
Recommended
Recommended
More Related Content
Similar to Cdc safe patient handling and mobility (sphm) - niosh workplace safety and health topic
Similar to Cdc safe patient handling and mobility (sphm) - niosh workplace safety and health topic (20)
More from Martin Sanders PhD, CSP, ASP
More from Martin Sanders PhD, CSP, ASP (13)
Recently uploaded
Recently uploaded (20)
Cdc safe patient handling and mobility (sphm) - niosh workplace safety and health topic
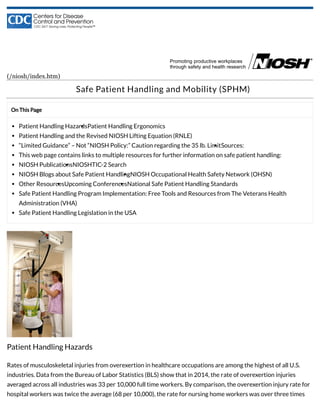
- 1. On This Page Patient Handling HazardsPatient Handling Ergonomics Patient Handling and the Revised NIOSH Lifting Equation (RNLE) “Limited Guidance” – Not “NIOSH Policy:” Caution regarding the 35 lb. LimitSources: This web page contains links to multiple resources for further information on safe patient handling: NIOSH PublicationsNIOSHTIC-2 Search NIOSH Blogs about Safe Patient HandlingNIOSH Occupational Health Safety Network (OHSN) Other ResourcesUpcoming ConferencesNational Safe Patient Handling Standards Safe Patient Handling Program Implementation: Free Tools and Resources from The Veterans Health Administration (VHA) Safe Patient Handling Legislation in the USA (/niosh/index.htm) Safe Patient Handling and Mobility (SPHM) Patient Handling Hazards Rates of musculoskeletal injuries from overexertion in healthcare occupations are among the highest of all U.S. industries. Data from the Bureau of Labor Statistics (BLS) show that in 2014, the rate of overexertion injuries averaged across all industries was 33 per 10,000 full time workers. By comparison, the overexertion injury rate for hospital workers was twice the average (68 per 10,000), the rate for nursing home workers was over three times
- 2. the average (107 per 10,000), and the rate for ambulance workers was over five times the average (174 per 10,000). The single greatest risk factor for overexertion injuries in healthcare workers is the manual lifting, moving and repositioning of patients, residents or clients, i.e., manual patient handling. Patient Handling Ergonomics Occupational safety and health programs have fostered research to identify injury risk factors and safety interventions to prevent injuries during patient handling. Evidence-based research has shown that safe patient handling interventions can significantly reduce overexertion injuries by replacing manual patient handling with safer methods guided by the principles of “Ergonomics.” Ergonomics refers to the design of work tasks to best suit the capabilities of workers. In the case of patient handling, it involves the use of mechanical equipment and safety procedures to lift and move patients so that health care workers can avoid using manual exertions and thereby reduce their risk of injury. At the same time, patient handling ergonomics seeks to maximize the safety and comfort of patients during handling. Patient Handling and the Revised NIOSH Lifting Equation (RNLE) One question that has been raised about patient handling is, “How much weight can be safely lifted without using assistive equipment?” When it comes to questions about lifting, many safety professionals rely on the Revised NIOSH Lifting Equation (https://www.cdc.gov/niosh/docs/94-110/pdfs/94-110.pdf) (RNLE). NIOSH researchers developed the RNLE to determine weight limits for preventing back injuries caused by manually lifting objects on the job. Research studies have validated the equation’s usefulness for computing safe weight limits when lifting inanimate objects such as boxes and other packages. As a matter of policy, NIOSH recommends its use for that purpose. The RNLE is not intended to be used for determining safe weight limits when lifting people. The shape and size of the human body differ from person to person, and patient handling situations are often complicated by many other factors such as the potential for unpredictable movements, the patient’s medical condition, and so on. Since the equation was designed to be used for more stable and predictable lifting tasks, it is generally considered to be impractical for patient handling tasks. As the field of safe patient handling grew over the years, practitioners increasingly expressed interest in trying to determine how much weight can be lifted safely using manual methods, and how much weight requires using lifting equipment. Dr. Thomas Waters examined the issue further and published an article entitled, “When is it Safe to Manually Lift a Patient?” (http://www.asphp.org/wp- content/uploads/2011/05/When_Is_It_Safe_To_Manually_Lift_A_Patient.pdf) . The article describes how the RNLE “can be used to calculate a recommended weight limit for a limited range of patient-handling tasks in which the patient is cooperative and unlikely to move suddenly during the task.” When lifting a box or other inanimate object, the lifter can usually get quite close to the object, which helps minimize strain caused by reaching while lifting. It is usually not possible to get as close when lifting a patient. In order to accommodate the added space needed when lifting a person, Dr. Waters increased the equation’s minimum horizontal distance of 10 inches (between the lifter’s spine and the object) to 14.5 inches (between the 1 2
