1. Validation of ASHA FACS–Functional Assessment of
Communication Skills for Alzheimer Disease Population
Isabel Albuquerque M. de Carvalho, PhD* and Letı´cia Lessa Mansur, PhDw
Abstract: This study was aimed to validate the American
Speech-Language-Hearing Association Functional Assessment
of Communication Skills (ASHA FACS) for a Brazilian
population. The scale was translated and adapted into
Portuguese. Thirty-two patients with mild Alzheimer disease
(AD), 25 patients with moderate AD, and 51 elderly without
dementia were examined with Mini Mental State Examination,
Geriatric Depression Scale, and Alzheimer Disease Assessment
Scale-cognitive subscale (ADAS-cog). The ASHA FACS was
answered by their relative/caregiver. The scale’s internal
consistency, its inter-examiner and intra-examiner’s reproduci-
bility, and scale’s criterion validity were researched by correla-
tion with ADAS-cog. The sensitivity and specificity were also
researched. Statistical analyses indicated that the ASHA FACS
has excellent internal consistency (Cronbach a = 0.955), test-
retest reliability (interclass correlation coefficient = 0.995;
P<0.001), and inter-examiners (interclass correlation coeffi-
cient = 0.998; P<0.001). It showed excellent criterion validity
when correlated with ADAS-cog. The ASHA FACS scale
showed good sensitivity (75.0%) and specificity (82.4%) values
once it is an ecologic and broad evaluation. The ASHA FACS
Portuguese version is a valid and reliable instrument to verify
communication alterations in AD patients and fills an important
gap of efficiency indicators for speech language therapy in our
country.
Key Words: communication, functionality, language, Alzheimer
disease, functional assessment
(Alzheimer Dis Assoc Disord 2008;22:375–381)
Functional communication is the ability to receive or
convey a message and also to communicate effectively
and independently in a natural environment regardless of
the mode of communication.1
This definition embraces an integrated concept of
communication rather than isolated processes. It em-
braces any verbal or nonverbal communication modality
and considers efficiency and independence as essential to
an appropriate response to everyday demands.2
One of the most important complaints of caregivers
and relatives of patients with Alzheimer disease (AD) is
the difficulty maintaining efficient and independent
communication, which leads to relationship problems
with family and others.
AD is a highly prevalent type of dementia.3
Its
diagnosis may be performed through clinical and
laboratorial evaluation and imaging tests. A functional
evaluation may be component of a clinical evaluation as it
estimates one’s ability to perform daily living activities; in
other words, the deficit caused by the disease and an
assessment of the negative impact on functional abilities
in an ecologic situation.4
Communication may be impaired from the first
stage of the disease.5–9
Consequently, speech and
language evaluation should assess the ability to commu-
nicate in different situations, independently of speech,
language, or cognitive impairment. This assessment
should consider environmental modifications, use of
hearing aids, time needed to communicate and behaviors
that may interfere with communicative ability in an
ecologic situation.
Such assessment may be better understood con-
sidering the International Classification of Functioning,
Disability, and Health (WHO-ICF),10
which considers
‘‘body’’ as functions of body systems or body structures,
and ‘‘activity and participation’’ as a complete range of
domains denoting aspects of functioning from both an
individual and societal perspective. This is information on
diagnosis plus functioning that provide a broader and
more meaningful picture of the health of people and
populations, which can then be used for decision-making
purposes.
The ICF defines ‘‘activity’’ as the execution of a task
or action by an individual and ‘‘participation’’ as the
involvement in a life situation. The contextual factors
represent the complete background of individual’s life
and living, which may have an impact on the individual
with a healthy condition.11
On the basis of this model, functionality focuses on
components of body structure/function; activity/partici-
pation, and environmental/personal factors used in a
positive way. Most functional communication tasks areCopyright r 2008 by Lippincott Williams & Wilkins
Received for publication November 27, 2007; accepted July 12, 2008.
From the *Old Age Research Group (PROTER) and CEREDIC,
School of Medicine; and wDepartment of Physiotherapy, Speech
Therapy and Occupational Therapy, University of Sa˜ o Paulo,
Sa˜ o Paulo, Brazil.
