6. How frequently do adrenal masses occur?
Incidentally discovered adrenal tumors: an institutional perspective. Herrera MF, Grant CS, van Heerden JA, Sheedy PF, Ilstrup DM Surgery. 1991;110(6):1014. .
7. Anatomy
Townsend, C.M., R Daniel Beauchamp, B Mark Evers, Mattox, K.L. and Christopher, F. (2017). Sabiston textbook of surgery : the biological basis of modern surgical practice. Philadelphia, Pa: Elsevier.
8. Townsend, C.M., R Daniel Beauchamp, B Mark Evers, Mattox, K.L. and Christopher, F. (2017). Sabiston textbook of surgery : the biological basis of modern surgical practice. Philadelphia, Pa: Elsevier.
9. Townsend, C.M., R Daniel Beauchamp, B Mark Evers, Mattox, K.L. and Christopher, F. (2017). Sabiston textbook of surgery : the biological basis of modern surgical practice. Philadelphia, Pa: Elsevier.
10. Moore, K.L., Agur, A.M.R. and Dalley, A.F. (2015). Essential clinical anatomy. Philadelphia: Wolters Kluwer Health
24. Role for biopsy?
Biopsy if,
• Inactive
• Inconclusive Imaging
• Alter management
• Infective/Infiltrative process
• Inoperable tumour for
oncology
Issues
• Non-superior sensitivity
• Risk of dissemination
• Technical
Bancos I, Tamhane S, Shah M, Delivanis DA, Alahdab F, Arlt W, Fassnacht M & Murad MH. The diagnostic performance of adrenal biopsy: a systematic review and meta-
analysis. European Journal of Endocrinology 2016. In Press.
25. Evaluation for Hormonal Secretion
1. Subclinical Cushings (6.4%)
2. Pheochromocytoma (3.1%)
3. Primary Aldosteronism (0.6%)
90% are Non-functional!
27. Pheochromocytoma
Palpitations
Perspiration
Pain in the
Head
Fassnacht, M., Arlt, W., Bancos, I., Dralle, H., Newell-Price, J., Sahdev, A., Tabarin, A., Terzolo, M., Tsagarakis, S. and Dekkers, O.M. (2016). Management of adrenal incidentalomas: European Society of
Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. European Journal of Endocrinology, [online] 175(2), pp.G1–G34.
33. Open Adrenalectomy (Anterior)
1. Extended subcostal incision OR midline
2. Division of triangular ligament
3. Kocher maneuver (Right) / Splenic & Pancreatic reflection (Left)
4. Medial dissection (IVC & Tumour)
5. Adrenal vein ligation (midportion adrenal)
6. Gentle, indirect adrenal traction
7. Clockwise dissection
8. Haemostasis, Haemostasis, Haemostasis
Fischer, J.E., Bland, K.I., Ovid Technologies, Inc and Al, E. (2007). Mastery of surgery. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins.
34. Laparoscopic Adrenalectomy (Lateral Transabdominal)
Townsend, C.M., R Daniel Beauchamp, B Mark Evers, Mattox, K.L. and Christopher, F. (2017). Sabiston textbook of surgery : the biological basis of modern surgical practice. Philadelphia, Pa: Elsevier.
35. Laparoscopic Adrenalectomy (Lateral Transabdominal)
Townsend, C.M., R Daniel Beauchamp, B Mark Evers, Mattox, K.L. and Christopher, F. (2017). Sabiston textbook of surgery : the biological basis of modern surgical practice. Philadelphia, Pa: Elsevier.
You only have to spend one week in surgery before you will be forced to head down to xrays and negotiate for an urgent CT . And upon completing a week of wards and undertaking that journey to xrays numerous times, you will be well aware of the sheer number of CT’s done at CMH in a week.
This is a testament to a world wide phenomenon of better access to and more liberal use of CT. The very same phenomenon that’s driven the incidental detection of subclinical or completely asymptomatic adrenal masses.
So today my talk will focus on adrenal masses from the perspective of the entity termed “Incidentalomas”…
We’ll take a look a what incidentalomas are, how common adrenal tumours are; the clinically applicable basic sciences; before considering the types of adrenal masses one encounters and the development of an approach centred on phenotyping & functional status before finally focusing on surgical management & Perioperative care
An adrenal incidentaloma is an adrenal mass detected on imaging not performed for suspected adrenal disease. By this strict definition, the imaging study is not done for symptoms related to adrenal hormone excess (e.g. pheochromocytoma, Cushing’s or Conn’s syndrome) or an otherwise suspected adrenal mass, but rather for the evaluation of symptoms that are not obviously related to an adrenal problem, such as abdominal or back pain or kidney stones.
