reStartEvents 5:9 DC metro & Beyond V-Career Fair Employer Directory.pdf
2. TRAUMATIC_INJURIES.pptx
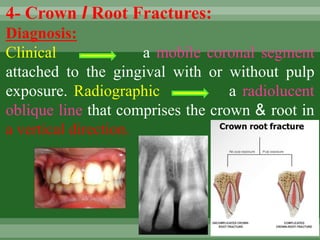
1. 4- Crown I Root Fractures:
Diagnosis:
Clinical a mobile coronal segment
attached to the gingival with or without pulp
exposure. Radiographic a radiolucent
oblique line that comprises the crown & root in
a vertical direction.
2. Treatment objectives
1- To maintain pulp vitality.
2- To restore normal esthetics & function.
3-To induce apical closure of incomplete roots of
permanent teeth.
3. Treatment:
1- Primary teeth:
If the tooth cannot be or should not be restored,
Extraction is the treatment of choice unless
removal of the apical fragment would result in
damage to the successor tooth bud.
II- Permanent teeth:
•Emergency treatment: stabilize (reattach) the
coronal fragment.
•Definite treatment: removal of the coronal
fragment followed by a supra-gingival
restoration.
4. a) If the fracture extends deeper sub-
gingivally, gingivectomy, osteotomy or
surgical or orthodontic extrusion is done
to prepare for restoration.
b) If the pulp is exposed, alternatives
treatment include; direct pulp capping,
pulpotomy or root canal treatment.
Prognosis:
Fractures extending deeply below the
gingival margin may not be restorable.
7. 5-Root Fractures:
Diagnosis:
Clinical : mobile coronal fragment
attached to the gingival that may be
displaced.
Radiographic : 1 or more, radiolucent lines
that separate the tooth fragment in
horizontal fractures. Multiple radiographic
exposures may be required for diagnosis
of other types of fractures.
8. Treatment objectives:
1. Reposition as soon as possible
2. Stabilize the coronal fragment in its
anatomically correct position to optimize
healing of the periodontal ligament &
neurovascular supply while maintaining
esthetic & functional integrity.
9. Treatment:
I- Primary teeth:
1. Extraction of the coronal fragment
without insisting on removing apical
fragment.
2. Wait & See is considered as alternative
treatment.
10. II- Permanent teeth:
A) Apical root fractures
No treatment is required, just follow-up
by x-rays up to 6 months.
Instruct the patient not to overload the
tooth
11. •1 month later, union may occur by a
calcific or fibrous tissue.
•If the fracture line increases in width,
this indicates failure of union RCT
followed by surgical removal of the
apical fragment.
12. B) Middle-third root fractures:
•Splinting is the treatment because the root part
attached to the crown isn't enough to stabilize the
tooth.
*Types of splints:
1- Composite splint: it is used when the adjacent
teeth are structurally healthy & well-aligned.
2- Light stainless steel wire splint.
3- Arch bar splint.
4- acrylic resin splint.
Teeth with root fractures should be splinted for 4-6
weeks.
13.
14. * Ideal requirements of a splint:
1- Quick & easy construction.
2- Stability throughout the healing period.
3- Should allow physiologic response of the
teeth.
4- Should allow easy access for Endodontic
treatment.
5- Should be passive & atraumatic.
6- Should be esthetically pleasant.
7- Shouldn't enhance plaque accumulation.
15. C) Cervical-third root fractures:
•If the fracture occurs at the bone level, the
coronal fragment is removed, RCT is
performed.
•If the fracture occurs 1-2 mm infrabony,
localized osteoplasty may be performed to
enable treatment followed by RCT.
•If the fracture is too far infrabony, then
extraction is the treatment of choice.
16. •Requisites of successful treatment of root
fractures:
1. The fragments must be in close contact.
2. The fragments must be immobilized.
3. Absence of infection.
*Patterns of healing of root fractures:
1. Healing by calcified tissue.
2. Healing by connective tissue.
3. Healing by bone & connective tissue.
4. Healing by granulation tissue.
17. Prognosis:
The best prognosis occurs in
1- Young age.
2- Immature roots.
3- Positive pulp response at the time of
injury.
4- Approximating the dislocation within I
mm.
Generally, apical fractures have better
prognosis than cervical ones.
18. 6. Concussion
Diagnosis:
Clinical : The tooth is tender to pressure &
percussion due to inflammation of the PDL
without mobility or sulcular bleeding.
Radiographic
There may or may not be thickening of the
periodontal ligament space.
Treatment objectives:
To optimize healing of the PDL & maintain
pulp vitality.
19. Treatment:
I- Primary teeth:
Unless associated infection exists, no pulpal
therapy is indicated.
II- Permanent teeth:
Although there is, a minimal risk of pulp
necrosis teeth with closed apices may undergo
pulpal necrosis due to associated injury to blood
vessels at the apex, & therefore must be
carefully followed-up.
Soft diet & analgesics .
20. Prognosis:
The younger the patient the better the
chances for tooth remaining.
