1. Presented at: National Society of Genetic Counselors Annual Education Conference, October 21–24, 2015, Pittsburgh, PA
Expanded carrier screening (ECS) is now routinely used in the clinical setting.
As a result, professional societies recently published a joint statement on the
incorporation of expanded carrier screening platforms into clinical practice for
prenatal and preconception patients.1
These guidelines stress the importance of
providing pre- and post-test genetic counseling.
It is important to understand how ECS and genetic counseling impact patients.
A number of studies have been conducted to measure the utility of genetic tests
for patients. For example, in the Impact of Personal Genomics (PGen) Study, a
longitudinal survey was designed to investigate the impact of direct-to-consumer
genetic tests on patients.2
The questions designed for these studies were based on
validated measures of psychological states, health behaviors, and numeracy.
However, no studies to date have specifically assessed patients’ responses to
multiplex genetic tests, such as expanded carrier screening, provided in a clinical
setting and paired with genetic counseling.
We sought to examine patients’ understanding of and engagement with expanded
carrier screening results, evaluate patients’ perceived utility of expanded carrier
screening results, and understand the impact of genetic counseling on patients’
experience with ECS results.
Study Population
Patients enrolled in this study received ECS through our laboratory, typically
for a panel testing over 250 autosomal recessive and X-linked diseases, with
the option to customize. Patients were primarily referred to our laboratory by
reproductive endocrinologists. The majority of patients were contacted as soon as
their results were ready to schedule a telephone genetic counseling appointment.
Some patients were not contacted to schedule genetic counseling due to their
ordering provider’s preference, though this option was still available for an
interested patient. Patients also had the opportunity to opt-out of this service if they
did not wish to speak to a genetic counselor.
Approximately 3 weeks after results were returned, an automated email was sent
to all patients inviting them to participate in this study. Consent was obtained for
all participants. Participants were given an opportunity to enter a raffle where
20 individuals would be randomly chosen to win a $50 gift card. IRB approval
was obtained for this study.
Survey Design
The questions designed for these studies were based on validated measures
of psychological states, health behaviors, and numeracy to enable future
comparison of results. They were designed to align with survey questions asked
in previous research studies with well-developed measures; one such measure
was the “REVEAL Impact of Genetic Testing in Alzheimer’s Disease” measure,
recommended for use in monitoring patients who receive genetic information.3,4
We designed the survey to achieve four specific aims, itemized below. Initial
analysis was conducted to assess differences between carriers and non-carriers,
though future analysis on the full study population will also compare responses
between those who did and did not have genetic counseling through our laboratory.
Aim 1: To assess patients’ understanding of and engagement with ECS
Aim 2: To assess patients’ perceived utility of expanded carrier screening results
Aim 3: To evaluate the impact of genetic counseling on patients’ experiences
with ECS results
Aim 4: To examine the relationships between perceived utility, receipt of genetic
counseling, carrier status, and sociodemographic characteristics
The initial analyses presented here focus on exploring patients’ understanding of
and engagement with their ECS results (Aim 1). Specifically, we looked at the
difference in emotional reaction between carriers and non-carriers.
Data Analysis
Chi-square tests of independence were conducted for all categorical variables
analyzed. Fisher exact tests were used on variables with small cell counts (n5).
Significance thresholds were set at p 0.05.
Study Population and Demographics
A total of 328 participants completed the survey. Most participants identified as
European/Caucasian (n=192), were between the ages of 30-34 years (n=102),
female (n=276), married (n=240), and had no children (n=247).
Carrier Status
136 survey participants self-reported as carriers and 183 self-reported as non-
carriers. This is a carrier rate of 41.4%, which is consistent with the carrier rate
we expect in our patient population. Those who were unsure of their carrier
status (n=9) were excluded from analyses (Table 1).
Genetic Counseling
Out of the total participants, 298 were contacted to schedule a genetic counseling
session at the time of the survey. 271 (84.9%) set up an appointment and received
genetic counseling. Not all referring providers participate in Recombine genetic
counseling services. Examining differences between carriers and non-carriers,
genetic counseling was received by 86.8% (118 out of 136) of carrier patients
and 83.6% (153 out of 183) of non-carrier patients.