**show sequence of imaging
The incidence and prevalence of adrenal incidentalomas has largely been extrapolated from imaging or autopsy studies.
In a study of 61,054 abdominal CT scans performed from 1985 to 1990, an incidental adrenal tumor (incidentaloma >1 cm) was detected in 259 patients (0.4 percent of all CT scans) [3]. Incidentally discovered adrenal tumors: an institutional perspective. Herrera MF, Grant CS, van Heerden JA, Sheedy PF, Ilstrup DM Surgery. 1991;110(6):1014.
The prevalence is higher in obese, diabetic, and hypertensive patients
Radiological studies report a frequency of around 3% in the age of 50 years, which increases up to 10% in the elderly. In childhood, adrenal incidentalomas are extremely rare
The prevalence of adrenal incidentaloma is higher in older patients (10 percent) [5].
In autopsy studies, the prevalence of incidentalomas is 2 percent, and it ranges from 1 to 9 percent. The prevalence is higher in obese, diabetic, and hypertensive patients
AME position statement on adrenal incidentaloma. Terzolo M, Stigliano A, Chiodini I, Loli P, Furlani L, Arnaldi G, Reimondo G, Pia A, Toscano V, Zini M, Borretta G, Papini E, Garofalo P, Allolio B, Dupas B, Mantero F, Tabarin A, Italian Association of Clinical Endocrinologists .Eur J Endocrinol. 2011;164(6):851. Epub 2011 Apr 6.
The adrenals are paired retroperitoneal glands that lie superiorly and anteromedially to the kidneys.
They are triangular-shaped with the right adrenal gland being usually more pyramidal in shape while the left is more crescenteric, hanging over the medial end of the kidney [8].
The adrenals are supplied by three arteries: superior (from the inferior phrenic arteries), middle (from the abdominal aorta), and inferior suprarenal arteries (from the renal arteries).
In terms of relational anatomy,
Both glands are enclosed in the renal fascia (fascia of gerota) which are attached to the crura of the diaphragm, with the diaphragm being their major point of attachment and a thin septum separating them from the kidneys.
The left adrenal gland is related anteriorly to the body of the pancreas and then largely surrounded by the diaphragm
Whereas the right adrenal gland is related anteriorly to the inferior vena cava, laterally to the liver and posteriorly to the right crus of the diaphragm
The left adrenal vein varies little and is usually confluent with the left inferior phrenic vein, finally draining into the left renal vein.
The right adrenal on the other hand is prone to much variation coupled with a relatively short course and propensity to be confluent with the IVC
A, Territory of potential right adrenal vein confluence.
B, Normal (>80%); single vein directly into the inferior vena cava (IVC).
C, IVC–renal vein trifurcation.
D, Renal vein confluence
E. High single vein into the IVC.
F, IVC–right hepatic vein trifurcation.
G, Right hepatic vein confluence.
Lymphatic drainage is achieved by para-aortic lymph nodes.
. Moore, K.L., Agur, A.M.R. and Dalley, A.F. (2015). Essential clinical anatomy. Philadelphia: Wolters Kluwer Health.
The adrenal glands have two embryonic origins, and consequently produce two different types of signalling chemicals. The outer cortex is of mesodermal origin and releases steroidal hormones, while the inner medulla is derived from ectoderm (arises from the neural crest) and secretes adrenergic neurotransmitters (also known as catecholamines).
In the cortex, the zona glomerulosa produces mineralocorticoids, the zona fasciculata glucocorticoids, and the zona reticularis sex steroids or gonadocorticoids, whereas the medulla produces catecholamines, adrenaline, and noradrenaline.
So in essence the Mineralocorticoids cause sodium and water rentention while losing potassium in the urine
Your glucocorticoids mobilize protein and fat stores, converting them into glucose under stressful situations
While your catecholamines run your fight or flight response, increasing heart rate, blood pressure and overall metabolic rate.
lung cancer
colorectal carcinoma
breast cancer
pancreatic cancer
With a newly identified adrenal lesion, there are two primary questions which will guide further management. First, could this mass be malignant? Second, is this mass functional? That is, are there any physical signs and symptoms or biochemical evidence of excess hormonal activity that could be attributed to excess secretion of an adrenally derived hormone.