Concussion may result in:
1- Asymptomatic pulp necrosis.
2- Discoloration of teeth.
3- Internal or external resorption.
4- No change & complete recovery.
21. 7. Subluxation:
Diagnosis:
C. P.
Mobile tooth without displacement which may or
may not have sulcular bleeding.
Radiographic
No change.
Treatment objectives:
To enhance healing of the PDL & neurovascular
supply.
Treatment:
I- Primary teeth:
Followed-up .
22. II- Permanent teeth:
Tooth stabilization & relieve any occlusal
interference.
For comfort, a flexible splint can be used for less
than 2 w.
Prognosis:
Primary tooth usually returns to normal within 2
weeks.
Mature permanent teeth may undergo pulpal
necrosis, so must be carefully followed-up.
23. 8. Lateral Luxation
Diagnosis
C.P.
-The tooth is displaced laterally with the crown
usually in a palatal or lingual direction & may
be locked firmly into this new position.
- The tooth is usually not mobile nor tender to
touch.
Radiographic: Increase in the periodontal
ligament space & displacement of the apex.
24. Treatment
I- Primary teeth
Allow passive repositioning or actively reposition
& splint for 2 weeks to allow for healing.
If injury is severe or the tooth is nearing
exfoliation Extraction.
II- Permanent teeth
•Reposition and stabilization as soon as possible
in its anatomically correct position to optimize
healing of the PDL & neurovascular supply,
while maintaining esthetic & functional integrity.
25. •Repositioning of the tooth is done with
digital pressure & little force.
•The tooth may extruded to free apical
lock in the cortical bone.
Splinting an additional 2-4 weeks may
be needed with breakdown of marginal
bone.
26. Prognosis:
Active repositioning increased risk of
pulp necrosis compared to teeth that are
left for passive repositioning.
In mature permanent teeth with closed
apices, pulp necrosis & obliteration are
common healing complications while
progressive root resorption is less likely to
occur.
27. 9. Intrusion:
C.P.
The tooth appears to be shortened or missed in
severe cases (more than 6 mm intrusion).
The tooth apex is usually displaced labially
towards or through the labial cortical plate of
bone in primary teeth or driven into the alveolar
process in permanent teeth
The tooth isn't mobile or tender to touch.
28. Radiographic
•Tooth appears to be displaced apically & the
PDL isn't continuous.
•The relationship of the intruded primary tooth
and the successor's tooth follicle should be
determined;
•If the apex is displaced labially, the apical tip can
be seen radiographically with the tooth appearing
shorter than its contralateral.
29. •If the apex is displaced palatally towards the
permanent tooth germ, the apical tip won't be
seen radiographically & the tooth appears
elongated.
Extra-oral lateral radiograph may be used to
detect displacement of the apex towards or
through the labial plate of bone.
•An intruded young permanent tooth may
mimic an erupting tooth.
30. Treatment:
I- Primary teeth:
Spontaneous re-eruption (within 3-4W.) unless it
endangering the developing tooth germ, otherwise
Extraction is indicated.
II- Permanent teeth:
Passive repositioning.
Active repositioning (Traction) or surgical
repositioning if intrusion is greater than 6mm.
Tooth stabilization to allow PDL healing & maintain
esthetic & function
Intrusion greater than 6 mm
indicates surgical
repositioning
31. •In mature teeth, reposition the tooth via
surgical or orthodontic extrusion & initiate
endodontic treatment within 3 weeks of the
traumatic incidence.
•In teeth with immature root formation, the
objective is to allow spontaneous eruption.
32. Prognosis:
1- Primary teeth:
90% re-erupt spontaneously (either partially or
completely) in 2-6 months. Even in cases of complete
intrusion & displacement of primary teeth through the
labial plate, re-eruption may occurs for more than 36
months.
Ankylosis may occur if the periodontal ligament was
severely damaged, thereby delaying or altering the
eruption of the permanent successor.
33. Complications following intrusion of primary teeth:
1-Dilacerations:
It occurs in permanent successors of intruded primary
teeth where the calcified portion is twisted providing a
new direction of growth. It may lead to a sharp angle
between the crown and the root.
2-Gemination:
Partial duplication of the affected teeth in that part of the tooth
formed after injury.
35. II- Permanent teeth:
• Mature teeth with closed apices have a risk for
pulp necrosis, pulp canal obliteration, and
progressive root resorption.
• Immature teeth that are allowed to reposition
spontaneously show the lowest risk for
complications.
• An intrusion of 7 mm or more have a negative
influence on healing.
36. Primary dentition
0pen apex
Closed apex /
less than 5
mm intrusion
Allow 6
months for
spontaneous
re-eruption &
advise the
parents about
the potential
the damage to
the tooth
Extract the tooth if
root tip is displaced
into the permanent
tooth bud
Permanent dentition
Closed
apex/greater than
6 mm intrusion
INTRUSION INJURIES
Consider
slight surgical
Luxation &
allow for
spontaneous
re-eruption or
orthodontic
repositioning.