- 3. lifter’s spine and the patient). After including this change in the equation, he applied the RNLE and determined that under the assumption of an otherwise “ideal” patient handling situation, the maximum recommended weight limit is 35 lbs. Based on Dr. Waters’ calculation, lifting algorithms developed by the Veterans’ Health Administration and the Association of periOperative Nurses state that assistive equipment should be used if the weight to be lifted by any single person exceeds 35 lbs. However, the guidance provided along with the algorithms advises that the 35 lb. limit is not, by itself, sufficiently protective under all circumstances. As explained below, assistive devices are still needed in most situations, even when the weight to be lifted is less than 35 lb. “Limited Guidance” – Not “NIOSH Policy:” Caution regarding the 35 lb. Limit When Dr. Waters derived 35 lb. as the maximum acceptable weight for manual patient handling, his calculation assumed the most ideal, low-risk situation for lifting a person. In his article, “When is it Safe to Manually Lift a Patient?” (http://www.asphp.org/wp- content/uploads/2011/05/When_Is_It_Safe_To_Manually_Lift_A_Patient.pdf) he cautioned that even when the patient is cooperative, many conditions reduce the weight limit even further. These include “lifting with extended arms, lifting when near the floor, lifting when sitting or kneeling, lifting with the trunk twisted or the load off to the side of the body, lifting with one hand or in a restricted space, or lifting during a shift lasting longer than eight hours.” Most patient handling tasks occur under one or more of these circumstances, and certain physical/medical conditions can compromise the patient’s safety during manual handling. Clearly, the majority of patient handling situations are far less than ideal, thus NIOSH cannot designate 35 lb, nor any other weight, as a protective “exposure limit” for patient handling. Instead, NIOSH shares in the consensus among patient handling professionals that the goal of safe patient handling programs should be to eliminate all manual lifting whenever possible. Sources: 1 BLS Table R8. Incidence rates for nonfatal occupational injuries and illnesses involving days away from work per 10,000 full-time workers by industry and selected events or exposures leading to injury or illness, private industry, 2014. (http://www.bls.gov/iif/oshwc/osh/case/ostb4374.pdf) 2 Waters, T., Putz-Anderson, V., Fine, L. [1993]. Revised NIOSH equation for the design and evaluation of manual lifting tasks. Ergonomics, 36, 749-776. Please Note: A Special Section entitled “Impact of Thomas Waters on the Field of Ergonomics,” has been published in Human Factors: The Journal of the Human Factors and Ergonomics Society, August 2016 58:665-795. View the Preface to the Special Section (http://hfs.sagepub.com/content/58/5/665.full.pdf) . This web page contains links to multiple resources for further information on safe patient handling: NIOSH Health Care and Social Assistance Program (HCSA) and the National Occupational Research Agenda (NORA)
- 4. “Healthcare and Social Assistance” (HCSA) is one of many occupational sectors studied by U.S. federal agencies such as the Bureau of Labor Statistics (BLS), The Occupational Safety and Health Administration (OSHA), and the National Institute for Occupational Safety and Health (NIOSH).Guided by NORA-identified research priorities, the mission of the NIOSH HCSA research program is to eliminate occupational diseases, injuries, and fatalities among workers in this sector.Much of this research focuses on safe patient handling. Collaboration among partners in government, industry, and academia has provided a great deal of information on safe patient handling through publications, conferences, and safety training programs.To date, most of the research has focused on the handling of “average-sized” patients in institutional settings such as hospitals and nursing