1. Composite Scaffolding made from Poly(Lactic Acid) and β-Tricalcium phosphate
Eric Queen B.S. in Chemistry
Sterling College
All surgeries that were performed on the sheep were without complication.
All the sheep made full recoveries after surgery and showed no signs of
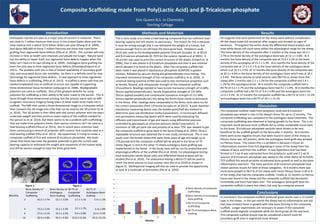
lameness. Throughout the entire study the differential blood analysis and
total white blood cell count were within the physiological range for the sheep.
The bone density of the composite after 2 months in the sheep was 10.2 ±
3.7% vs the bone density of the autologous bone was at 12.1 ± 3.0%. At 4
months the bone density of the composite was at 13.2 ± 3.1% vs the bone
density of the autologous at 15.1 ± 3.3%. At 6 months the bone density of the
composite was at 17.4 ± 4.1 % vs the bone density of the autologous bone
which is at 19.3 ± 3.5%. At 12 months the bone density of the composite was
at 30.3 ± 4.6% vs the bone density of the autologous bone which was at 34.1
± 4.4%. The bone volume to total volume ratio (BV:TV) as shown from the
sheep after 2 months was 2.1 ± 1.1% for the composite scaffold and 2.4 ±
1.2% for the autologous bone. At 4 months the composite scaffold had a
BV:TV of 3.2 ± 1.7% and the autologous bone had 4.1 ± 1.8%. At 6 months the
composite scaffold had a BV:TV of 9.4 ± 4.8% and the autologous bone has
12.4 ± 4.3%. At 12 months the composite scaffold has a BV:TV of 23.0 ± 12.2%
and autologous bone has a BV:TV of 24.1 ± 13.1%.
Introduction
The in vitro study is to create a load bearing composite that has sufficient load
bearing capacity but still retains its porousness. The reason for this is because
it must be strong enough that it can withstand the weight of a human, but
porous enough that it can still have the bone grow back. Poly(lactic acid)
(PLA) was used as the biodegradable polymer (Fraczek-Szczypta et. al 2012)
and β-tricalcium phosphate (β -TCP) for the ceramic (Ignatius et al 2001). A
3D printer was used to print the correct structure of the plastic (Colwell et. al
2006), then it was placed in β-tricalcium phosphate and then it was sintered
which allowed it to bond to the plastic. After the composite scaffold had
been made it was placed in dipotassium phosphate (K2HPO4) in gelatin
solution, followed by vacuum drying and glutaraldehyde cross-linking. This
improved mechanical strength of the composite scaffold (J et al. 2010). A
universal testing machine (UTM) was used to test mechanical properties such
as tensile, flexural, and compressive strength of the composite scaffold
(TiniusOlsen). Readings needed to have tensile transverse strength of 53 MPa
(forces applied perpendicular), tensile longitudinal strength of 135 MPa
(forces applied parallel) and compressive transverse strength of 131 MPa
(forces applied perpendicular) this being the forces bone needs to withstand
in the femur. After readings were comparable to the femur tests were run for
the correct porousness (Park ) (Fraczek-Szczypta et. al 2012). A pore diameter
distribution measuring device uses the bubble point/half-dry method to
determine pore size distribution (Seika Corporation). A microscopic diffusion
and permeation measuring device which were used by evaluating the
diffusion and transmission of gas and vapors using differential pressure
controlled by gas/vapors at ultra-low pressure (Seika Corporation). A
minimum of 180 µm pore size and porosity of at least 75% was needed to get
the composite scaffold to grow back to the bone (Chang et al. 2003). Once a
repeatable structure was obtained the in vivo study commenced. The in vivo
study used 150 female sheep that were three years of age and weigh up to
170 pounds and the composite scaffold will be placed in the femur of 75
sheep (figure 1) and in the other 75 sheep autologous bone grafting was
implemented in the femur. In the study, tests will be run for anatomical and
physiological effects of the scaffold (Pol et al. 2010). For physiological testing
total leukocytes (white blood cells) and differential blood analysis will be
studied (Pol et al. 2010). For anatomical testing a Micro-CT will be used to
check the bone volume to total volume ratio (Pol et al 2010) as shown in
(figure 2). Multispectral imaging will also be used to provide the opportunity
to look at a multitude of biomarkers (Pol et al. 2010).