-surgical
repositioning
&physiological
splinting for 1-2
weeks of injury
-Ca(OH)2
pulpectomy
within tow weeks
of the injury.
-surgical or
orthodontic
repositioning.
-Ca(OH)2
pulpectomy
within two
weeks of the
injury.
Follow up is recommended to monitor signs
of pathology, via radiographs.
-Follow up for 4 weeks.
-Advise the parents about
possible.
37. 10. Extrusion:
(partial Avulsion)
Diagnosis:
C.P.
The tooth appears elongated & is mobile.
Radiographic findings:
An increase in the width of the periodontal ligament space
apically.
Treatment:
I- Primary teeth:
Reposition and splinting the tooth for 1-2 weeks & allow for
healing, except when there are indications for extraction
(e.g.: sever injury or exfoliation).
38. II- Permanent teeth:
•Reposition the tooth as soon as possible & then
stabilize the tooth in its anatomically correct position
to optimize healing of the periodontal ligament &
neurovascular supply while maintaining esthetic &
functional integrity.
•Repositioning may be done with slow & steady
apical pressure to gradually displace the coagulum
formed between the apex & the floor of the socket
•Splint the tooth for up to 3 weeks.
39. Prognosis:
•There is a lack of clinical evidence
evaluating repositioning of extruded
primary teeth ( NO DATA).
•In mature permanent teeth with closed
apices, there is a considerable risk for
pulp necrosis & pulp canal obliteration,
therefore these teeth must be followed-up
carefully.
41. 11. Avulsion:
Diagnosis:
Clinical & radiographic features:
Reveal that the tooth is not present in its socket or
that the tooth already has been replanted.
Treatment Objectives:
I- Primary teeth:
To prevent further injury to the developing successor,
Avulsed primary teeth should not be replanted.
42. II- Permanent teeth:
Replant & stabilization the tooth as soon as
possible in its anatomically correct position to
optimize healing of the periodontal ligament
and neurovascular supply while maintaining
esthetic and functional integrity, except when
replantation is contraindicated.
43. Contraindications of tooth replantation:
1-The child's stage of dental development (the risk of
ankyloses where considerable alveolar growth has to take
place)
2-Compromising medical condition; such as:
Immunocompromise, severe congenital cardiac anomalies,
severe uncontrolled seizure disorder, severe mental disability
& severe uncontrolled diabetes.
3-Compromised integrity of the avulsed tooth or the
supporting structures.
Treatment:
The treatment strategies are directed towards avoiding the
inflammation that may occur as a result from the tooth's
attachment damage and/or pulpal infection.
44. Technique of replantation:
1- Patient preparation:
Inform the parents -and if possible, the patient-
about: - The need for splinting, for 1-2 weeks.
•The need for RCT, 1-2 weeks after replantation.
•The uncertain prognosis of tooth replantation.
the cementum.
45. 2- Tooth preparation:
•The tooth is held from the crown.
•The dentist should avoid using any brush or sharp
instrument on the root surface as it might remove
remnants of the periodontal fibers and exposed the
cementum.
46. 3- Socket preparation:
•The socket and the surrounding tissues should
be carefully inspected and cleaned with sterile
saline.
•Use a soft tissue curette to remove any
coagulated tissue from the socket, then
carefully irrigate the socket.
47. 4- Tooth replantation:
The tooth is placed into the socket carefully using
gentle pressure.
5- Checking occlusion:
The replanted tooth should be free of contact
with the opposing teeth to avoid overloading the
tooth, which may interfere with proper
reattachment.
6- Splinting:
Flexible splinting for 1-2 weeks is indicated.
48. Prognosis:
depends on:
A) The stage of root development:
The chance for revascularization is better in case
of open apices than in case of closed apices.
B) The extra-oral dry time:
The tooth has the best prognosis if replanted
immediately. If the tooth cannot be replanted
within 5 minutes, it should be stored in a medium
that will help to maintain vitality of the periodontal
ligament fibers.
49. Transportation media for avulsed teeth:
1- Viaspan.
2-Hank's balanced salt solution-HBSS-
(tissue culture medium).
3- Cold milk.
4- Saliva (buccal vestibule or floor of the
mouth).
5- Physiologic saline or water.
50. Limited tooth storage in a cell-compatible medium
prior to replantation has produced similar healing
results as compared with immediately replanted
teeth.
The risk of ankylosis increases with an extra-oral dry
time of 15 minutes. An extra-oral dry time of 60
minutes is considered as the crtical point where
survival of the periodontal cells is unlikely to occur..
In permanent anterior teeth, there is a considerable
risk for pulp necrosis, root resorption, ankylosis, and
subsequent infra-occlusion during adolescent
growth.
51. First aid for avulsed teeth
1-Keep the patient calm
2-Find the tooth & pick
it up by the crown
3-Clean the tooth 4-Place the tooth in a
suitable storage medium
Seek emergency dental treatment immediately