homes. Continued research in these and other settings such as home health care and emergency response, and with obese and morbidly obese (“bariatric”) patients is needed.The research-based evidence gathered thus far has led to the development of safe patient handling standards, and ongoing legislation to enact laws requiring or promoting the use of safe patient handling programs in health care settings. You can use the links and references shown below to find more information on publications, injury data networking, conferences, training programs, standards, and legislation on safe patient handling. NIOSH Publications Safe Lifting and Movement of Nursing Home Residents DHHS (NIOSH) Publication Number 2006-117 (February 2006) State of the Sector Healthcare and Social Assistance Identification of Research Opportunities for the Next Decade of NORA Chapter 11: Musculoskeletal Disorders and Ergonomic Issues DHHS (NIOSH) Publication No. 2009-139 (June 2009) NIOSH Hazard Review: Occupational Hazards in Home Healthcare Chapter 2: Musculoskeletal Disorders and Ergonomic Interventions DHHS (NIOSH) Publication No. 2010-125 (January 2010) Safe Patient Handling Training for Schools of Nursing DHHS (NIOSH) Publication No. 2009-127 (March 2010) NIOSH fast facts: home healthcare workers – how to prevent musculoskeletal disorders DHHS (NIOSH) Publication Number 2012-120 (February 2012) NIOSHTIC-2 Search NIOSHTIC-2 (http://www2a.cdc.gov/nioshtic-2/) is a searchable bibliographic database of occupational safety and health publications, documents, grant reports, and journal articles supported in whole or in part by NIOSH. View search results on Safe Patient Handling (http://www2a.cdc.gov/nioshtic-2/BuildQyr.asp? s1=%27patient+handling%27&f1=*&t1=1&s2=%27patient+lift*%27&f2=*&t2=1&s3=%27lift*+patient*%27&f3=* &t3=1&s4=%27handl*+patient*%27&f4=*&t4=1&s5=lift*+and+patient*&f5=TI&terms=5&Adv=1&n=new&View= b&Startyear=&EndYear=&whichdate=DP&D1=10&Limit=500&Sort=DP+DESC&ct=&B1=Search)
- 5. NIOSH Blogs about Safe Patient Handling Prevention of Back Injuries in Healthcare Settings (http://blogs.cdc.gov/niosh-science-blog/?p=158) Strains, Sprains and Pains in Home Healthcare: Working in an Uncontrolled Environment (http://blogs.cdc.gov/niosh-science-blog/2010/04/16/homehealthcare/) NIOSH Occupational Health Safety Network (OHSN) The OHSN is a secure electronic surveillance system designed to promote analysis and benchmarking of existing occupational health data to prevent injury and illness among healthcare workers. Occupational health staff and workplace safety managers can use OHSN Tools to convert data to OHSN format, then upload without worker identifiers to the secure web portal. Current modules focus on traumatic injuries among healthcare workers including musculoskeletal injuries from patient handling events; slips, trips, and falls; and workplace violence. Other Resources American Association for Safe Patient Handling and Movement (AASPHM) (http://aasphm.org/) AASPHM: Healthcare Recipient Sling and Lift Hanger Bar Compatibility Guidelines (http://aasphm.org/wp- content/uploads/AASPHM-Sling-Hanger-Bar-Guidelines-2016.pdf) International Journal of Safe Patient Handling & Mobility (http://www.americanjournalofsphm.com/) (formerly the American Journal of Safe Patient Handling & Movement) American Nurses Association (ANA) Safe Patient Handling and Mobility (http://www.anasphm.org/) Association of Occupational Health Professionals in Healthcare (AOHP) Resource Guide (http://aohp.org/aohp/Portals/0/Documents/ToolsForYourWork/free_publications/Beyond%20Getting%20Starte d%20Safe%20Patient%20Handling%20-%20May%202014.pdf.pdf) Association of periOperative Nurses (AORN) (http://www.aorn.org/) Association of Safe Patient Handling Professionals (ASPHP) (http://www.asphp.org/) Occupational Safety and Health Administration (OSHA) Worker Safety in Hospitals: Safe Patient Handling (https://www.osha.gov/dsg/hospitals/patient_handling.html) Occupational Safety and Health Administration (OSHA) Ergonomics: Guidelines for Nursing Homes (https://www.osha.gov/ergonomics/guidelines/nursinghome/index.html) Safe Patient Handling in Washington State (http://www.washingtonsafepatienthandling.org/) Upcoming Conferences 2 National Bariatric SPHM Conference, September 14-15, 2017, Austin, TX. http://bariatricsphmconference.com/ (http://bariatricsphmconference.com/) Human Factors and Ergonomics in Health Care 2018 International Symposium, March 26-28, 2018, Boston Marriott Copley Place Hotel, Boston, MA nd