Methods and Materials
The composite scaffold made from poly(lactic acid) and β-tricalcium
phosphate was tested in vivo in the sheep’s femur for up to 12 months. The
composite scaffolding was compared to the autologous bone treatment. The
composite scaffolding was observed at having growth to the bone. This is an
important result because most scaffolds fail to create sustainable tissue back
to the bone. β-tricalcium phosphate particles were shown to be very
beneficial to the scaffold growth to the bone after 2 months. At 4 months
there were some negative results that were found in some of the sheep as
fibrous tissue was still present, while the autologous bone graft was showed
no fibrous tissue. The reason this is a problem is because it shows an
inflammatory reaction from PLA degrading in some of the sheep from the
release of lactic acid from the scaffold. A new hypothesis that has been
formed is if 3 wt.% was subtracted from the poly(lactic acid) and if 3 wt.%
amount of β-tricalcium phosphate was added to the initial 38/62 wt.% PLA/b-
TCP scaffold this would promote accelerated bone growth as well as decrease
inflammatory reactions. The more particles of β-tricalcium phosphate have
shown positive results for both of those categories. At 6 months there was
more bone growth in 98.0 % of the sheep with minor fibrous tissue in 85.0 %
of the sheep that had the composite scaffold. Finally at 12 months no fibrous
tissue was found in the sheep and the composite scaffold had decreased
remarkably and bone had taken over. The autologous bone graft beat the
composite scaffold in every test taken, but only by a marginal amount.
Discussion
In conclusion, the composite scaffold produced great results over a 12 month
span in the sheep. In the last month the sheep had no inflammation and still
had slow constant bone in-growth with new bone forming in the composite
scaffold. Longer experiments are necessary to assess if the composite
scaffold would degrade completely while the bone grows all the way back.
This composite scaffold should now be considered a bench mark for
secondary graft sites in segmental bone disease.
Conclusions
Orthopedic injuries are seen as a major area of concern in medicine. There
are close to 7 million fractures that occur in the United States alone and the
total medical cost is about $215 billion dollars per year (Zhang et al. 2009).
And about 800,000 of those 7 million fractures are those that need bone
grafting from segmental bone defects (Pilia et al. 2013). This number will only
increase in time as health care improves and people live longer. Natural bone
has the ability to repair itself, but segmental bone defects happen when the
body can’t heal on its own (Zhang et al. 2009). Autologous bone grafting has
been the only way to treat segmental bone defects (Dhandayuthapani et al.
2011). The problem with this is that of limited availability of secondary graft
sites and associated donor site morbidity. So there is a definite need for new
technology for segmental bone defects. A new approach to treat segmental
bone defects is scaffolding. (Pilia et al. 2013). A scaffold is when cells that are
seeded (implanted) into an artificial structure are capable of supporting
three-dimensional tissue formation (Lebourg et al. 2008). Biodegradable
polymers are used as scaffolds. One of the greatest benefits for using
polymers for scaffolding is their ability to be tailor made to the person. This is
done through three dimensional printing, but the process starts with an MRI
(magnetic resonance imagery) being taken of what needs to be made into a
scaffold. The MRI then sends a three dimensional image to a computer which
then converts the 3D image into a file that can be read by the 3D printer (Li et
al. 2014). The 3D printer is then filled with the correct polymer with the exact
molecular weight and then prints an exact replica of the scaffold needed for
the person (Li et al. 2014). But there seems to be a problem with scaffoldings
that are made from polymers alone, their porous construct can’t be used as a
load bearing scaffold (Pilia et al. 2013). But in recent years scientists have
been constructing a mixture of polyester with ceramic that could be used as a
load bearing scaffold (Pilia et al. 2013). My experiment is trying to create a
composite scaffold of PLA and sintered β-tricalcium phosphate. My study
shows that these two have the greatest potential to give the correct load
bearing capacity to withstand the weight and movement of the human body
and still be porous enough to have the bone grow back.
Results
Figure 1. Figure 2.
0
5
10
15
20
25
30
35
40
2 4 6 12
Months
Bone density of Composite
Scaffolding
Bone Density of Autologous
bone grafting
BV:TV of Composite
Scaffolding
BV:TV of Autologous Bone
Grafting
Months
Bone Density of
Composite
Scaffolding
Bone Density of
Autologous
Bone Grafting
BV:TV of
Composite
Scaffolding
BV:TV of
Autologous Bone
Grafting
2 10.2 ± 3.7% 12.1 ± 3.0% 2.1 ± 1.1% 2.4 ± 1.2%
4 13.2 ± 3.1% 15.1 ± 3.3% 3.2 ± 1.7% 4.1± 1.8%
6 17.4 ± 4.1% 19.3 ± 3.5% 9.4 ± 4.8% 12.4 ± 4.3%
12 30.3 ± 4.6% 34.1 ± 4.4% 23.0 ± 12.2% 24.1± 13.1%