HAP 752 Semester Long Project Write-Up Koyin Aladesuru Linkedin
1. 1
Koyin Aladesuru
4/16/2015
HAP 752- AdvancedHealthInformationSystems
Semester Long Project
HIV (Human Immunodeficiency Disease)
Introduction:
There was once upon a time when the word HIV seemed like a taboo, and the mere mention of
the word could have one glance at you with a death sentence stare. HIV, also known as Human
Immunodeficiency Virus, spreads through body fluids that affect vital cells in the immune
system. Without treatment, HIV often leads to AIDS (Acquired Immunodeficiency Syndrome),
an advance stage of HIV that destroys several cells in the body and makes one prone to
opportunistic infections and diseases. HIV can be transmitted through a list of possible risk
factors such as number of sexual partners, condom usage, injection drug users, sexual
orientation, history of STD’s, or even geographical location. According to recent statistics
provided by the Center for Disease Control and Prevention (CDC), there are about 50,000 new
HIV infections per year and approximately 1.2 million people in the United States were living
with HIV at the end of 2011. Fortunately however, with the advancement of antiretroviral
therapy (ART) and proper medical care, HIV is no longer a death sentence. Antiretroviral
therapy, which was introduced in the mid-1990’s, has proven to be a life saver in the fight
against HIV. The goal of this project is to build a system that allows healthcare providers to
conduct a thorough risk assessment for HIV, recommend effective prevention methods, track
lab values for patients, show trend of values over time, detect abnormal results, and identify
adverse drug reactions.
Background:
HIV can be broken up into three stages:
1. Acute infection: This stage is typically within 2 to 4 weeks after infection of HIV, and the
word “acute” implies that this is when one is at the highest risk of spreading the disease.
This is also the period when one may display symptoms such as fever, fatigue, cough,
shortness of breath, sore throat, rash, and enlarge lymph nodes.
2. Clinical latency (inactivity or dormancy): This stage is often referred to as HIV
asymptomatic, where one may display little to no symptoms. Typically, people who are
adherent to antiretroviral therapy during this stage can maintain clinical latency for a
long period of time (usually several decades). Towards the latter end of this stage
however, the viral load (amount of virus in the blood) usually increases, while the CD4 T-
2. 2
cells (white blood cells in the body) begins to drop. The immune systemgets weaker at
this point.
3. AIDS (Acquired Immunodeficiency Syndrome): As the immune system progressively
gets weaker, one becomes severely exposed to opportunistic infections and cancer.
When the CD4 count falls below 200 cells/mm^3, one may be diagnosed as AIDS.
Although, it is important to note that one can also be diagnosed as AIDS once one
develops one or more opportunistic infections, regardless of CD4 count. A normal range
for a CD4 count falls between 500 and 1,200 cells/mm^3. CDC points out that without
treatment, people diagnosed with AIDS survive an average of 3 years life expectancy.
HIV Testing
Know your HIV status- is the recurring mantra that has been floating around our society for
several decades. Risk assessment and routine testing for HIV is very important, particularly
amongst younger adults who may be at a higher risk of exposure. In the public health
community, it is not uncommon to hear that a sexually active person has never been tested for
HIV. ELISA, also known as Enzyme-Linked Immuno Assay, is a widely used laboratory test to
detect HIV antibodies in the blood. It can detect HIV as early as 3 weeks after exposure and if a
patient tests positive, they further undergo a confirmatory test, known as a Western Blot, to
confirm positivity. In order to screen out false-positive results, which happen in rare cases, it is
important to supplement an ELISA test with a Western Blot test. Subsequently, a clinician then
orders a Viral Load and CD4 test which we’ll discuss in the next few sections.
Viral Load
This is a term used to describe the amount of virus in the blood. In clinician language, viral Load
can be described as the number of copies of HIV RNA in a milliliter of blood. In simple terms,
the more HIV spreads in your blood, the higher your viral load. Viral load is a useful metric to
measure the health status of an HIV patient and the impact of antiretroviral therapy on their
health. It is recommended to look at a trend of viral load over time (we will discuss this later on
in the project). Compared to hypertension, diabetes, or some other chronic diseases, HIV does
not necessarily have a specific range/cutoff for a “normal” viral load. According to the Health
Resources and Services Administration (HRSA), viral count can be measured using the following
data criteria:
Suppressed (Undetectable level): < 200 copies/mL
Unsuppressed (Detectable level): > 200 copies /mL
CD4 Count:
CD4 T-cells, also known as “CD4 Count”, are white blood cells that protect the immune system.
A CD4 test measures the amount of T-cells in the body. As the CD4 count decreases, the risk of
developing opportunistic infections increases. As I mentioned earlier, a CD4 count less than 200
cells/mm^3 is considered below normal range and it indicates that HIV is advancing to AIDS.
