml)
StrokeVolume(ml)
ICG-Stroke Volume
TD PAC Stroke Volume