1. Evidence Appraisal: Each study was appraised using the following criteria: 1)
human, animal, or cadaveric; 2) prospective or retrospective; and 3) individual
study or systematic review. Based on the availability of the evidence for Aβ, all
types of research were included. The Strength of Reporting Taxonomy (SORT)
was used for classifying the type of evidence.
Data Extraction: The results of Aβ comparisons across time for animal or
human studies were included in the analysis. Results were measured using PET
scan imaging or immunoblotting of cerebral tissue biomarkers.
Summary Measures: Based on the available evidence, changes from baseline
to follow-up for the differences between healthy and injured subjects were
considered. Hedges’ g effect sizes were used for comparing the level of Aβ
deposition in those exposure to TBI compared to non-exposed subjects. For
studies that reported frequency counts of increased Aβ in TBI subjects compared
to healthy subjects, odds ratios were considered.
Critical Appraisal
The Role of Beta-Amyloid Following Traumatic Brain Injury
A Critically Appraised Topic
Powell JR, McKeon PO
Athletic Training Education, Department of Exercise and Sport Sciences, Ithaca College, Ithaca NY
Concussions occur in males and females of all ages and in all sports,
but are most common in contact and collision activities. Data collected
from emergency department visits show a 62% increase (153,375 to
248,418) in nonfatal traumatic brain injuries (TBI) between 2001 and
2009 with as many as 3.8 million reported and unreported sport- and
recreation-related concussions occurring each year in the United
States.1
There is increasing evidence that TBI promotes the accumulation,
misfolding, and aggregation of abnormal proteins associated with
neurodegeneration related to other diseases including Alzheimer’s
disease.2
Beta-amyloid (Aβ) is a partially cleaved protein that is eliminated in a
healthy brain. Accumulation of Aβ forms insoluble plaques which
interrupt neural activity.3 Potentially, this may be a meaningful
biomarker for long-term brain health after TBI.
Background
Search Strategy
Articles were sourced from releveant databases to examine the prospective
link or relationship between TBI and Aβ deposition
• In vivo and cadaveric human studies were included.
• Systematic reviews with meta-analysis of animal studies were included if
the focus of the study centered on linking Aβ to TBI.
• Comparisons of Aβ deposition in TBI to healthy controls were
considered if no neurological comorbidities were present.
• Significant differences were quantified by effect sizes.
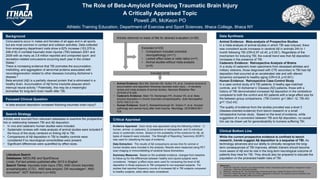
Literature Search
Databases: MEDLINE and SportDiscus
Limits: Full text articles published after 2013 in English
Search Terms: traumatic brain injury (TBI), AND chronic traumatic
encephalopathy (CTE), AND beta amyloid, OR neurodegen*, AND
biomarker*, NOT Alzheimer’s (n=455)
Articles retreived on basis of title for abstract evaluation (n=26)
Excluded (n=23)
• Comparison included comorbid
neuropathology (n=11)
• Lacked effect sizes or odds ratios (n=7)
• Animal studies without meta-analysis
(n=5)
Included (n=3)
While the current prospective evidence is confined to bench
research, trends suggest Aβ deposition is a sequelae of TBI. As
technology advances and our ability to clinically recognize the long-
term consequences of TBI improves, athletic trainers should become
more aware of Aβ and its role in the long-term neurological outcome of
patients they treat for TBI. They should also be prepared to educate the
population on the protracted health risks of TBI.
Clinical Bottom Line
• Animal Evidence: Bird SM, Sohrabi HR, Sutton TA, et al. Cerebral amyloid-β
accumulation and deposition following traumatic brain injury – A narrative
review and meta-analysis of animal studies. Neurosci Biobehav Rev.
2016;64:215-228.
• Cadeveric Evidence: Stein TD, Montenigro PH, Alvarez VE, et al. Beta-
amyloid deposition in chronic traumatic encephalopathy. Acta Neuropathol
2015;130(1):21-34.
• Human Evidence: Scott G, Ramlackhansingh AF, Edison P, et al. Amyloid
pathology and axonal injury after brain trauma. Neurology. 2016;86(9):821-
828.
References:
1. Broglio SP, Cantu RC, Gioia GA, et al. National Athletic Trainers’ Association position statement: management of sport
concussion. J Athl Train. 2014;49(2):245-265.
2. McKee AC, Daneshvar DH. The neuropathology of traumatic brain injury. Handb Clin Neurol. 2015;127:45-66.
3. Irvine GB, El-Agnaf OM, Shankar GM, et al. Protein Aggregation in the Brain: The molecular basis for Alzheimer’s and
Parkinson’s diseases. Mol Med. 2008;14(7-8):451-464.
Animal Evidence: Meta-analysis of Prospective Studies
In a meta-analysis of animal studies in which TBI was induced, there
was consistent acute increases in cerebral Aβ in animals 24h to 1
month following TBI (OR=2.97 ±0.40, p 0.001). Regardless of the
mechanism for inducing TBI, the overall trend was that Aβ deposition
increases in the presence of TBI.
Cadaveric Evidence: Retrospective Analysis of Brains
In a study of cadaveric brain specimens from deceased athletes and
military veterans, those diagnosed with CTE secondary to TBI had Aβ
deposition that occurred at an accelerated rate and with altered
dynamics compared to healthy aging (OR=3.8, p<0.001).
Human Evidence: Retrospective Case-Control Study
In a case control study of 9 TBI patients, 9 heathy age-matched
controls, and 10 Alzheimer’s’ Disease (AD) patients, those with a
history of TBI demonstrated increased Aβ deposition in the cerebellum
compared to both the control and AD patients with a large effect size for
the between-group comparisons. (TBI-Control: g=1.96±1.12, TBI-AD:
g=7.12±2.43).
The quality of evidence from the studies provided was a level 3
(disease-oriented evidence) from bench research or a small
retrospective human study. Based on the level of evidence, while
suggestive of a connection between TBI and Aβ deposition, no causal
link can be drawn yet for generalizability to humans suffering TBI.
Data Synthesis
Is beta-amyloid deposition increased following traumatic brain injury?
Focused Clinical Question