Emotional Reactions to Results
Regardless of carrier status, most participants reported never or rarely feeling
negative emotions (sad, surprised, anxious, loss of control, regret, uncertain, worried,
guilty, difficulty making reproductive decisions, and difficulty talking to others)
towards their results. Most reported sometimes or often feeling positive emotions
(relieved, happy, understanding their reproductive choices) regarding their results.
Carriers and non-carriers reported a significant difference between how often they
felt the following emotions in the past two weeks regarding their results: (Table 2).
– Anxious
– Loss of control
– Regret
– Uncertain about what their results mean for their children/family
– Difficulty making decisions for reproductive planning
Carriers and non-carriers did not report a significant difference (p 0.05)
between how often they felt sad, surprised, relieved, happy, and guilty about
possibly passing on disease risk to their children. Carriers and non-carriers also
did not differ significantly (p 0.05) in how often they understood clearly their
decisions for reproductive planning, were worried about children developing
disease, had difficulty talking about their results with others, and if they wanted
to tell others about their results.
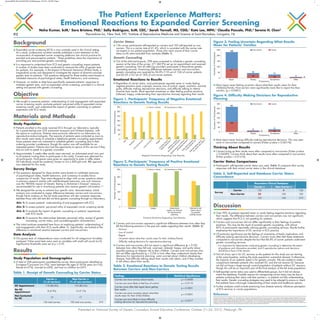
Most report never feeling uncertain about what their results mean for their
child(ren)/family. Non-carriers were significantly more like to report this than
carriers. (p = 0.0001).
Most report never having difficulty making reproductive decisions. This was seen
more in non-carriers compared to carriers (Fisher p-value = 0.04174).
Thinking About Results
Carriers bring up their results more often compared to non-carriers (Fisher p-value
= 0.04589). Carriers think about their results more often compared to non-carriers
(Fisher p-value = 0.01616).
Carrier Status Comparisons
Participants’ self-reported carrier status was used. Table 3 compares their survey
responses with their actual carrier status in the clinical database.
Background
Objective
Materials and Methods
Results
Discussion
Carrier n Non-Carrier n
(% of carriers) (% of non-carriers)
GC Appointment 118 (86.8%) 153 (83.6%)
No GC
8 (5.9%) 13 (7.1%)Appointment
Not Contacted
10 17by GC
136 total carriers 183 total non-carriers 319
Table 1. Receipt of Genetic Counseling by Carrier Status
81
30
19 6
150
15
13
5
0
50
100
150
200
250 Non-Carrier Carrier
NumberofParticipants
Never Rarely Sometimes Often
Frequency
Figure 3. Feeling Uncertain Regarding What Results
Mean for Patients’ Families
Recombine Clinical Database
Carrier n Non-Carrier n
Survey
Carrier 132 4 136
Non-Carrier 23 160 183
155 164 319
Table 3. Self-Reported and Database Carrier Status
Concordance
NumberofParticipants
Non-Carrier Carrier
Never Rarely Sometimes Often
Frequency
109
9 18
161
8
11
3
0
50
100
150
200
250
300
Figure 4. Difficulty Making Decisions for Reproductive
Planning
Feelings Statistical Significance
Carriers are more anxious about results. p = 0.0008
Carriers are more likely to feel loss of control. p = 0.0110
Carriers more often feel regret about getting
their results.
p = 0.0001
Carriers are more uncertain about what their
results mean for their child/children.
p = 0.0001
Carriers are more likely to have difficulty
making decisions for reproductive planning.