3. 3
According to the Health Resources and Services Administration (HRSA), CD4 count can be
measured using the following data criteria:
Normal range: 500 – 1,200 cells/mm^3
Below normal range: < 200 cells/mm^3
PrEP:
Pre-exposure prophylaxis, also known as PrEP, is an effective prevention option for people who
are at high risk of getting HIV. CDC recommends PrEP for people who are HIV-negative but are
at substantial risk for the disease. PrEP is taking in the form of a pill called Truvada and is
recommended to be taking daily to prevent HIV. According to a PreP study conducted, the risk
of getting HIV infection was about 92% lower for patients who took Truvada consistently. Part
of this project will explore a scenario where a provider conducts a risk assessment for a patient
recently exposed to HIV, performs an HIV test (which comes back negative), and recommends
PreP as an effective risk reduction method.
ALERTS and Clinical Decision Support Systems (CDSS):
In order for health providers to make accurate and effective clinical decisions, a data system
should be able to trigger a series of alerts or warnings to guide them during treatment. Data
mining helps physicians, nurses, and other health professionals predict the likelihood of an
event occurring. This could range from risk stratification of a particular disease, to disease
management and adverse drug interactions. Keep in mind that it is important not to
overwhelm providers with alerts, particularly for less urgent clinical decisions.
A clinician will be able to achieve the following with this system:
1. Identify patients who are at risk of getting HIV
2. Prescribe PrEP as an effective prevention method
3. Monitor viral load count for HIV positive clients
4. Monitor CD4 count and prescribe PCP Prophylaxis if CD4 count drops below 200
5. Prescribe antiretroviral medications and check for any drug interactions/allergies
6. View a graphical trend of viral load performance
RequirementsSpecification:
Scenario 1
A patient comes in for a routine HIV test. A nurse/community health educator uses a risk
assessment screening tool to measure the patients risk for HIV. Out of 9 standardized
questions, if the patient answers “Yes” to 5 or more, an alert will be triggered as “high risk”.
4. 4
The medical personnel will then perform an HIV (ELISA) test and if the test comes out negative,
a clinician will suggest/prescribe PreP as an effective risk reduction method.
Scenario name: Risk assessment and PrEP prescription
Decision made by the scenario: CDSS will help determine if patient is at substantial risk of
getting HIV and alert the provider to offer PrEP as a preventive option.
Actors: Medical Personnel, Patient
Description: The medical personnel can use the clinical decision support system to conduct a
risk assessment and prescribe PrEP to HIV-negative patients who are high risk of exposure to
HIV.
Use case name: CDSS utilization
Overview: HIV has a high correlation with sexual behaviors. The purpose of this use case is to
identify a patient who is at increased risk of exposure to the disease. If they answer yes to 5 or
more risk assessment questions, a provider will offer the option of PrEP in order to mitigate
their risk.
Primary actor: Medical staff (Phlebotomist, Nurse, Community Health educator)
Secondary actor: Clinicians
Start point: The medical staff performs a risk assessment of patient sexual behaviors. If patient
scores more than 5 out of 9 standardized questions, a “high risk alert” will pop up. Medical
personnel will the recommend an HIV test
End point: The provider reviews lab results and utilizes the clinical decision support systemto
offer PrEP to patient
Information Exchange: The information about potential risk factors is entered into a patient’s
sexual risk assessment screening tool. The provider will use the CDSS tool to identify if the
patient is high risk, perform HIV test, and recommend risk prevention treatment as needed i.e.
PrEP.
Scenario 2:
A patient walks in for a routine HIV test. The medical personnel administer an ELISA test and
the result comes back positive. Provider conducts a confirmatory test (Western Blot) to confirm
positivity. Results come back positive again. Provider then diagnoses patient as HIV (ICD9: 042).
The provider orders lab work which includes a Viral Load and CD4 test. If VL > 200, an alert
triggers “unsuppressed viral load”, and if CD4 < 200, another alert triggers “Below normal
5. 5
range”. Provider uses the CDSS systemto prescribe antiretroviral therapy and to check for any
allergies/drug to drug interaction.
Scenario name: Viral Load Suppression, CD4 monitor, and Drug to Drug interaction
Decision made by the scenario: To find out if an HIV positive patient has a detectable viral load
(VL > 200), a CD4 count < 200, and an adverse drug reaction to antiretroviral therapy. This will
be used to monitor health status of the patient.
Actors: Medical Personnel, Clinician
Description: The medical personnel will draw blood to check if viral load is suppressed, if CD4
count is within normal range, and if there are any adverse drug reactions
Use case name: VL suppression and CD4 normal range
Overview: The purpose of this use case is to routine test see if a patient is HIV positive. HIV test
comes back positive and nurse schedules same day appointment is scheduled for patient to see
provider. Provider diagnoses patient does confirmatory test and diagnoses patient with HIV.