.
Unenhanced CT scan is the first line test of choice. In more than 70% of cases, it is possible to identify adrenal adenomas on the basis of this test alone. Low attenuation (<10 HU) is the characteristic finding on this study. Enhanced CT with adrenal washout protocols may be used where unenhanced CT is unclear. Adenomas exhibit characteristic rapid enhancement washout after administration of CT contrast. MRI is an alternative to CT scan. Again, there are characteristic findings of adrenal adenomas including a loss of signal intensity of out-of-phase sequences.5
Imaging findings help to guide the answer to the question of whether a given adrenal lesion may be malignant. There is a relationship between the size of an adrenal lesion and the likelihood of malignancy. Thus, all lesions larger than 6 cm should be considered malignant until proven otherwise. Due to diagnostic uncertainty, may would advocate resection for lesions 4 cm or larger.1 Additionally, as the incidence of benign lesions increases with age, additional concern should be taken for younger patients with even small adrenal lesions. On axial imaging, ACC exhibit increase attenuation on non-contrast CT, irregular borders and enhancement, and calcification and necrosis.
Unenhanced CT scan is the first line test of choice. In more than 70% of cases, it is possible to identify adrenal adenomas on the basis of this test alone. Low attenuation (<10 HU) is the characteristic finding on this study.
Metanalysis evidence on the accuracy of imaging tests for differentiating malignant from benign adrenal masses.
The data suggest that CT density >10 HU has high sensitivity for the detection of malignancy, the 95% CI suggesting that this is above 90%. However, all other estimates of test performance are based on small numbers of studies with few patients, and 95% CIs are notably wide, indicating uncertainty in test performance for all other imaging markers. There is no clear superiority between CT/MRI/orPET CT but given the ease of CT- it is preferred.
3 imaging parameters guide the CT interpretation of adrenal incidentalomas
Adrenocortical carcinomas were significantly associated with mass size, with 90 percent being more than 4 cm in diameter when discovered. Adrenal mass size is also important because the smaller the adrenocortical carcinoma is at the time of diagnosis, the better the overall prognosis.
Adrenocortical carcinomas were significantly associated with mass size, with 90 percent being more than 4 cm in diameter when discovered. Adrenal mass size is also important because the smaller the adrenocortical carcinoma is at the time of diagnosis, the better the overall prognosis
2nd aspect of imaging characterization over and above size is the attenuation of the mass
unenhanced attenuation — On computed tomography (CT) scanning, the density of the image (black is less dense) is attributed to radiograph attenuation. The intracytoplasmic fat in adenomas results in low attenuation on unenhanced CT; non-adenomas have higher attenuation in unenhanced CT. The Hounsfield scale is a semiquantitative method of measuring radiograph attenuation.. If an adrenal mass measures <10 HU on unenhanced CT (ie, has the density of fat), the likelihood that it is a benign adenoma is nearly 100 percent. However, up to 30 percent of adenomas do not contain large amounts of lipid and may be indistinguishable from non-adenomas on nonenhanced CT scans and are termed lipid-poor adenomas.
Clinical utility of noncontrast computed tomography attenuation value (hounsfield units) to differentiate adrenal adenomas/hyperplasias from nonadenomas: Cleveland Clinic experience. Hamrahian AH, Ioachimescu AG, Remer EM, Motta-Ramirez G, Bogabathina H, Levin HS, Reddy S, Gill IS, Siperstein A, Bravo EL .J Clin Endocrinol Metab. 2005;90(2):871. Epub 2004 Nov 30.
●HU>10 – In a retrospective cohort study of 353 patients with adrenal nodules who underwent adrenal biopsy and/or adrenalectomy, Adrenal masses with unenhanced CT attenuation >10 HU diagnosed malignancy with a sensitivity of 100 percent, specificity of 33 percent, positive predictive value (PPV) of 72 percent, and negative predictive value (NPV) of 100 percent. Unenhanced CT attenuation of ≤10 HU excluded malignancy even in this high-risk population.