Grant support by CAPES (Coordenac¸a˜ o de Aperfeic¸oamento de Pessoal
de Nı´vel Superior).
Reprints: Isabel Albuquerque M. de Carvalho, PhD, Al. Santos 455 cj.
1611, 01419-000 Sa˜ o Paulo, SP, Brazil (e-mail: belcarvalho@
terra.com.br).
ORIGINAL ARTICLE
Alzheimer Dis Assoc Disord Volume 22, Number 4, October–December 2008 375
2. classified as activity/participation and have a direct
relation to social inclusion and quality of life.
Functional activity assessment scales center on
quantifying and qualifying the deficiency caused by the
disease in the view of functionality. They also facilitate
therapeutic planning and familial/caregiver orientation.
From a research perspective, functional evaluation
provides information on efficacy and effectiveness of
therapeutic treatments. From an economic point of view,
functional evaluation may determine specific treatment
based on its cost/benefit.12
The American Speech-Language-Hearing Associa-
tion Functional Assessment of Communication Skills for
Adults (ASHA FACS) augments traditional assessment
of speech, language, and cognitive deficits, with informa-
tion on deficit effects on the daily cognitive-communica-
tive context. It can be used to determine weather the
subject is able to carry on a conversation, communicate
basic needs, and conduct daily planning. In other words,
it evaluates how communication impairment affects an
individual’s ability to perform basic everyday commu-
nication functions.13
The scale was first developed and validated in the
United States for adults with aphasia after left hemi-
sphere stroke and adults with traumatic brain injury. To
extend the use of the ASHA FACS to additional
populations, Paul et al13
conducted a validation study
of the ASHA FACS for multicultural population, adult
population with communication disorders stemming from
right hemisphere stroke, dementia, and dysarthria, and a
field test for international use. Their results suggested that
the ASHA FACS is a valid instrument to assess
functional communication ability for demented patients
with AD and related dementias.
Functional analyses of communication in healthy
elderly and those with AD may suggest that important
communication impairment throughout the disease wor-
sens patient’s independence and autonomy, in addition to
compromising their quality of life.14
There is no such assessment instrument in Brazil.
The ASHA FACS would be of great value to assess
patients with dementia.
The goal of this study is to validate the Brazilian
version of communication independence of the ASHA
FACS for clinical use with Alzheimer patients.
METHODS
A total of 108 subjects, 51 cognitively intact elderly
individuals, 32 patients with mild AD, and 25 patients
with moderate AD participated in the study. The AD
group (ADG) consisted of individuals who met the
criteria for probable AD according to National Institute
of Neurological and Communicative Diseases and
Stroke/Alzheimer’s Disease and Related Disorders Asso-
ciation,15
and they were all in anticholinesterasic treat-
ment for at least 3 months.
Control group (CG) was composed of elderly with
no dementia and ADG was composed of all patients with
AD (both mild and moderate patients). Although the best
way to classify dementia in its severity level is through the
Clinical Dementia Rating, we decided to follow Paul
et al’s13
study that had used the Mini Mental State
Examination (MMSE) for that purpose. We used the
Brazilian classification of MMSE according to level of
education16
for that matter.
Both groups (CG and ADG) had individuals older
than 65 years of age, with no history of drug or alcohol
abuse, no depression symptoms, or noncontrolled depres-
sion (Geriatric Depression Scale, GDS10),17
and no
other neurologic disease associated with AD. In addition
to these exclusion criteria, normal elderly with MMSE16
scores less than 18 for illiteracy were excluded from the
study, 21 for subjects with 1 to 3 years of formal
education and 24 for individuals with 4 or more years of
formal education. Patients with AD and MMSE less than
11 were also excluded. All subjects were free of severe and
uncorrected visual or auditory deficits that could interfere
with test performance.
Patients with AD were selected among Old Age
Research Group (PROTER) Psychiatric Institute, Neuro-
linguistic Investigation Laboratory (Laborato´rio de In-
vestigac¸a˜o em Neurolingu¨ı´stica) and Cognitive Disorders
Reference Center (CEREDIC), Hospital das Clı´nicas,
School of Medicine, University of Sa˜ o Paulo. Elderly with
no dementia were selected among the community of Sa˜ o
Paulo and Poc¸os de Caldas and among caregivers of
patients from PROTER and CEREDIC who did not
participate in this study.
