2016 indicator reference guide priority pop prevention services
•
0 likes•16 views

2016 indicator reference guide priority pop prevention services

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to 2016 indicator reference guide priority pop prevention services
Similar to 2016 indicator reference guide priority pop prevention services (20)
More from #GOMOJO, INC.
More from #GOMOJO, INC. (20)
Recently uploaded
Recently uploaded (20)
2016 indicator reference guide priority pop prevention services
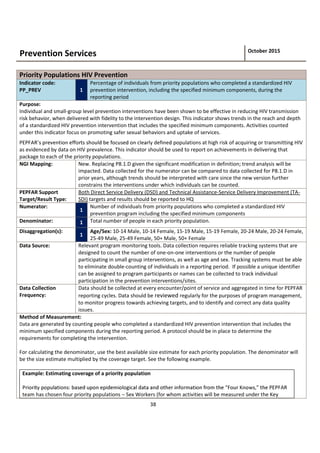
- 1. 38 Prevention Services October 2015 Priority Populations HIV Prevention Indicator code: PP_PREV 1 Percentage of individuals from priority populations who completed a standardized HIV prevention intervention, including the specified minimum components, during the reporting period Purpose: Individual and small-group level prevention interventions have been shown to be effective in reducing HIV transmission risk behavior, when delivered with fidelity to the intervention design. This indicator shows trends in the reach and depth of a standardized HIV prevention intervention that includes the specified minimum components. Activities counted under this indicator focus on promoting safer sexual behaviors and uptake of services. populations at high risk of acquiring or transmitting HIV as evidenced by data on HIV prevalence. This indicator should be used to report on achievements in delivering that package to each of the priority populations. NGI Mapping: New. Replacing P8.1.D given the significant modification in definition; trend analysis will be impacted. Data collected for the numerator can be compared to data collected for P8.1.D in prior years, although trends should be interpreted with care since the new version further constrains the interventions under which individuals can be counted. PEPFAR Support Target/Result Type: Both Direct Service Delivery (DSD) and Technical Assistance-Service Delivery Improvement (TA- SDI) targets and results should be reported to HQ Numerator: 1 Number of individuals from priority populations who completed a standardized HIV prevention program including the specified minimum components Denominator: 1 Total number of people in each priority population. Disaggregation(s): 1 Age/Sex: 10-14 Male, 10-14 Female, 15-19 Male, 15-19 Female, 20-24 Male, 20-24 Female, 25-49 Male, 25-49 Female, 50+ Male, 50+ Female Data Source: Relevant program monitoring tools. Data collection requires reliable tracking systems that are designed to count the number of one-on-one interventions or the number of people participating in small group interventions, as well as age and sex. Tracking systems must be able to eliminate double-counting of individuals in a reporting period. If possible a unique identifier can be assigned to program participants or names can be collected to track individual participation in the prevention interventions/sites. Data Collection Frequency: Data should be collected at every encounter/point of service and aggregated in time for PEPFAR reporting cycles. Data should be reviewed regularly for the purposes of program management, to monitor progress towards achieving targets, and to identify and correct any data quality issues. Method of Measurement: Data are generated by counting people who completed a standardized HIV prevention intervention that includes the minimum specified components during the reporting period. A protocol should be in place to determine the requirements for completing the intervention. For calculating the denominator, use the best available size estimate for each priority population. The denominator will be the size estimate multiplied by the coverage target. See the following example. Example: Estimating coverage of a priority population team has chosen four priority populations Sex Workers (for whom activities will be measured under the Key
- 2. 39 Populations indicator), migrant mine workers in three districts, out-of-school girls aged 15-24 in 25 peri-urban areas, boys 14 25 targeted for VMMC. Package of interventions: together with the IP, the team designs a set of interventions for each of these groups that include the minimum components required in this indicator, tailored to the population. Size estimation: the team also estimates the size of each of the populations in each of the geographic zones where the IP will implement. Geographic zones are chosen based upon epidemiological data with care to prevent duplication of service support with other donors. In our example, size estimations for migrant miners might be 10,000 in District 1; 8,000 in District 2; and 4,000 in District 3 (based upon a recent report from the International Organization for Migration). Target setting: the team sets a coverage target for each population, with a goal of saturating that population to reach impact. Using our example of migrant mine workers, the team might decide to shoot for 80% coverage of each population, making the target for district 1, 8,000 reached; for district 2, 6,400 reached; and district 3 3,200 reached. The