p = 0.0417
Table 2. Emotional Reactions to Genetic Testing Results
Between Carriers and Non-Carriers
Surprised
0
50
100
150
200
250
300
350
NumberofParticipants
Sad
Loss
ofcontrol
Anxious/nervous
U
ncertain
about
fam
ily
im
plications
R
egret
W
orried
aboutm
y
children
developing
disease
D
ifficulty
m
aking
reproductive
decisions
D
ifficulty
talking
about
m
y
results
w
ith
others
G
uilty
aboutpassing
on
the
disease
risk
Never or Rarely Sometimes or Often
Negative Emotions Regarding Test Results
Figure 1. Participants’ Frequency of Negative Emotional
Reactions to Genetic Testing Results
0
50
100
150
200
250
Relieved Happy Understood
clearly my choices
for reproductive
planning
Wanted to tell
others about
my genetic
testing results
Positive Emotions Regarding Test Results
NumberofParticipants
Never or Rarely Sometimes or Often
Figure 2. Participants’ Frequency of Positive Emotional
Reactions to Genetic Testing Results
The Patient Experience Matters:
Emotional Reactions to Expanded Carrier Screening
Neha Kumar, ScM,1
Sara Bristow, PhD,1
Sally Rodriguez, ScM, CGC,1
Sarah Yarnall, MS, CGG,1
Kate Lee, MPH,1
Claudia Pascale, PhD,2
Serena H. Chen2
1
Recombine Inc, New York, NY; 2
Institute of Reproductive Medicine and Science at Saint Barnabas, Livingston, NJ92
References
1. Edwards JG, Feldman G, Goldberg J, et al. Expanded Carrier Screening in Reproductive Medicine—Points to Consider: A Joint Statement of the American College of Medical Genetics and
Genomics, American College of Obstetricians and Gynecologists, National Society of Genetic Counselors, Perinatal Qual. Obstet Gynecol. 2015;125(3):653-662. 2. Carere DA, Couper MP,
Crawford SD, et al. Design, methods, and participant characteristics of the Impact of Personal Genomics (PGen) Study, a prospective cohort study of direct-to-consumer personal genomic testing
customers. Genome Med. 2014;6(12):96. 3. Chung WW, Chen CA, Cupples LA, et al. A New Scale Measuring Psychologic Impact of Genetic Susceptibility Testing for Alzheimer Disease.
Alzheimer Dis Assoc Disord. 2009;23:50–56. 4. Carere DA, Couper MP, Crawford SD, et al. Design, methods, and participant characteristics of the Impact of Personal Genomics (PGen) Study,
a prospective cohort study of direct-to-consumer personal genomic testing customers. Genome Med. 2014;6(12):96.
Over 90% of patients reported never or rarely feeling negative emotions regarding
their results. The difference between carriers and non-carriers was not significant,
which suggests that ECS is not upsetting for patients.
Carriers and non-carriers did not differ significantly in their feelings of positive
emotions. This may be the result of post-test genetic counseling, with almost
85% of participants reportedly utilizing genetic counseling services. Results further
emphasize the importance of GC services in ECS practice.
Of particular significance are the feelings of uncertainty of family implications and
difficulty making reproductive decisions. Carriers more often feel these statements
compared to non-carriers despite the fact that 86.8% of carrier patients underwent
genetic counseling services.
– It is important for laboratories conducting genetic counseling to determine the extent
of guidance and information provided, and if reproductive options and decisions
should be a focus of the session.
Not all clinics opt in for GC services so the patients for this study are not starting
at the same baseline, making the study population somewhat skewed. Furthermore,
the majority of our patients opted in for genetic consults. We are unable to make
comparisons between patients who received GC and did not receive GC because
we did not have a large enough control population of patients without GC sessions,
though this will be an important part of the final analysis of the full study population.
Self-reported carrier status was used to differentiate groups, but it did not always
match the database. Possible reasons for misreporting carrier status may be due to
patients confusing their status with their partner’s, or patients not fully understanding
their results. Genetic counseling strategies may need to be adjusted to ensure or check
that patients have a thorough understanding of their results and healthcare options.
Further analyses could include examining how disease severity influences perception
of ECS services in carrier populations.
Kumar NSGC 2015 44x44@196%-PrintReady.qxp 10/13/15 5:42 PM Page 1