The ASHA FACS is a functional scale that assesses
a complex communication situation in an ecologic
environment. It consists of a communicative indepen-
dence score and qualitative dimensions of communication
scores. The 7-point Scale of Communication Indepen-
dence measures functional communication performance
along a continuum of independence, in terms of levels
of assistance and/or prompting needed to communicate.
The 5-point Scale of Qualitative Dimensions of Commu-
nication measures a range of response dimensions
(ie, adequacy, appropriateness, promptness, and commu-
nication sharing). In this study, we addressed the
communication independence scale.
The ASHA FACS communication independence
scale is composed of 43 items divided into 4 domains:
Social Communication (21 items); Communication of
Basic Needs (7 items); Reading, Writing, and Number
Concepts (10 items); and Daily Planning (5 items). Within
each domain, functional behaviors that are to be observed
and rated are specified (Appendix). The 7-point scale
score assess communication performance in an indepen-
dence continuum in terms of prompting and/or assis-
tance. The definition of scores are: 7 means that the
subject is totally able to perform the communication
behavior with no assistance; 6 means that the subject
performs the communication behavior rarely needing
assistance; 5 means that the subject needs assistance
occasionally; 4 means that the assistance is often; 3 means
that to have a good communication performance the
de Carvalho and Mansur Alzheimer Dis Assoc Disord Volume 22, Number 4, October–December 2008
376 r 2008 Lippincott Williams Wilkins
3. subject will need assistance very frequently; 2 means that
the assistance has to be maximal; and 1 means that even
with maximal assistance, the individual is not able to
perform the communication behavior. There is also an N
rating that means the behavior cannot be observed nor is
information available from other sources.
After a written authorization from ASHA to
validate the ASHA FACS for a Brazilian population, a
translation into Portuguese was done following a
thorough procedure.18
Initially, the original instrument
was translated into Portuguese by 2 speech language
pathologists and 1 independent translator. These 3
translations were then compared resulting in the initial
version of the scale in Portuguese. Subsequently, back
translation into English was performed by 2 translators to
identify possible inconsistencies and discrepancies in the
English to Portuguese translation. Minor differences were
identified and discussed by a small committee of judges.
A final consensual Portuguese version of the ASHA
FACS was produced and used in the present study.
The initial part of the ASHA FACS scale is
composed of a questionnaire focusing on age, schooling,
present and previous occupational activity, living situa-
tion (alone, with family, or institution), information
about laterality, other language spoken, previous reading
and writing ability, and use of glasses or hearing aids.
Only after this first interview and considering inclusion
and exclusion criteria, the subjects were included in the
study.
Data were collected through the following protocol:
MMSE—Brazilian version,15,19,20
GDS,17
Alzheimer Dis-
ease Assessment Scale-cognitive subscale (ADAS-cog)—
Brazilian version,21,22
and ASHA FACS.2
All subjects
from both CG and ADG answered MMSE, GDS, and
ADAS-cog, whereas the family or caregiver answered the
ASHA FACS about the subject tested.
The protocol application took approximately 1
hour, being 45 minutes with the subject and 15 to 20
minutes with family or caregiver, being administered by
the first author of this study and another speech language
pathologist previously trained to administer this func-
tional scale, in a quiet environment. To have data scored
by 2 different examiners for the interrater reliability
analysis, all testing were taped on a digital recorder
(Panasonic RR-US360) and send to the other speech
pathologist to score the test from the original and
complete testing. For the intrarater reliability, it was
used as the first data collection, described above as ‘‘first
interview’’ and the second data (or interview) was taken
within 2 weeks of difference from the first one.
It is very important to highlight that all the family
members who answered the ASHA FACS were the
patient’s main caregiver. There were no professional
caregivers; they were all very close to the patient. To
maintain the pattern, we also selected only close relatives
to answer the ASHA FACS for the CG.
Field testing of the ASHA FACS was conducted
to assess internal consistency; interrater and intrarater
reliability, validity, instrument sensitivity and specificity.
