Persistent PTSD among Patients with Fragile X Syndrome: Case Series
SLC6A4 COMT and Deregulation of the Prefrontal -10-6-15-36x30
1. SLC6A4, COMT and Deregulation of the Prefrontal Cortex in PTSD
Laura Viner, Jesse Viner, Leah Klein, and Emily Rose Kirschenbaum
Psychiatry and Behavioral Sciences, Northwestern University Medical School, and Yellowbrick
Growing evidence suggests that there are
complex and dynamic interactions
between genetic and environmental
factors in the vulnerability to PTSD. The
genes involved in neuro-transmitter
regulation of emotion processing and
response networks have been proposed as
candidate genes for investigating
vulnerability to PTSD, with
environmental exposure to trauma.
SLC6A4 and COMT are two such
candidate genes in that they have each
been shown to alter brain function in the
emotion-regulating regions associated
with primary symptoms of PTSD,
especially negative attention and affective
bias. SLC6A4 is a serotonin transporter
gene that affects brain function in the
emotion-regulating regions of the
amygdala and prefrontal cortex. COMT is
responsible for dopamine modulation in
the prefrontal cortex and hippocampus.
Both genes have polymorphisms
associated with either vulnerability to, or
resilience against, PTSD when exposed to
trauma. The homozygous s/s variant of
the SLC6A4 gene, and the met/met
homozygous variant of the COMT gene,
have both been linked to a greater risk of
PTSD with the experience of trauma.
Such findings have been somewhat
inconsistent in the literature, and recent
studies have suggested that those
inconsistencies may be the result of
complex interactions between genetic and
environmental factors, and with different
populations of PTSD and trauma
survivors studied.
The present study examined the
relative association of the two
homozygous alleles of SLC6A4 (s/s and
l/l) and COMT (met/met and val/val)
among survivors of sexual and
physical trauma, with or without
PTSD, and the corresponding neuro-
physiological deregulation of the
prefrontal cortex.
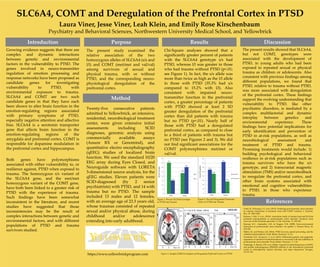
Chi-Square analyses showed that a
significantly greater percent of patients
with the SLC6A4 genotype s/s had
PTSD, whereas l/l was greater in those
who had trauma without PTSD (p<.01;
see Figure 1). In fact, the s/s allele was
more than twice as high as the l/l allele
in those with PTSD (35.3% had s/s
compared to 15.2% with l/l). Also
consistent with impaired neuro-
transmitter function in the prefrontal
cortex, a greater percentage of patients
with PTSD showed at least 2 SD
greater deregulation of the prefrontal
cortex than did patients with trauma
but no PTSD (p<.01). Nearly half of
those with PTSD had a deregulated
prefrontal cortex, as compared to close
to a third of patients with trauma but
no PTSD (see Figures 2 and 3). We did
not find significant associations for the
COMT polymorphisms met/met or
val/val.
The present results showed that SLC6A4,
but not COMT, genotypes were
associated with the development of
PTSD, in young adults who had been
exposed to repeated sexual or physical
trauma as children or adolescents. Also
consistent with previous findings among
different populations, we found that
PTSD, relative to trauma without PTSD,
was more associated with deregulation
of the prefrontal cortex. These findings
support the evolving understanding that
vulnerability to PTSD, like other
psychiatric disorders, is mediated by a
complex multifactorial and dynamic
interplay between genetics and
environmental experience. These
findings have potential implications for
early identification and prevention of
PTSD in at-risk populations, as well as
neurobiological assessment and
treatment of PTSD and trauma.
Promising treatments would include: 1)
building psychological and behavioral
resilience in at-risk populations such as
trauma survivors who have the s/s
genotype, and 2) transcranial magnetic
stimulation (TMS) and/or neurofeedback
to reregulate the prefrontal cortex, and
other brain systems associated with
emotional and cognitive vulnerabilities
to PTSD, in those who experience
trauma.
Introduction Purpose Results Discussion
Twenty-five consecutive patients
admitted to Yellowbrick, an intensive,
residential, neurobiological treatment
center, were given extensive initial
assessments including SCID
diagnoses, genomic analysis using
commercially available assays
(Assure RX or Genomind), and
quantitative electro encephalography
(qEEG) studies of localized brain
function. We used the standard 10/20
EEG array during Eyes Closed, and
Neuroguide software with LORETA
3-dimensional source analysis, for the
qEEG studies. Eleven patients were
SCID-diagnosed (by 2 senior
psychiatrists) with PTSD, and 14 with
trauma but no PTSD. The sample
included 13 males and 12 females,
with an average age of 23.3 years old,
whose traumas consisted of repeated
sexual and/or physical abuse, during
childhood and/or adolescence
extending into early adulthood.
Method
Clark, R., DeYoung, C.G. et al. (2013). Predicting post-traumatic stress disorder
in veterans: Interaction of traumatic load with COMT variation. J. Psychiat.
Res., 47, 1849-1856.
Kolassa, I. Ertl, V. et al., (2010). Association study of trauma load and SLC6A4
promoter polymorphism in posttraumatic stress disorder: Evidence from
survivors of the Rwandan genocide. J. Clin. Psychiat., 71, 543-547.
Koenan, K.C., Amstadter, A.B., & Nugent, N.R. (2009). Gene-environment
interaction in posttraumatic stress disorder: An update. J. Trauma Stress, 22,
416-426.
Miller, J.K. and Weiner, J.M. (2014). PTSD recovery, spatial processing, and the
val66met polymorphism. Front. Behav. Neurosci., 8, 1-6.
Norrholm, S.D., Jovanovic, T. et al. (2013). Differential genetic and epigenetic
regulation of catechol-O-methyltransferase is associated with fear inhibition in
posttraumatic stress disorder. Front. Behav. Neurosci., 7, 1-10.
Tunbridge, E. Burnet, P.W. et al. (2004). Catechol-O-methyltransferase (COMT)
and proline dehydrogenase (PRODH) mRNAs in the dorsolateral prefrontal
cortex in schizophrenia, bipolar disorder, and major depression. Synapse,
51,112-118.
References
https://www.yellowbrickprogram.com
Figure 1. Percent SLC6A4 Genotype
in PTSD and Trauma
Figure 2. Percent Deregulated Prefrontal
Cortex in PTSD and Trauma
Figure 3. Sample LORETA Analysis of Deregulated Prefrontal Cortex in PTSD
54.8
72.7
45.2
27.3
0
10
20
30
40
50
60
70
80
PTSD Trauma
PercentDeregulated
Regulated
Deregulated
35.3
23.5
15.2
30.3
0
5
10
15
20
25
30
35
40
PTSD Trauma
PercentGenotype
S/S
L/L