total target for this population would be 17,600. Reporting: At the APR, the team will report a single number to PEPFAR headquarters, which is the sum of all members of each priority population reached in the reporting period with the full package. So if the programs reached 18,000 migrant mine workers, 20,000 out of school girls and 33,000 boys, the number would be 71,000. This total would be disaggregated and reported by sex by age. In the APR narrative, the team would further disaggregate the results by priority population, and describe progress made toward coverage goals for each one. Note that sex workers would not be included in this total even though they are a priority population, as they are Calculating percentage of priority population reached: Numerator = number of target population reached (for our miner example, this would be 18,000) Denominator = Total priority population size (for the miner example, 22,000) Note that it will be important for the team to also perform this calculation for each district or distinct subset of the population. In our migrant mine worker example, this means calculating coverage for each district, to learn whether coverage targets were met for each district and adjust performance plans accordingly. Explanation of Numerator: The numerator is the number of individuals from each priority population who completed a standardized HIV prevention program, including the specified minimum components during the reporting period. For the purposes of the APR, the team will sum the numbers reached in each of the priority populations and report that total. For the purposes of tracking coverage more meaningfully at the regional, national or sub-national level, the team will track this indicator separately for each priority population. Priority population: PEPFAR-funded programs will identify priority populations for HIV prevention in their COPs and will report on these populations within this indicator. Please note that priority populations will include "Other Vulnerable Populations." Groups that might be counted in the category of Other Vulnerable Populations include the following and should always be selected on the basis of available epidemiological data:" o Clients of sex workers o Military and other uniformed services o Incarcerated persons o Mobile populations (e.g., migrant workers, truck drivers) o Non-injecting drug users Delivery of prevention packages for all priority populations will be tracked with this indicator, with the exception of
- 3. 40 packages for key populations as defined by UNAIDS and WHO: sex workers, men who have sex with men/transgender, KP Standardized HIV Prevention Intervention is defined as an activity or set of activities designed for a specific priority population to reduce HIV transmission that is implemented the same way each time. These interventions adhere to written protocols, include goals and activities tailored to the priority population, typically comprise multiple encounters with the same individuals or small groups, and have a system for tracking and reporting the completion of every element of the intervention. Minimum components: Every intervention for adult populations must include all of these components: 1. Targeted risk assessment and provision of risk reduction information, education and/or counseling to correctly identify HIV prevention methods, reject misconceptions about HIV transmission, and accurately gauge and personalize risk for HIV infection. 2. Condom promotion, condom skills training including negotiation skills and facilitated access to condoms whether through direct provision, linkages to social marketing outlets or other means (or referrals for condom promotion, provision and related skill development)9 . 3. Informational sessions on HIV testing and counseling with active referrals to or provision of HTC services. 4. Demand creation to increase awareness, uptake and acceptability of relevant clinical services such as voluntary medical male circumcision (VMMC), prevention of mother-to-child transmission (PMTCT), HIV care and treatment, TB testing and treatment and reproductive health. 5. Activities which: promote gender equitable principles; address harmful norms related to sex and gender; and seek to reduce stigma and discrimination associated with HIV; and prevent gender-based violence. Every intervention for youth populations must include all of these components: 1. Targeted risk assessment and provision of risk reduction information, education and/or counseling to correctly identify HIV prevention methods, reject misconceptions about HIV transmission and increase perception of risk for HIV infection. 2. Curriculum-based, age-appropriate, HIV prevention skills and sexuality education to prevent HIV acquisition and encourage safer sex strategies for sexually active youth. 3. Informational sessions on HIV testing and counseling with active referrals to or provision of youth-friendly HTC services. 4. Community programs targeting adults to raise awareness of HIV risks for young people, promote positive parenting and mentoring practices, and effective adult-child communication about sexuality and sexual risk reduction. 