First, internal consistency analysis of the ASHA FACS
and of each domain was carried out. The number
of individuals assessed in each domain varied once
Cronbach a coefficient was calculated, which was done
only for the subjects (control or AD) who had answered
the domains and the total scale completely. In this
respect, 75 individuals answered the total scale score, 96
for Social Communication, 108 for Communication of
Basic Needs, 108 individuals for Reading, Writing, and
Numbers Concepts, and 92 people for Daily Planning.
Statistical Analysis
The following tests were used in the statistical
analyses: 1. Kruskal-Wallis (with Dunn posttest;
P0.05) to analyze sex, age, education, MMSE, and
GDS, comparing CG with mild and moderate ADG. 2.
ASHA FACS internal consistency was calculated using
the Cronbach a coefficient. 3. To analyze interrate and
intrarate reliability, 1-way interclass correlation coeffi-
cient23
was used to follow the international studies
performed with ASHA FACS. 4. To analyze predictive
value (sensitivity and specificity), an ROC (receiver
operating characteristic) curve analysis was done. 5.
Spearman correlation was used for correlation analyses
among ASHA FACS domains and ADAS-cog. 6.
Descriptive analyses (means and standard deviation) of
sociodemographic variables and of the descriptive data
were carried out.
Ethics
This study was approved by the Ethics in Research
Committee of the Hospital Das Clı´nicas Da Faculdade
De Medicina Da Universidade De Sa˜ o Paulo and all
participants signed the informed consent forms.
RESULTS
Sociodemographic characterization showed equiva-
lence for education for all groups, mean years of
education was 5.31 ( ± 5.07) for the CG; 6.84 ( ± 4.91)
for mild ADG; and 4.76 ( ± 3.49) for moderate ADG,
P = 0.116. There was a significant difference of age
(P0.001) between CG 74.08 ( ± 7.21) and ADG but
not between mild 77.75 ( ± 5.48) and moderate ADG
79.44 ( ± 5.94), even though all were above 74 years old.
In sex analysis, there were more female subjects in the
control and moderate ADG, whereas the mild ADG was
very homogeneous for sex with a slight advantage for
male subjects.
The MMSE mean score showed a significant
difference among 3 groups as expected to differentiate
nondemented individuals from mild and moderate AD
patients. There was no significant difference among the
3 groups for GDS, also as expected.
Family/caregiver answered the ASHA FACS scale
about the subject tested. Most of them in both the groups
were daughters followed by wives. More than 80%
respondents were female. Graphics 1 and 2 characterize
their relationship to the subject.
Alzheimer Dis Assoc Disord Volume 22, Number 4, October–December 2008 Validation of ASHA FACS
r 2008 Lippincott Williams Wilkins 377
4. Table 1 presents the Cronbach a coefficient for
ASHA FACS internal consistency, considering all
tested individuals. a scores above 0.70 represent the
scale’s high internal consistency. Results showed high
internal consistency for the scale’s total score and for all 4
domains, even for Communication of Basic Needs that
had a = 0.744. In an item-by-item analysis, item number
15, ‘‘understand tone of voice’’ from the Social Commu-
nication domain, had the lowest internal consistency
value. Calculating a’s coefficient without this item, the
result was 0.957 and had no effect on scale’s internal
consistency. For this reason, the authors did not remove
the item.
To analyze the inter-examiner and intra-examiner
reliability both, mild and moderate ADG were considered
as 1 group (ADG). Table 2 presents these analyses of each
ASHA FACS domains and total score. The results
suggest high test-retest and inter-examiner values for all
domains and for the scale total score.
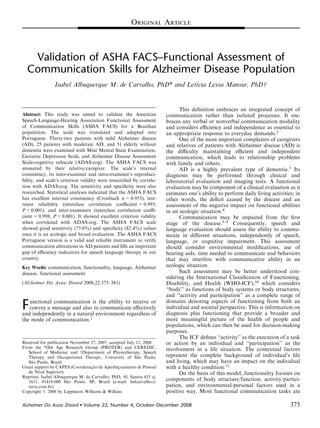
Table 3 shows the significant correlation between
ASHA FACS scale and ADAS-cog test used as a gold
standard for validation process. Graphics 3 and 4
illustrate that the lower the ADAS-cog score (showing
cognitively preserved performance), the higher the ASHA
FACS score.
