1. #
Gender
Extra-axial Space Parenchyma (Grey Matter)
Tracts (White
Matter)
OtherAge at
Scan
1
F • 4mm deep chronic subdural
collection over left cerebral
convexity; no mass effect
- - -
1 m
2
F
- - - -
1 m
3
F
• Bilateral subdural fluid
collections with mild mass
effect on the right side - -
• Machrocephalic
5 m • Mild ventriculomegaly
4
M
• Mild prominence of anterior
subarachnoid space - -
• Dilated right
lateral
semicircular canal
& vestibule
5 m
5
M
-
• Tissue loss in left temporal lobe
• Mild thinning of
the corpus
callosum
-• Multifocal lesion of susceptibility
consistent with chronic blood
products
6 m
6
M • Prominent extra-axial spaces
bilaterally in frontal and
temporal regions
• Mild parenchymal volume loss • Thinning of the
corpus
callosum
-• Right cerebellar hemisphere hypo-
density (possible old hemorrhage)6 m
7
M
• Extra-axial space anteriorly
• 4 mm signal abnormality at the
level of the base of the right
hypothalamus with 3rd
ventricle
- • Brachycephalic
11 m
QUANTIFICATION OF PROLONGED SEDATION IN INFANTS AND
CORRELATION TO BRAIN MRI FINDINGS
METHODS
We compared patients with healthy controls at two ages: <6 months (N=4
patients and 3 controls) and 6-12 months (N=3 patients and 3 control) as per
IRB approval at Boston Children’s Hospital. We quantified the amounts of
drugs used for prolonged sedation management that included muscle relaxants
(cisatracurium, rocuronium), opioids (fentanyl, morphine, methadone), and
benzodiazepines (midazolam, lorazepam). We analyzed: (1) average daily
doses during sedation and weaning per group (mg/kg/day ± SD); (2) individual
total treatment doses per patient (mg/kg/day); and (3) individual daily doses
over time (mg/kg) only for morphine and midazolam. The number of anesthesia
events and individual neuroradiology reports were also presented. Pearson’s
correlation coefficient was used to measure the linear relations between
different variables analyzed.
SUMMARY AND CONCLUSIONS
v Patients with gastro-intestinal and cardiac diseases undergo very
long periods of sedation.
v Of all the drugs used, morphine and midazolam were used the
most frequently and were administered at the highest doses.
v Prolonged sedation with morphine and midazolam is strongly
associated with increased incidence of neuroradiological
abnormalities in infants younger than 12 months of age. Days of
sedation and the number of anesthesia events do not appear to be
associated with the number of neuroradiology abnormalities.
v Given the current standard of care using these drugs, further
investigations should investigate how prolonged sedation with
opioids and benzodiazepines can affect brain development and
give rise to potential functional alterations later in life.
Hannah W. Kilcoyne, Russell W. Jennings, Patricia E. Grant, Dusica Bajic
Department of Anesthesiology, Perioperative and Pain Medicine, Boston Children’s Hospital, Harvard Medical School, Boston, MA
Table 1. Brain MRI Reports. Summary of individual neuroradiological findings for
patients analyzed (N=7) that included changes in (1) the extra-axial space, (2) parenchyma,
(3) tracts, and (4) other incidental findings that were not present in the controls (N=6). MRI
scans were analyzed by a neuroradiologist at Boston Children’s Hospital. Age at scan is
given in months. Only one patient had no pathological findings on the brain MRI report.
Figure 1. Average daily dose of drugs used for sedation and weaning: muscle relaxants
(rocuronium and cisatracurium), opioids (fentanyl, morphine, and methadone), and
benzodiazepines (midazolam and lorazepam) in full-term patients less than 6 months old (A, N=4),
and full-term patients 6 to 12 months old (B, N=3). Average daily dose (mg/kg/day ± SD) is shown
separately for sedation treatment and weaning periods. Fentanyl is presented in morphine
equivalents (10 mcg fentanyl = 1 mg morphine).
Figure 3. Daily dose (mg/kg) of individual patients over time for morphine (A and B) and
midazolam (C and D) in patient less than 6 months old (N=4) and those 6-12 months old (N=3).
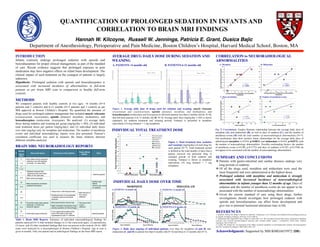
Fig. 5. Correlations. Graphs illustrate relationship between the average daily dose of
morphine (A), and midazolam (B), as well as days of sedation (C), and the number of
anesthesia events (D) with the total number of neuroradiological abnormalities (N=7).