5. Demand creation to increase awareness, uptake and acceptability of youth-friendly clinical services such as voluntary medical male circumcision (VMMC), HIV care and treatment, and TB testing and treatment. 6. Condom promotion, condom skills training including negotiation skills and facilitated access to condoms whether through direct provision, linkages to social marketing outlets or other means (or referrals for condom promotion, provision and related skill development1 for sexually active youth. 7. Activities which: promote gender equitable principles; address harmful norms related to sex and gender; and seek to reduce stigma and discrimination associated with HIV and to prevent gender-based violence. Standardization and documentation allows public health professionals to evaluate program outcomes. The best interventions are often identified through a series of efficacy reviews. National Efficacy Review Criteria should be developed for HIV prevention programs in each country. Technical assistance should be provided to national and local prevention programs to document, evaluate, and standardize HIV prevention interventions designed to reach a specific 9 PEPFAR may fund prevention programs that do not provide or refer for condom promotion and provision. These programs may not be counted under this indicator.
- 4. 41 target population to ensure efficacious interventions are implemented and reported. Explanation of Denominator: The denominator is the estimated number of individuals in the priority population. Whenever possible, size estimates for the population should be done at the level of implementation to allow for real- time tracking of coverage. These lower level estimates can be aggregated for national tracking of coverage. See example earlier in this reference sheet for more detail. The data tracked at the national level should be disaggregated by each priority population. Success in achieving coverage of each priority population should be described in the narrative accompanying the reporting of results in the APR. Interpretation: When measured over time and disaggregated, this indicator can demonstrate progress towards achieving coverage of priority populations with a minimum package of validated HIV prevention interventions. In shorter time frames, the information collected with this indicator can be used to assess progress towards program-specific goals and to make management decisions to facilitate progress towards those goals. When calculating the percent of a population who completed a standardized HIV prevention intervention during the reporting period, the indicator will represent PEPFAR coverage only. National or other donor programs may be implemented and not represented in this indicator. This indicator does NOT capture the impact of HIV prevention programs on incidence. Teams are encouraged to conduct impact evaluations of specific programs using incidence or other contextually appropriate outcome measures to determine whether programs are reducing transmission of HIV. PEPFAR Support: DSD: Individuals will be counted as receiving direct service delivery support from PEPFAR when BOTH of the below conditions are met: Provision of key staff or commodities AND frequent, at least quarterly, support to improve the quality of services. TA-SDI: Individuals will be counted as supported through TA-SDI when the point of service delivery receives support from PEPFAR that meets the second criterion only: Frequent, at least quarterly support to improve the quality of services. 1. PEPFAR is directly interacting with the patient or beneficiary in response to their health (physical, psychological, etc.) care needs by providing key staff and/or essential commodities for routine service delivery. For priority populations receiving HIV prevention services, this can include ongoing procurement of critical commodities such as condoms, teaching materials, or community promotion materials, or funding for salaries of personnel who deliver components of the intervention or paying for transportation of those staff to the point of service delivery. Staff who are responsible for the completeness and quality of routine patient records (paper or electronic) can be counted here; however, staff who exclusively fulfill MOH and donor reporting requirements cannot be counted. AND/OR 2. PEPFAR provides an established presence at and/or routinized frequent (at least quarterly) support for those prevention services at the point of service delivery. For HIV prevention among priority populations, this ongoing support for service delivery improvement can include: site supervision, training or assistance with monitoring and evaluation, support for quality improvement activities, and development of materials and protocols. Additional References: HIV P3, HIV-P4b. The Global Fund to Fight AIDS, Tuberculosis and Malaria Monitoring and Evaluation Toolkit 4th Edition. November 2011. (http://www.theglobalfund.org/en/me/documents/toolkit/)