The ROC curve analysis was used to verify ASHA
FACS sensitivity and specificity. They were calculated
for each sample value, and the value that maximized
sensitivity and specificity simultaneously was selected.
The closer to the upper left corner the curve is, and
the closer to 1.0 the area on the curve is, the better
the accuracy measurement in discriminating subjects,
based on the gold standard method. The ROC
curve results for mild ADG only showed an area on the
curve of 0.851 (95% confidence interval, 0.770-0.932;
P0.001); sensitivity of 75.0% and specificity of
82.2% with 79.5% of accuracy. Positive predictive
value was 72.7% and negative predictive value
was 84.0%. The suggested ASHA FACS cut-off was
5.98 to be indicative of AD. Graphic 5 illustrate these
results.
DISCUSSION
This study was mainly motivated by the lack of
efficacy indicators for speech language interventions in
clinical practice and scientific research. From this point of
view, there is a great need for an instrument, in Brazilian
Portuguese, with characteristics to assess communication
in patients with dementia for both diagnosis and follow-
up purposes.
The ASHA FACS is a simple, quick, and low-cost
assessment that provides information about the patient’s
cognitive-communicative behavior in their environment.
11,90%
7,14%
35,71%9,52%
23,81%
2,38%
4,76% 4,76%
wife
husband
daughter
son
Grandaughter
Grandson
companion
sister
GRAPHIC 1. ASHA FACS respondent’s characterization—
Control group. ASHA FACS indicates American Speech-
Language-Hearing Association Functional Assessment of
Communication Skills
18,87%
5,66%
49,06%
7,55%
3,77%
1,89%
7,55%
1,89%
1,89%
1,89%
wife
husband
daughter
son
grandaughter
grandson
Daughter in law
nephew
friend
ex-wife
GRAPHIC 2. ASHA FACS respondent’s characterization—AD
group. AD indicates Alzheimer disease; ASHA FACS, American
Speech-Language-Hearing Association Functional Assessment
of Communication Skills.
TABLE 1. ASHA FACS Internal Consistency Analysis
Total Score and Domains No. Items Cronbach a
ASHA FACS—Total (n = 75) 43 0.955
Social Communication (n = 96) 21 0.887
Basic Needs (n = 108) 7 0.744
Reading, Writing, Number
Concepts (n = 98)
10 0.923
Daily Planning (n = 92) 5 0.814
ASHA FACS indicates American Speech-Language-Hearing Association
Functional Assessment of Communication Skills; n, number of individuals.
TABLE 2. ASHA FACS Intrarate and Interrate Reliability
Total Score
(n = 28)
CG
(n = 12)
ADG
(n = 16)
ASHA FACS
Domains Intra Inter Intra Inter Intra Inter
Social
Communication
0.968* 0.981* 0.952* 0.756* 0.936* 0.972*
Basic Needs 0.967* 0.995* 0.886* 0.996* 0.966* 0.993*
Reading, Writing,
and Number
Concepts
0.993* 0.992* 0.914* 0.920* 0.989* 0.986*
Daily Planning 0.995* 0.999* 0.993* 0.992* 0.971* 0.993*
ASHA FACS
Total score
0.995* 0.998* 0.974* 0.972* 0.988* 0.996*
*P0.001.
ADG indicates Alzheimer disease group; ASHA FACS, American Speech-
Language-Hearing Association Functional Assessment of Communication Skills;
CG, control group; n, number of individuals.
de Carvalho and Mansur Alzheimer Dis Assoc Disord Volume 22, Number 4, October–December 2008
378 r 2008 Lippincott Williams Wilkins
5. A functional assessment of communication was chosen
because of the understanding that the loss of indepen-
dence caused by the lack of ability to care for oneself;
control one’s body and mind and act on the environment
may be one of the most primary human fear. The
difficulty in communicating is understood as a worsening
in loss of functionality, which leads to a rise in
dependence.