For small tumours with attenuations of >10 HU we can assess the absorption of and rapidity of contrast washout on CT scan
On delayed contrast-enhanced CT, adenomas typically exhibit rapid contrast medium washout, whereas non-adenomas have delayed contrast material washout [16]. Ten minutes after administration of contrast, an absolute contrast medium washout of more than 50 percent was reported to be 100 percent sensitive and specific for adenoma when patients with adenomas were compared with carcinomas, pheochromocytomas, and metastases [16,18,19]
Contrast-enhanced washout CT utilizes the unique perfusion pattern of adenomas. Adenomas take up intravenous CT contrast rapidly, but also have a rapid loss of contrast – a phenomenon termed ‘contrast
enhancement washout’. It is assumed that malignant adrenal lesions usually enhance rapidly but demonstrate a slower washout of contrast medium. This washout phenomenon can be quantified by ‘contrast washout values’, which involve lesion attenuation measurements at specific time points acquired in a dedicated adrenal CT: before injection of contrast medium (HUnativ), at
60 s following injection of contrast medium (HUmax) and
then at 10 or 15 min after contrast injection. This allows
calculation of the relative contrast enhancement washout
(=100 × (HUmax − HU10/15 min)/HUmax) and absolute contrast
enhancement washout (=100 × (HUmax − HU10/15 min)/
(HUmax − HUnativ)). A relative washout >40% and an
absolute washout >50% is assumed to suggest that an
adrenal lesion is benign
Performance of adrenal biopsy in the diagnosis of malignancy overall was:
sensitivity 87% (CI: 95% of 78–93%), specificity 100%
(CI: 95% of 76–100%), positive likelihood ratio of 229
(CI: 95% of 2.9–18145) and negative likelihood ratio
of 0.13 (CI: 95% of 0.07–0.23). Performance was lower
(and with even wide 95% CIs) for ACC: sensitivity
70% (CI: 95% of 42–88%), specificity 98% (CI: 95% of
86–100%), positive likelihood ratio of 100.43 (CI: 95%
of 8–1245) and negative
We suggest performing a biopsy of an adrenal mass only if all of the following criteria are fulfilled (i) the lesion is hormonally inactive (in particular, a pheochromocytoma has been excluded), (ii) the lesion has not been conclusively characterized as benign by imaging and (iii) management would be altered by knowledge of the histology.
Adrenal biopsy has a limited role in evaluation of adrenal masses –some value in infiltrative or infectious process.
Even in such situations, adrenal biopsy should only be performed by
an experienced radiologist and when it is required to
guide further care. We particularly recommend against
an adrenal biopsy if an adrenal mass is likely to be an
adrenocortical carcinoma, because a biopsy of such a
tumor runs the risk of tumor dissemination precluding
an R0 resection (although this risk seems to be low (180)).
The only exception might be if a formal confirmation of
While most adrenal incidentalomas are nonfunctional, 10 to 15 percent secrete excess amounts of hormones.
The most complete analysis of this issue comes from a review of all 828 published articles on adrenal incidentalomas from 1980 to 2008.
Malignant – Primary adrenal carcinoma 1.9 percent, metastases 0.7 percent
●Benign – Nonfunctioning 89.7 percent, subclinical Cushing's syndrome 6.4 percent, pheochromocytoma 3.1 percent, primary aldosteronism 0.6 percent
Recommended evaluation of adrenal incidentalomas is costly, has high false-positive rates and confers a risk of fatal cancer that is similar to the risk of the adrenal lesion becoming malignant; time for a rethink? Cawood TJ, Hunt PJ, O'Shea D, Cole D, Soule S . Eur J Endocrinol. 2009;161(4):513. Epub 2009 May 13.
An abnormal 1 mg overnight DST (cortisol >1.8 mcg/dL [>50 nmol/L]) is consistent with ACTH-independent autonomous cortisol production, a finding that should be further evaluated with 24-hour urinary free cortisol, serum ACTH concentration, and a high-dose (8 mg) overnight DST. Clinically significant glucocorticoid secretory autonomy is confirmed by a post-overnight 8 mg DST 8 AM serum cortisol concentration >1.8 mcg/dL (>50 nmol/L). (See "Establishing the diagnosis of Cushing's syndrome".)
