
Recommended
More Related Content
Similar to Bloody Diarrhea and Anemia: A Case of Amebic Colitis
Similar to Bloody Diarrhea and Anemia: A Case of Amebic Colitis (20)
Recently uploaded
Recently uploaded (20)
Bloody Diarrhea and Anemia: A Case of Amebic Colitis
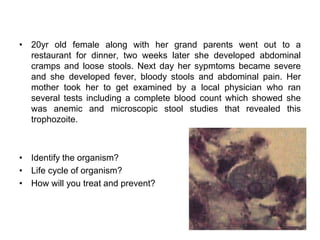
- 1. • 20yr old female along with her grand parents went out to a restaurant for dinner, two weeks later she developed abdominal cramps and loose stools. Next day her sypmtoms became severe and she developed fever, bloody stools and abdominal pain. Her mother took her to get examined by a local physician who ran several tests including a complete blood count which showed she was anemic and microscopic stool studies that revealed this trophozoite. • Identify the organism? • Life cycle of organism? • How will you treat and prevent?
- 2. INTRODUCTION • Entamoeba histolytica is a parasite of global distribution but most of the morbidity and mortality from amebiasis occurs in developing countries. • The total burden of disease caused by E. histolytica is unknown, however roughly 2% of life-threatening diarrhea in children ages 12 to 23 months of age.
- 3. • There are three species of intestinal amebae with identical morphologic characteristics: E. histolytica, E. dispar, and E. moshkovskii • E. dispar and E. moshkovskii are non-pathogenic and do not cause clinical disease.
- 4. • E. histolytica has a simple, 2-stage life cycle that consists of an infectious cyst and a motile trophozoite. • The cyst form measures 5 to 20 μm in diameter and contains 4 or fewer nuclei. • The ameboid trophozoite, which is responsible for tissue invasion, measures 10 to 60 μm and contains a single nucleus with a central karyosome
- 5. • The cysts are relatively resistant to chlorination and desiccation, and they can survive in a moist environment for several weeks.
- 7. • Infection occurs following ingestion of cysts in fecally contaminated food or water. • Within the lumen of the small intestine, the quadrinucleate cyst undergoes nuclear then cytoplasmic division, giving rise to eight trophozoites.
- 8. • Only about 10% of infected persons develop invasive disease characterized by invasion of the colonic epithelium by trophozoites. • Trophozoites that gain access to the bloodstream can spread hematogenously to establish infection at distant sites .
- 9. • Why some persons develop invasive disease and others remain asymptomatic remains a mystery; parasite and host differences are likely to be important in this regard.
- 10. PATHOGENESIS • After excystation within the lumen of the small intestine, trophozoites adhere to colonic mucins and epithelial cells, largely via an amebic galactose/N-acetyl-d- galactosamine inhibitable surface lectin.
- 11. • Secreted cysteine proteinases then facilitate tissue invasion by degrading human colonic mucus and extracellular matrix proteins.
- 12. • Further disruption of the colonic epithelium results directly from contact-dependent cytolysis of epithelial and immune cells • and from an acute epithelial cell inflammatory response with recruitment of neutrophils and immune-mediated tissue damage.
- 13. Fig. 113.2 Model for stepwise invasion of the colonic mucosa by Ent amoeba histolytica. Following excystation, trophozoites (blue) adhere to colonic mucins, and degradation of mucus by amebic proteinases enables contact with the epithelium. Contact-dependent killing of epithelial cells and activation of an epithelial cell response marked by pro- inflammatory cytokine release follow. Amebapore is a protein that forms ion channels or pores in lipid membranes and depolarizes target cells, thus contributing to the virulence of the trophozoite. Activation of pro-interleukin (IL)-1β by amebic cysteine proteinases, with resulting recruitment of neutrophils, further contributes to tissue damage. NFκβ, nuclear factor kappa beta. (From Huston CD. Parasite and host con tributions to the pathogenesis of amebic colitis. Trends Parasitol 2004; 20:23-6.
- 14. • The cecum and ascending colon are affected most commonly, although in severe disease the entire colon may be involved. • On gross examination, pathology can range from mucosal thickening to multiple punctate ulcers with normal intervening tissue to frank necrosis.
- 15. • For unknown reasons, the downward invasion of amebic trophozoites often is halted at the level of the muscularis mucosa.