Throughout the course of dementia, an important
loss caused by cognitive decline may compromise
functionality. During the process of AD, there is a
decline of memory, attention, and language, which
impacts negatively on the communication ability6,24
and
may cause disengagement of interpersonal relationships,
worsening cognitive decline, increased caregiver stress,
and a worsening of patient and family/caregiver’s quality
of life.
In this study, there was homogeneity of sample for
education, sex, laterality (with almost 100% for right-
handed individuals), use of glasses or auricular prosthesis,
state of living (most individuals living with their families
in both groups), and no depression symptoms. The age
variable had statistical significant difference between the
groups, ADG having an average of 4 years older than the
CG, although both groups had an age average higher
than 74 years. Higher age mean for AD patients
corroborates literature data, that says prevalence of AD
gets higher as age increases.25
No stress level test was
applied to this population, although it could be a good
measure for next studies.
We were careful to do the golden standard test
(ADAS-cog) in all subjects, independently of their score
on the ASHA FACS scale. Unfortunately, it was not
possible to do the assessment protocol in a blinded
situation because the first author selected and assessed all
individuals. To minimize the bias, the professional
responsible for the ASHA FACS reassessment to inter-
rater reliability analyses had no previous knowledge of
the subject’s diagnosis.
The ADAS-cog was used as a gold standard test
because of its nature of a nonecologic test of the cognitive
functions, which has been translated, adapted, and
validated for a Brazilian population and mainly because
there is no other functional evaluation properly validated
in Brazil that could be used as a gold standard for the
ASHA FACS. The results presented here showed that
the ASHA FACS score have significant correlation to
ADAS-cog for both demented and normal elderly.
The nature of ADAS-cog and ASHA FACS
assessment is different. The first is a cognitive test to
TABLE 3. Correlation Between ASHA FACS Versus ADAS-cog
Social
Communication Basic Needs
Reading, Writing, and
Number Concepts Daily Planning
Overall ASHA
FACS Score
ADAS-cog (n = 57)
Control r = À 0.53 r = À 0.30 r = À 0.54 r = À 0.55 r = À 0.63
P0.0001 P = 0.034 P0.0001 P0.0001 P0.0001
AD r = À 0.52 r = À 0.51 r = À 0.71 r = À 0.56 r = À 0.69
P0.0001 P0.0001 P0.0001 P0.0001 P0.0001
Bold values have statistical significance.
ADAS-cog indicates Alzheimer’s Disease Assessment Scale-cognitive subscale; ASHA FACS, American Speech-Language-Hearing Association Functional Assessment
of Communication Skills; CG, control group; n, number of individuals.
0 10 20 30 40
4.5
5.0
5.5
6.0
6.5
7.0
EscoreTotaldaAsha-facs
Escore da ADAS-cog
r = -.63; p0.001
GRAPHIC 3. Correlation ADAS-cog versus ASHA FACS—
Control group. ADAS-cog indicates Alzheimer Disease Assess-
ment Scale-cognitive subscale; ASHA FACS, American
Speech-Language-Hearing Association Functional Assessment
of Communication Skills.
10 20 30 40 50 60
2.0
2.5
3.0
3.5
4.0
4.5
5.0
5.5
6.0
6.5
7.0
EscoreTotaldaAsha-facs
Escore da ADAS-cog
r = -.69; p0.001
GRAPHIC 4. Correlation ADAS-cog versus ASHA FACS—AD
group. ADAS-cog indicates Alzheimer Disease Assessment
Scale-cognitive subscale; ASHA FACS, American Speech-
Language-Hearing Association Functional Assessment of
Communication Skills.
Alzheimer Dis Assoc Disord Volume 22, Number 4, October–December 2008 Validation of ASHA FACS
r 2008 Lippincott Williams Wilkins 379
6. evaluate AD’s process and the latter is an ecologic
assessment that highlights the communicative behavior
associated with cognitive function. Therefore, it seems
very appropriate to use ADAS-cog for the validation
process as the 2 instruments assess distinct sides of the
same issue. The scale of functional communication skills
may add important ecologic information to the ADAS-
cog and other tests on AD patient cognitive and
functional evaluation.