In the past, it was thought that all patients with pheochromocytoma are symptomatic. However, with widespread use of computed imaging, pheochromocytomas are being discovered in the presymptomatic stage [51,52]. In a study of 271 consecutive patients with pheochromocytoma treated from 2005 to 2016, 61 percent were discovered as an incidental finding on cross-section imaging, 27 percent due to pheochromocytoma-related symptoms, and 12 percent due to mutation-based testing [53].
Pheochromocytoma Characteristics and Behavior Differ Depending on Method of Discovery. Gruber LM, Hartman RP, Thompson GB, McKenzie TJ, Lyden ML, Dy BM, Young WF, Bancos I . J Clin Endocrinol Metab. 2019;104(5):1386.
Biochemical testing for pheochromocytoma should be performed if the unenhanced CT attenuation is ≥10 HU, but not if it is <10 HU
Small pheochromocytomas (eg, <1.5 cm) may have normal biochemical testing (image 8). Pheochromocytomas need a critical mass before they can become biochemically detectable.
Consider surgery for lipid poor, non functioning and vascular adrenal masses
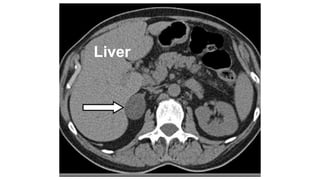
Unenhanced (A) and enhanced (B) axial CT images from a 49-year-old man who presented with right-sided abdominal discomfort. A 1.6 cm left adrenal mass was incidentally discovered (arrows). On the unenhanced image, the CT attenuation was 40 HU and diagnostic of a lipid-poor mass. With contrast administration, the adrenal nodule was very vascular (B) and had slow contrast washout (<50% at 10 minutes). The patient was normotensive and had no signs or symptoms of adrenal-related disease. The plasma fractionated metanephrines and 24-hour urine fractionated metanephrines and catecholamines were normal. However, in view of the suspicious imaging phenotype and the patient's young age, surgical resection after alpha-adrenergic blockade was advised. On pathology, it proved to be a 2.1 × 1.7 × 1.3 cm pheochromocytoma.
Aldosteronomas are rare (less than 1 percent) causes of an adrenal incidentaloma. However, because the majority of patients with primary aldosteronism are not hypokalemic, all patients with hypertension and an adrenal incidentaloma should be evaluated by measurements of plasma aldosterone concentration and plasma renin activity [1,2]. In addition, patients who are normotensive but have spontaneous hypokalemia should also be tested for primary aldosteronism
All patients with documented pheochromocytoma and adrenocortical cancer should undergo prompt surgical intervention because untreated pheochromocytoma may result in significant cardiovascular complications
Patients with aldosterone-producing adenomas should be offered surgery to cure aldosterone excess
it is reasonable to consider that younger patients and those who have disorders potentially attributable to autonomous glucocorticoid secretion (eg, recent onset of hypertension, diabetes, obesity, and low bone mass) and have well-documented glucocorticoid secretory autonomy (ie, suppressed dehydroepiandrosterone sulfate [DHEAS], failure to suppress cortisol normally on 1 mg overnight dexamethasone test [DST], low serum corticotropin [ACTH] concentration, lack of suppression to high-dose overnight DST [8 AM serum cortisol >1.8 mcg/dL]) are candidates for adrenalectomy. If adrenalectomy is performed, perioperative glucocorticoid coverage should be administered because of the risk of adrenal insufficiency, hemodynamic crisis, and death. Patients should be sent home from the hospital on glucocorticoid replacement and monitored for recovery of the hypothalamic-pituitary-adrenal axis
Adrenal masses with either suspicious imaging phenotype or size larger than 4 cm should be considered for resection because a substantial fraction will be adrenocortical carcinomas [2,14]. The clinical scenario and patient age frequently guide the management decisions in patients who have adrenal incidentalomas that fall on either side of the 4 cm diameter cutoff. As an example, most clinicians would advise resecting a lipid-poor (29 HU) 3.2 cm adrenal incidentaloma in a 23-year-old woman; whereas, most clinicians would choose serial imaging follow-up in an 83-year-old woman with a lipid-rich (9 HU) 4.7 cm adrenal incidentaloma.