Our preliminary data show positive linear relationships for the average daily dose of
administered morphine (r=0.934, p=0.0021) and midazolam (r=0.810, p=0.0272) with
the number of neuroradiology abnormalities. Possible confounding factors: the number
of anesthesia events (r=0.398, p=0.3772) and days of sedation (r=0.397, p=0.3784) do
not appear to be associated with the number of neuroradiology abnormalities.
BRAIN MRI: NEURORADIOLOGY REPORTS
AVERAGE DRUG DAILY DOSE DURING SEDATION AND
WEANING
Figure 2. Total treatment dose (sedation
and weaning) (mg/kg/day) of each drug for
each patient (N=7). Total treatment period
is defined as the total number of days that a
patient received one particular drug. It
included periods of both sedation and
weaning. Fentanyl is shown in morphine
equivalents (10 mcg fentanyl = 1 mg
morphine).
INDIVIDUAL TOTAL TREATMENT DOSE
INDIVIDUAL DAILY DOSE OVER TIME
CORRELATION to NEURORADIOLOGICAL
ABNORMALITIES
INTRODUCTION
Infants routinely undergo prolonged sedation with opioids and
benzodiazepines for proper clinical management, as part of the standard
of care. Recent evidence suggests that prolonged exposure to pain
medication may have negative effects on infant brain development. The
clinical impact of such treatment on the youngest of patients is largely
unknown.
Hypothesis: Prolonged sedation with opioids and benzodiazepines is
associated with increased incidence of abnormalities in full-term
patients as per brain MRI scan in comparison to healthy full-term
controls.
0
1
2
3
4
5
6
7
Cisatracurium Rocuronium Fentanyl Morphine Methadone Midazolam Lorazepam
AverageDailyDose(mg/kg/day)
Sedation Weaning
0
1
2
3
4
5
6
7
Cisatracurium Rocuronium Fentanyl Morphine Methadone Midazolam Lorazepam
AverageDailyDose(mg/kg/day)
Sedation Weaning
A. PATIENTS <6 months old B. PATIENTS 6-12 months old
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
5.5
6
6.5
7
7.5
8
TotalTreatmentDose(mg/kg/day)
Muscle Relaxants Opioids Benzodiazepines
Cisatracurium
Rocuronium
Fentanyl
Morphine
Methadone
Midazolam
Lorazepam
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5
#NeuroradiologicalAbnormalities
Average Daily Dose of Morphine during Sedation
(mg/kg/day)
r = 0.934
p = 0.0021
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
0 0.5 1 1.5 2 2.5 3 3.5
Average Daily Dose of Midazolam during Sedation
(mg/kg/day)
r = 0.810
p = 0.0272
A. Morphine B. Midazolam
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
0 5 10 15 20 25 30 35
#NeuroradiologicalAbnormalities
Days of Sedation
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
0 5 10 15 20 25
# of Anesthesia Events
r = 0.383
p = 0.397
C. Days of sedation D. Number of anesthesia events
r = 0.397
p = 0.3784
MIDAZOLAM
0
1
2
3
4
5
6
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
DailyDose(mg/kg)
1 2 3 4 5 6
0
1
2
3
4
5
6
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28
DailyDose(mg/kg)
1 2 3 4 5 6 7 8 9
Days of Sedation Days of Weaning
C. PATIENTS <6 months old
D. PATIENTS 6-12 months old
MORPHINE
0
1
2
3
4
5
6
7
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28
DailyDose(mg/kg)
1 2 3 4 5 6 7 8 9 10 11
0
1
2
3
4
5
6
7
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
DailyDose(mg/kg)
1 2 3 4 5 6 7 8 9 10 11
Days of WeaningDays of Sedation
A. PATIENTS <6 months old
B. PATIENTS 6 -12 months old
Acknowledgment: Supported by NIH K08DA035972 (DB).
REFERENCES
1. Anand KJ, Willson DF, Berger J, Harrison R, Meert KL, Zimmerman J, et al. Tolerance and withdrawal from prolonged opioid use
in critically ill children. Pediatrics. 2010 Apr 19;125:1208-25.
2. Andropoulos DB, Ahmad HB, Haq T, Brady K, Easley RB, et al. The association between brain injury, perioperative anesthetic
exposure, and 12-month neurodevelopment outcomes after neonatal cardiac surgery: a retrospective cohort study. Pediatric
Anesthesia. 2014 24:266-274.
3. Loepke AW, Soriano SG. An assessment of the effects of general anesthetics on developing brain structure and neurocognitive
function. Anesthesia & Analgesia. 2008 106(6):1681-1707