The results show that the functional communication
skills may be understood in its cognitive correspondence
and that communicative ability patterns may be used as
indicative of cognitive decline. The translated and
adapted scale’s internal consistency findings for our
population are consistent with the internal consistency
findings of the studies performed with the original scale in
United States and other English-speaking countries.2,13
We considered even for the interrate reliability value for
Social Communication domain for the CG, which is 0.756
but had statistical significance. That may be explained
once Social Communication is a broad domain and
answers depends much of the person and environment
that we are exposed to have a good performance, being so
the answers may vary a little.
The sensitivity and specificity analyses indicate that
ASHA FACS is good to differentiate healthy subjects
from those with AD process (75%), and specific to
identify individuals with AD (82.4%). The sensitivity and
specificity values are considered satisfactory as the
functional scale assesses complex communicative function
in a broad manner. The area above the ROC curve also
indicated good accuracy in discriminating subjects.
Finally, the statistical analysis with mild AD only,
suggests a cut-off score of 5.98 to detect AD.
In conclusion, the ASHA FACS showed great
interrate and intrarate reproducibility, a high correlation
to the gold standard test, and good sensitivity and
specificity. These data suggest that ASHA FACS is a
valid and reliable scale for a population with AD, and
may supplement the lack of efficacy indicators for clinical
and scientific speech language intervention in our
environment.
APPENDIX
ASHA-FACS
Domains
Social
Communication
Communication
of Basic Needs
Reading, Writing,
and Number
Concepts
Daily
Planning
Behavior
Refer to familiar
people by name
Recognize
familiar voices/
faces
Understand
simple signs
Know what
time it is
Express
agreement/
disagreement
Make likes/
dislikes known
Use common
reference
material
Dial phone
numbers
Explain how to
do something
Express feelings Follow written
directions
Keep
scheduled
appoint-
ments
Request
information
Request helps Understand basic
print material
Use
calendar
Exchange
information on
the phone
Respond in an
emergency
Write/type own
name
Follow a
map
Answer yes/no
questions
Fill out forms
Follow simple
verbal
directions
Write massages
Understand non
literal meaning
Comprehend
numbers
Understand
intent
Make basic
money
transactions
Understand
conversation in
a noisy
situation
Understand
simple units of
measurement
Understand TV/
radio
Participate in
conversation
Recognize/correct
own
communication
error
REFERENCES
1. American Speech-Language-Hearing Association (ASHA). Advisory
Report, Functional Communication Measures Project. Rockville,
MD: ASHA; 1990.
2. Fratalli C, Thompson C, Holland A, et al. Functional Assessment of
Communication Skills for Adults (ASHA FACS). Rockville, MD:
American Speech-Language-Hearing Association; 1995.
3. Morris JC. Differential diagnosis of Alzheimer’s disease. Clin
Geriatr Med. 1994;10:257–276.
ROC curve
1 - Specificity
1,00,75,50,250,00
Sensibility
1,00
,75
,50
,25
0,00
Area=0.851; CI95%=(0.770; 0.932); p0.001
Sensitivity=75.0%
Specificity=82.4%
GRAPHIC 5. ROC curve analysis for ASHA FACS total score.
ASHA FACS indicates American Speech-Language-Hearing
Association Functional Assessment of Communication Skills;
ROC, receiver operating characteristics.
de Carvalho and Mansur Alzheimer Dis Assoc Disord Volume 22, Number 4, October–December 2008
380 r 2008 Lippincott Williams Wilkins
7. 4. McCue M, Pramuka M. Functional assessment. In: Goldstein G,
Beers S, eds. Rehabilitation. New York: Plenum Press; 1998.
5. Heller RB, Dobbs AR, Rule BG. Communicative function in patients
with questionable Alzheimer’s disease. Psychol Aging. 1992;7:395–400.
6. Ripich D. Functional communication with AD patients: a caregiver
training program. Alzheimer Dis Assoc Disord. 1994;8:95–109.
7. Bayles K. Effects of working memory deficits on the communicative
functioning of Alzheimer’s dementia patients. J Commun Disord.
2003;36:209–219.