On computed imaging, the presence of large amounts of macroscopic fat in an adrenal mass is diagnostic of a myelolipoma (image 6) [58]. Although adrenal myelolipomas may grow over time, they can usually be followed without surgical excision. However, when larger than 6 cm in diameter or when causing local mass-effect symptoms, surgical removal should be considered
An adrenalectomy may be done laparoscopically, endoscopically via the posterior approach, or as an open procedure. Laparoscopic adrenalectomy, compared with open adrenalectomy, is associated with less pain, shorter hospitalization time, less blood loss, and faster recovery
Laparoscopic versus open posterior adrenalectomy: a case-control study of 100 patients. Thompson GB, Grant CS, van Heerden JA, Schlinkert RT, Young WF Jr, Farley DR, Ilstrup DM Surgery. 1997;122(6):1132.
In patients with known or suspected adrenal carcinoma, the laparoscopic approach should only be considered if the adrenal mass is <10 cm and does not appear to be locally invasive [62,63]. An open adrenalectomy is recommended for all large (>10 cm) adrenal masses, including those benign imaging features, as the adrenal mass may be diagnosed as malignant on a definitive histologic review
1. Extended subcostal incision. Can also be extended cephalad in the midline up to the xiphoid to allow better exposure for mobilization of the liver and other upper abdominal viscera, which is often necessary for very large (10 cm) or invasive tumors.
Exposure for this approach may be facilitated by elevating the right flank somewhat and by placing a roll under the right side. A midline incision is an option for the occasional patient who requires bilateral open adrenalectomy.
2. After entering the abdomen, the liver and peritoneal surfaces are inspected for the presence of metastatic disease. On the right side, the liver is fully mobilized by dividing the triangular ligament. With a large tumor it may be necessary to mobilize the hepatic flxexure of the colon and retract it inferiorly.
3. The duodenum is also mobilized using a Kocher maneuver (dissection of the lateral peritoneal attachments of the duodenum to allow inspection of the duodenum, pancreas, and other retroperitoneal structures over to the great vessels.) to expose the IVC (Fig. 9B).
4. On the left side, the splenic flexure of the colon is mobilized from its attachments and the splenorenal ligament is divided. The tail of
the pancreas and spleen are together reflected medially to expose the adrenal.
Inferior traction on the kidney exposes the adrenal gland. The dissection begins medially to develop the plane between the
tumor and the vena cava and to assess resectability. Periaortic lymph nodes should be assessed for involvement as well.
The right adrenal vein is ligated and the tumor is dissected away from the vena cava. A portion of the lateral wall of the vena cava may be taken along with the tumor if it appears involved.
Most of the arterial branches that enter the superior, medial, and inferior aspects of the adrenal are small and can be cauterized, but there are often two or three larger branches that should be tied. The right adrenal vein is usually identifiable early in the dissection and is typically
located at about the midportion of the adrenal; it enters the posterolateral aspect of the IVC. Th is vein should be carefully isolated with blunt dissection and transfixed. Excessive traction on the adrenal vein is to be avoided as it may tear along the vena cava with resultant brisk hemorrhage.
Once the vein has been ligated and divided, the
adrenal can be retracted away from the
vena cava and all remaining medial attachments
and small vessels can be divided. The dissection then continues along the inferomedial border of the adrenal and out laterally along the superior
pole of the kidney. The dissection should not extend too low into the area of the renal hilum because of the risk of injuring a superior polar renal artery. Finally, the relatively avascular posterior and lateral
attachments are divided.
.
For left sided adrenal masses
Initial peritoneal access is achieved 2cm inferior to the costal margin in the midclavicular line (Palmer’s point). The ports are
equally distributed along the costal margin, with the posterior port placed as far lateral-posterior as permitted by the position of
the colon (Fig. 39-24). At least 5cm between each port to minimize external interference of the laparoscopic instruments. For tissue dissection, we
employ the hook monopolar cautery and an energy-based tissue
sealing or dividing device.
The lateral attachments of the spleen are taken down first, with the goal of rotating the left upper quadrant viscera anteromedially. Care must be taken to avoid a capsular tear of the spleen, which may arise from undue tension on a congenital or acquired adhesive
band.
Splenic mobilization is continued until the greater curvature of the stomach becomes visible at its apex, at which point the spleen and tail of the pancreas are allowed to fall anteriorly with rightward tilting of the table and gentle use of the fan
retractor, if necessary.
It is critical to achieve the correct plane of dissection precisely during this part of the procedure because the
tail of the pancreas and splenic vessels are potentially vulnerable to injury.