(ICD-9: 042). Orders viral load and CD4 count to check normalcy and check for drug
interactions.
Start point: Nurse, Phlebotomist, or Community Health Educator tests patient for HIV. Results
come back positive. Western blot is performed for confirmatory test. Results come back
positive again.
End Point: Provider diagnoses patient and orders a viral load and CD4 test. Patient results show
that VL level is higher than normal and CD4 is below the normal range. Provider prescribes
antiretroviral therapy to patient. Check for any allergies. Allergy alert triggers and provider
prescribes appropriate medications.
Information Exchange: The information about the patient is entered into the system and the
provider will monitor the patient’s health outcomes over a period of time.
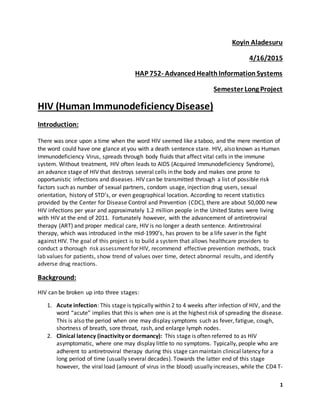
ENTITY RELATIONSHIP DIAGRAM:
7. 7
Implementation:
Scenario 1 Implementation:
HIV Tester and Tracker
Step 1: A provider, nurse or community health educator conducts risk assessment of patient.
Enters patient demographics, and asks a series of 7 standardized questions.
Step 2: If patient answers “yes” to 5 questions or more, an alert will appear indicating the
patient is “high risk”
Step 3: The medical personnel (who could be a nurse, community health worker, or a clinician)
will then recommend an HIV test to the patient in attempt to promote risk reduction efforts
Step 4: HIV ELISA test is performed and noted. Based on the negative result, an alert will appear
indicating the patient is fine but will recommend PrEP for prevention strategy against the
exposure to HIV. Patient accepts recommendation and physician prescribes PreP to be taking
daily. Physician also educates patient about the impact of high risk sexual behaviors.
Scenario 2 Implementation:
Step 1: Patient walks in for HIV test with complaints of having flu-like symptoms. The Medical
personnel perform an HIV test (ELISA). The result comes back positive.
Step 2: The patient is sent to a provider who will conduct a confirmatory test (Western blot) to
make sure this is not a false-positive. The clinician orders the confirmatory test to evaluate true
positivity.
Step 3: The clinician diagnoses the patient with an ICD-9 “042” indicating “HIV”. The clinician
then explains the results to the patient and orders some additional labs to be performed such
as Viral Load, and CD4 tests.
Step 4: The clinician reviews the labs and based on if the values for the viral load are > 200 or
CD4 < 200, an alert will appear indicating an “unsuppressed’ VL and CD4 count “lower than
normal range”.
Step 5: The clinician clicks the “e-prescription” tab in the systemto prescribe antiretroviral
therapy.
Step 6: The clinician uses the CDSS to check for any drug interactions. If patient has any
allergies, an alert will appear indicating that an alternative medication should be prescribed.
Step 7: The clinician puts in prescription order for Stribild and Complera.
9. 9
Based on the patient’s answers to the risk assessment questions, an automatic high risk alert is
triggered.
10. 10
Although the patient tested negative for HIV, there will be another alert indicating a prevention
recommendation for PreP based on the patient’s risk factors.
11. 11
Alternatively, let’s see what happens if a patient tests positive to HIV. All steps listed earlier
should reflect in the following screenshots:
16. 16
CDSS
Conclusion:
CDSS and alerts are very important tools in clinical decision making. Whether it’s checking to
see patients risk stratification, or alerts when labs are abnormal, or when there is an adverse
drug reaction, CDSS proves to be a useful tool in guiding clinicians. This systemimproves the
quality of care, overall patient satisfaction, and ultimately reduces cost for both patient and
provider- achieving the IOM (Institute of Medicine) Triple Aim model. HIV is not a death
sentence and as long as people practice safe sex and monitor their sexual behavior regularly,
their risk significantly diminishes.