8. Forbes-McKay KE, Venneri A. Detecting subtle spontaneous
language decline in early Alzheimer’s disease with a picture
description task. Neurol Sci. 2005;26:243–254.
9. Mansur LL, Carthery MT, Caramelli P, et al. Linguagem e cognic¸a˜ o
na doenc¸a de Alzheimer (Language and cognition in Alzheimer’s
disease). Psicologia. 2005;18:300–307.
10. WHO. International Classification of Functioning, Disability and
Health (ICF). Geneva: WHO; 2001. Available at: http://www.who.int/
classifications/icf/en/.
11. Buchalla CM. A Classificac¸a˜ o Internacional de Funcionalidade,
Incapacidade e Sau´ de (International Classification of Functionality,
Incapacity and Health). Acta Fisia´trica. 2003;10:29–31.
12. Fratalli C. Functional assessment. In: Lubisnky R, Fratalli C, eds.
Professional Issues in Speech-language Pathology and Audiology. 2nd
ed. San Diego: Singular Publisher Group; 2000.
13. Paul D, Fratalli C, Holland A, et al. Functional Assessment of
Communication Skills for Adults–Addendum. Rockville, MD:
American Speech-Language Hearing Association; 2004.
14. Carvalho IA. Comunicac¸a˜ o funcional em idosos sadios e com
doenc¸a de Alzheimer. Exame de qualificac¸a˜ o. Programa de
Po´ s-graduac¸a˜ o em Fisiopatologia Experimental da Faculdade de
Medicina da Universidade de Sa˜ o Paulo. (Functional Communica-
tion in healthy elderly and Alzheimer’s disease patients. Graduation
Exam. Graduation Program in Experimental Phisiopathology,
School of Medicine, University of Sao Paulo); 2005.
15. McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of
Alzheimer’s disease: report of the NINCDS-ADRDA work group
under the auspice of department of health and human services task
force on Alzheimer’s disease. Neurology. 1984;34:939–944.
16. Brucki SM, Nitrini R, Caramelli P, et al. Sugesto˜ es para o uso do
Miniexame do Estado Mental no Brasil. Arq Neuropsiq. 2003;61(3B):
777–781.
17. Yesavage JA, Brink TL, Rose TL, et al. Development and
validation of a geriatric depression screening scale: a preliminary
report. J Psychiatr Res. 1983;17:37–49.
18. Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of
health-related quality of life measures: literature review and
proposed guidelines. J Clin Epidemiol. 1993;46:1417–1432.
19. Folstein MF, Folstein SE, McHugh PR. ‘‘Mini-Mental State’’.
A practical method for grading the cognitive state of patients for the
clinician. J Psychiatr Res. 1975;12:189–198.
20. Bertolucci PH, Brucki SM, Campacci SR, et al. O Miniexame do
Estado Mental em uma populac¸a˜ o geral: impacto da escolaridade
(The Mini Mental State Examination in general population: formal
education impact). Arq Neuropsiq. 1994;52:1–7.
21. Rosen WG, Mohs RC, Davis KL. A new rating scale for
Alzheimer’s disease. Am J Psychiatry. 1984;141:1356–1364.
22. Schultz RR, Siviero MO, Bertolucci PHF. The cognitive subscale of
‘‘Alzheimer’s Disease Assessment Scale’’ in a Brazilian sample. Braz
J Med Biol Res. 2001;34:1295–1302.
23. Schick P. Assessing reproducibility for internal data in health-
related quality of life questionnaires: which coefficient should be
used? Qual Life Res. 2004;13:571–586.
24. Venneri A, Forbes-McKay KE, Shanks MF. Impoverishment of
spontaneous language and the prediction of Alzheimer’s disease.
Brain. 2005;128(Pt4):E27.
25. Lopes MA, Bottino CM. Prevaleˆ ncia de demeˆ ncia em diversas
regio˜ es do mundo-Ana´ lises de estudos epidemiolo´ gicos de 1994 a
2000. Arq Neuropsiquiatr. 2002;60:61–69.
Alzheimer Dis Assoc Disord Volume 22, Number 4, October–December 2008 Validation of ASHA FACS
r 2008 Lippincott Williams Wilkins 381