- 6. https://www.hfes.org/web/HFESMeetings/2018HCSCallforproposals.html (https://www.hfes.org/web/HFESMeetings/2018HCSCallforproposals.html) 2018 Safe Patient Handling & Mobility/Falls Conference: Featuring content on Mobility-related Adverse Events, April 16-20, 2018, Rosen Centre, Orlando, FL http://www.tampavaref.org/conferences.ht (http://www.tampavaref.org/conferences.htm) 1 International Conference on Safe Patient Handling and Mobility, September 5-7, 2018, Hyatt Regency, Atlanta, GA https://sphmjournal.com/save-date-1st-international-sphm-conference-september-5-7-2018/ (https://sphmjournal.com/save-date-1st-international-sphm-conference-september-5-7-2018/) National Safe Patient Handling Standards One of the goals established by the NORA Healthcare and Social Assistance (HCSA) Sector Council was for organizations to establish national standards to guide a reduction in musculoskeletal disorders in healthcare workers. The American Nurses Association (ANA) facilitated this effort with several Council members and other interprofessional national subject matter experts, reaching across the continuum of care. On June 26, 2013, ANA released Safe Patient Handling and Mobility Interprofessional National Standards (http://www.anasphm.org/) . For more information about the NORA HCSA Sector Council’s involvement in this and other activities, contact the NORA coordinator at noracoordinator@cdc.gov (mailto:noracoordinator@cdc.gov). Safe Patient Handling Program Implementation: Free Tools and Resources from The Veterans Health Administration (VHA) The VHA provides toolkits that contain comprehensive information related to developing and maintaining safe patient handling programs. These toolkits (http://www.tampavaref.org/safe-patient-handling.htm) include guidance and templates that are being used in VHA hospitals for patient assessment, equipment selection, policy development, program coordination and management, training, and program assessment. They also include algorithms that can be used to maximize safety while handling and mobilizing all patients, with extra guidance specific to “patients of size,” i.e., “bariatric” patients. Easy access to the algorithms and other tools is now available on a free mobile app (https://mobile.va.gov/app/safe-patient-handling) . Safe Patient Handling Legislation in the USA Safe patient handling legislation has been introduced in numerous states and at the federal level. At the state level, the following safe patient handling laws have been enacted: California Labor Code Section 6403.5 signed into law On October 7, 2011 Illinois Public Act 97-0122 signed into law on July 30, 2011 New Jersey S-1758/A-3028 signed into law January 2008 Minnesota HB 712.2 signed into law May 2007 Maryland SB 879 signed into law April 2007 Rhode Island House 7386 and Senate 2760, passed on July 7, 2006 Hawaii House Concurrent Resolution No. 16 passed on April 24, 2006 st
- 7. Washington House Bill 1672 signed into law on March 22, 2006 Ohio House Bill 67, Section 4121.48 signed into law on March 21, 2006 New York companion bills A11484, A07836, S05116, and S08358 signed into law on October 18, 2005 Texas Senate Bill 1525 signed into law on June 17, 2005 To date, no federal safe patient handling law has yet been enacted. The most recently introduced federal bill is the Nurse and Health Care Worker Protection Act of 2015 (H.R.4266 (https://www.congress.gov/bill/114th- congress/house-bill/4266/text? q=%7B%22search%22%3A%5B%22%5C%22hr4266%5C%22%22%5D%7D&resultIndex=1) and S.2408 (https://www.congress.gov/bill/114th-congress/senate-bill/2408/text? q=%7B%22search%22%3A%5B%22%5C%22s2408%5C%22%22%5D%7D&resultIndex=1) ). Read “Preventing Back Injuries in Health Care Settings (http://blogs.cdc.gov/niosh-science- blog/2008/09/22/lifting/)” on the NIOSH Science Blog and share your comments. Related Topics Ergonomics and Musculoskeletal Disorders Health Care Workers Follow NIOSH Facebook (http://www.facebook.com/NIOSH) Flickr (http://www.flickr.com/photos/NIOSH) Pinterest (http://www.pinterest.com/cdcgov/workplace-safety-and-health/) Twitter (http://twitter.com/NIOSH) YouTube (http://www.youtube.com/user/NIOSHSafetyVideos) NIOSH Homepage NIOSH A-Z Workplace Safety & Health Topics Publications and Products Programs Contact NIOSH
- 8. (https://www.cdc.gov/Other/plugins/#pdf) File Formats Help: How do I view different file formats (PDF, DOC, PPT, MPEG) on this site? (https://www.cdc.gov/Other/plugins/) Page last reviewed: August 2, 2013 Page last updated: December 4, 2017 Content source: National Institute for Occupational Safety and Health (http://www.cdc.gov/niosh) Division of Applied Research and Technology