- 20. • Subsequent lateral spread of amebae undermines the overlying epithelium, resulting in the clean-based, flask- shaped ulcers that characterize amebic colitis. • Early in infection, an influx of neutrophils is typical, but in well-established ulcers, few inflammatory cells are seen.
- 21. • Organisms may be seen ingesting red blood cells (erythrophagocytosis). • At distant sites of infection (e.g., liver abscess), similar pathologic characteristics include central liquefaction of tissue surrounded by a minimal mononuclear cell infiltrate
- 22. • Because more than 90% of persons colonized with E. histolytica spontaneously clear the infection within a year, an effective immune response to amebiasis seems to develop. • Children with fecal anti-amebic lectin immunoglobulin (Ig)A have short-lived protection from subsequent intestinal infection.
- 23. • The protective role of secretory IgA is not certain, however, and the contributions of humoral and cellular immunity to protection from amebiasis remain unknown.
- 24. • Nearly everyone with invasive amebiasis develops a systemic and a mucosal humoral immune response. • Antibodies alone are unable to clear established infection, however, because asymptomatic cyst passers remain infected for months after anti-amebic antibodies develop.
- 25. CLINICAL FEATURES • Infection with E. histolytica results in one of three outcomes. • Approximately 90% of infected persons remain asymptomatic.
- 26. • The other 10% of infections result in invasive amebiasis characterized by dysentery (amebic colitis) or, in a minority of cases, extraintestinal disease (most commonly amebic liver abscess.
- 28. • The major diagnostic challenge for the clinician seeing a patient with amebic colitis is to distinguish the illness from other causes of bloody diarrhea.
- 29. • The differential diagnosis includes the causes of bacterial dysentery, such as Shigella, Salmonella, and Campylobacter species and enteroinvasive or enterohemorrhagic Escherichia coli, and noninfectious diseases, including inflammatory bowel disease, and ischemic colitis.
- 30. • In contrast to bacterial dysentery, which typically begins abruptly, amebic colitis begins gradually over one to several weeks • Although more than 90% of patients with amebic colitis present with diarrhea, abdominal pain can occur without diarrhea; abdominal pain, tenesmus, and fever are highly variable.
- 31. • Weight loss is common because of the chronicity of the illness. Microscopic blood is present in the stool of most patients with amebic dysentery.
- 33. • The most feared complication of amebic dysentery, acute necrotizing colitis with toxic megacolon, occurs in 0.5% of cases. • This complication manifests as an acute dilatation of the colon, and 40% of patients die from sepsis unless it is promptly recognized and treated surgically.
- 34. • Unusual complications include the formation of enterocutaneous, rectovaginal, and enterovesicular fistulas and ameboma. • Ameboma, due to intraluminal granulation tissue, can cause bowel obstruction and mimic carcinoma of the colon.
- 35. • Although a history of dysentery early in the illness is common, dysentery has resolved in most patients by the time of presentation • Extraintestinal sites of infection are involved and typically result either from direct extension of liver abscesses (e.g., amebic pericarditis or lung abscess) or from hematogenous spread of disease (e.g., brain abscess)
- 36. DIAGNOSIS • The gold standard for diagnosis of amebic colitis remains colonoscopy with biopsy, • colonoscopy should be performed whenever infectious causes of bloody diarrhea are strong considerations in the differential diagnosis of ulcerative colitis.
- 37. • Because the cecum and ascending colon are affected most often, colonoscopy is preferred to sigmoidoscopy. • Identification of amebae can be aided by periodic acid– Schiff staining of biopsy tissue, which stains trophozoites magenta.
- 38. • Stool examination for ova and parasites, the traditional method for diagnosing amebiasis, should not be relied upon. • Although the presence of amebic trophozoites with ingested erythrocytes strongly correlates with E. histolytica infection, these rarely are present.
- 39. • and in the absence of hematophagous trophozoites, microscopy cannot distinguish E. histolytica from E. dispar. • Noninvasive methods to accurately differentiate E. histolytica from E. dispar include stool culture with isoenzyme analysis
- 40. • serum amebic-antibody titers, PCR, and an enzyme- linked immunosorbent assay (ELISA) that detects the amebic lectin antigen in stool samples • Of these, only serum amebic-antibody titers and the stool ELISA are widely available for clinical use.