References:
1. Center for Disease Control and Prevention. (Jan, 2015). HIV/AIDS. Retrieved from:
http://www.cdc.gov/hiv/basics/whatishiv.html
2. AIDSMap. (July, 2012). HIV/AIDS- sharing knowledge, changing lives. Retrieved from:
http://www.aidsmap.com/Viral-load/page/1327496/
3. AIDS.gov. (March, 2015). HIV/AIDS Basics. Retrieved from: https://www.aids.gov/hiv-
aids-basics/just-diagnosed-with-hiv-aids/understand-your-test-results/viral-load/
17. 17
4. AIDS.gov. (Sep, 2014). HIV/AIDS Basics. Retrieved from: https://www.aids.gov/hiv-aids-
basics/just-diagnosed-with-hiv-aids/understand-your-test-results/cd4-count/
5. Health Resources and Services Administration. (2015). About Ryan White HIV/AIDS
Program. Retrieved from: http://hab.hrsa.gov/abouthab/aboutprogram.html
Entities considered for this prototype:
Field Name Type Data Format Source of Data Intended Use of Data Description
patient_id Number Number
Entered by
front desk
staff
Used to identify patient
records within the
system and paper
records outsidethe
system
Clinic’s internal
patient identifier
(medical record
number); must be
unique to patient
within your
organization
dob
Date/Time Date Entered by
front desk
staff
Used to calculateage
of patient
Patient’s date of
birth
YYYY-MM-DD
gender Text Text
Entered by
front desk
staff
Used to identify patient
by race
Patient’s gender
First_name Text
Entered by
front desk
staff
Used to identify patient
by firstname
Patient's last
(family) name
Last_Name Text Text
Entered by
front desk
staff
Used to identify patient
by lastname
Patient’s, first
(given) name
pcp_id Text Text
Assigned by
front desk
staff
Used to assign patient
to a primary care
physician
ID of the patient’s
primary care
physician (as
indicated in the
"Providers"file)
ethnicity Text Text
Entered by
front desk
staff
Used to identify patient
by ethnicity
Patient’s ethnicity
race Text Text
Entered by
front desk
staff
Used to identify patient
by race
Primary racewith
which patient
identifies.
EncounterID Number 999.9
Generated
usingAccess
database
Used to identify each
unique patient
appointment
Each patient
appointment has
a unique identifier
for querying
purposes
18. 18
ApptDate Date/Time mm/dd/yyyy
Entered by
front desk
staff
Used to identify the
date of appointment
Patient
appointment date
StartTime Date/Time Date/Time
Entered by
front desk
staff
Used to identify the
starttime for each
appointment
Start time for
each appointment
endTime Date/Time Date/Time
Entered by
front desk
staff
Used to identify the
end time for each
appointment
End time for each
appointment
provider_id Text Text
Entered by
front desk
staff
Used to identify the
Primary CarePhysician
for each patient
Provider ID
(correspondingto
the provider
record in the
“Providers”file) of
the provider that
performed the
procedure.
DiagCode Text Text
Entered by
clinician
Used to identify the
ICD-9 diagnosiscodes
associated with each
appointment
The diagnosis
code
nomenclature
used to code the
firstdiagnosis
associated with
the current
procedure.
ICD_Code Text Text
Entered by
clinician
Used to identify
diagnosiscodes and
problem lists
The diagnosis
code
nomenclature
used to code the
diagnosis.
ICD_Description Text Text
Entered by
clinician
Used to identify
diagnosisdescription
The descriptive
label for diagnosis
code.
Lab_date
Date Date Entered by
medical
personnel
Used to identify the
date the lab test was
performed
The date on which
the current
measurement was
taken.
YYYY-MM-
DD
YYYY-MM-DD
19. 19
Lab_ID Integer Integer
Entered by
medical
personnel
Used to identify unique
lab tests in the HER
An identifier used
to uniquely
identify the
observation
within the client’s
EHR/Reporting
System.
LabName Text Text
Entered by
medical
personnel
Used to identify the
name of the lab test
that was administered
The descriptive
label for the type
of observation
being reported
LabValue Text String
Entered by
medical
personnel
Used to identify the lab
result
The raw valueof
the measurement
associated with
the current
observation.
Note: Blood
Pressurecan be
sent as one
“systolic/diastolic”
stringvalue
order_date
Date Date
Entered by
clinician
Used to identify date of
prescription
Date medication
was orderedYYYY-MM-
DD
YYYY-MM-DD
MedName Text Text
Prescribed by
Physician
To improve or maintain
the condition of the
patient
Medication
description
associated with
the current
drug_code in the
current record
provider_id Number Auto Number
Automatically
generated by
Access
database
Used to identify each
unique provider within
an organization
Clinic’s internal
provider
identifier. This
field should
accurately match
the current
provider to the
encounters for
which they were
the identified
provider in the
“encounters” file.
provider_name Text Text
20. 20
Entered by IT
administrator
or medical
personnel into
the EHR
Used to identify
provider by name and
credentials i.eMD, PA,
RN etc.
Provider’s name
as you wish for it
to appear in EHR
AgentSubstance Text Text
Entered by
clinician
Used to identify any
allergies to medications
Allergy name
Reaction Text Text
Entered by
clinician
Used to identify the
reaction caused by
allergy
Reaction to
allergic substance
i.e itching
RiskFactors Text Text
Entered by
medical
personnel
Used to identify risk
factors for HIV
Listof
standardized
questions for HIV
Risk Assessment
Result Text Text
Entered by
medical
personnel
Used to identify answer
to risk assessmenti.e
"Yes" or "No"
Yes or No answers
only