- 41. • Because serum anti-amebic antibodies do not develop in patients infected with E. dispar, serologic tests for amebiasis accurately distinguish E. histolytica and E. dispar infection. • From 75% to 85% of patients with acute amebic colitis have detectable anti-amebic antibodies on presentation, and convalescent titers develop in more than 90% of patients.
- 42. • For amebic liver abscess, 70% to 80% of patients have detectable antibody titers on presentation, and convalescent titers develop in more than 90% of patients. • Antiamebic antibodies can persist for years, however, a positive result must be interpreted with caution.
- 44. • Because approximately 10% of asymptomatic cyst passers develop invasive amebiasis, E. histolytica carriers should be treated. • For non-invasive disease, treatment with a luminal agent alone is adequate (e.g., paromomycin 25 to 35 mg/kg/ day in 3 divided doses for 7 days).
- 45. • Patients with amebic colitis should first be treated with an oral nitroimidazole (either metronidazole [500-750 mg 3 times daily for 10 days] or tinidazole [2 g once daily for 3 to 5 days]) to eliminate invasive trophozoites.
- 46. • Metronidazole and tinidazole are believed to be less effective against organisms in the colonic lumen, and subsequent treatment with a luminal agent such as paromomycin is recommended to prevent recurrent disease
- 47. Prevention • Water can be made safe for drinking and food preparation by boiling it for 1 minute, by halogenation (with chlorine or iodine), or by filtration. • Naturally acquired immunity to intestinal amebiasis provides short-lived protection against reinfection, giving hope that a vaccine may be feasible.
- 48. Other Amebae • Nine other amebae species commonly infect the human GI tract. These include 1. E. dispar, 2. Entamoeba moshkovskii, 3. Entamoeba bangladeshi, 4. Entamoeba coli, 5. Entamoeba hartmanni, 6. Entamoeba gingivalis, 7. Entamoeba polecki, 8. Endolimax nana, and 9. Iodamoeba butschlii.
- 49. • With the exception of E. gingivalis, which has no known cyst stage, all of these true amebae have simple 2-stage life cycles, consisting of an infectious cyst form and a motile trophozoite form. • E. dispar is a nonpathogenic protozoan parasite that is morphologically indistinguishable from Entamoeba histolytica by light microscopy.
- 50. • infection with E. dispar is approximately 10 times more prevalent than E. histolytica infection. • Although E. dispar has been demonstrated to cause mucosal ulcerations in animal models, it has not been demonstrated to cause human disease and does not require treatment.
- 51. • Entamoeba moshkovskii, indistinguishable from E. dispar and E. histolytica except that trophozoites of E. histolytica might show erythrophagocytosis. • its causation of human disease is still controversial, infection by E. moshkovskii is associated with diarrhea in infants.
- 52. • Entamoeba coli trophozoites contain a single nucleus with a prominent karyosome that usually is eccentric in location, distinguishing them from E. histolytica and E. dispar trophozoites, which have a centrally located karyosome. • Entamoeba coli is nonpathogenic and requires no specific treatment
- 53. • E. gingivalis is the only ameba found in the oral cavity, where it lives in the anaerobic environment of the gingival crease. • The trophozoite is identical in size to that of E. histolytica and contains a single nucleus with a prominent central karyosome.
- 54. • oral-oral contact is believed to be its mode of transmission. • E. gingivalis is associated with poor dental hygiene and periodontal disease • The increased frequency of colonization in this setting might simply reflect a hospitable host environment.
- 55. • E. gingivalis often is associated with periodontal disease in AIDS patients, however, and treatment with metronidazole has been reported to be effective.
- 56. • E. polecki, characterized by a uninucleated cyst, is primarily a parasite of pigs and monkeys that sometimes infects humans. • It has been suggested that several distinct uninucleated cystproducing Entamoeba species can infect humans, and it has been proposed that these organisms collectively be termed “E. polecki-like”.
- 57. • At present, specific treatment of E. polecki-like infections is not routinely recommended, but persons with heavy burdens of this parasite can develop nonspecific GI symptoms and might benefit from treatment. • Good clinical responses to metronidazole and diloxanide furoate have been reported.
- 58. • Endolimax nana is a nonpathogenic intestinal ameba that often infects humans. • Distribution is most common in the tropics, where 5% to 33% of persons are infected. • Infection requires no specific treatment, but it serves as a useful marker for fecal-oral exposure.