In patients with large or inferiorly positioned tumors,
the splenic flexure of the colon must be mobilized caudally by
dividing the splenocolic ligament.
We use an open book technique,
which involves developing the cleft-like plane just medial to the adrenal gland and lateral to the aorta (Fig. 39-25).
The left-hand page of the book is composed of the spleen, tail of the
pancreas, and greater curvature of the stomach. The right-hand
page of the book is made up by the kidney and adrenal tumor.
The left crus of the diaphragm is a useful landmark that leads the
surgeon to the left inferior phrenic vein.
the left inferior phrenic vein courses along the medial aspect of the left
adrenal gland before joining with the left adrenal vein. By developing
the cleft of the open book, moving from superior to inferior,
the adrenal vein is encountered at the inferomedial aspect of the
adrenal gland. The small adrenal arteries that lie within this plane
can be handled with energy-based coagulation. The left adrenal
vein is carefully dissected out, aggressively coagulated or clipped,
and divided. The inferior tip of the left adrenal gland may extend
low, approaching the renal hilum within millimeters. However,
because the left adrenal vein is rather long (2 cm), it is generally
not necessary to expose the renal vasculature during left adrenalectomy.
Many patients have a superior pole renal artery branch
that approaches the inferior aspect of the left adrenal gland. Injury
to this structure must be carefully avoided by keeping dissection
close to the adrenal capsule while the specimen is elevated away
from the medial aspect of the superior pole of the left kidney.
The adrenal gland is liberated by completing dissection circumferentially
and posteriorly, taking the specimen off of the
superior pole of the kidney and posterior abdominal wall. These
attachments are deliberately divided last because they aid in suspending
the adrenal gland on the lateral-superior wall of the
operative field, providing exposure of the medial vascular plane
during the critical initial portion of the procedure. The tumor
is placed into a resilient catchment device, morcellated, and
extracted.
FIGURE 39-25 Technique of left laparoscopic adrenalectomy. The
spleen and pancreatic tail have been mobilized and retracted anteromedially
to expose the adrenal gland. The cleft of the open book is developed
in a superior to inferior direction to identify the inferior phrenic
vein and adrenal vein.
A conceptual contrast between left and right adrenalectomy is that left adrenalectomy centers on identification of the correct plane of dissection and right adrenalectomy centers on
the avoidance of venous bleeding. Of note, the junction of the inferior vena cava and right renal vein is frequently difficult to identify. In vivo, the transition is a gradual curve rather than the 90-degree takeoff depicted in anatomy texts.
The most common operative complication is hemorrhage, which can occur from the adrenal vein, small arteries to the adrenal, the adrenal gland or tumor, hepatic veins, renal vessels, and the IVC or adjacent solid organs (spleen, pancreas, kidney, liver). Bleeding has also been the most common reason for conversion from the laparoscopic approach to open adrenalectomy.
Minor bleeding during the procedurecan usually be managed with tamponade of the area and then direct control of the bleeding site with cautery or clips. Prompt conversion to an open procedure should be carried
out if the bleeding is from a major vessel that cannot be immediately controlled. In addition to hemorrhage, vascular occlusion can also occur by inadvertent ligation of a renal artery branch or other visceral vessels.
Other organs and structures in the vicinity of the dissection that may be injured (by cautery, clips, or retraction) include the colon, spleen, pancreas, liver, stomach, kidney, and ureter, and these should be inspected carefully prior to closure. If there is any concern that the pancreatic parenchyma has
been injured, a closed-suction drain should be placed. The diaphragm and pleura can also be injured with any of the various approaches, although this complication is less common with the laparoscopic approach.
The patient with a pheochromocytoma is at risk for intraoperative hypertensive crisis and arrhythmias if there has not been adequate preparation pharmacologically for surgery.
Patients with an adrenal tumor causing Cushing syndrome should receive glucocorticoids as a stress dose in the perioperative period, which can then tapered to an oral maintenance steroid dose until their hypothalamic–pituitary–adrenal axis has recovered, which may take up to 12 to 18 months.
Following resection of a pheochromocytoma, additional intravenous fluids may be required postoperatively due to intravascular
volume expansion from Doxazosin.
These patients may also become hypoglycemic postoperatively due to loss of inhibition of insulin secretion by high levels of circulating
catecholamines.
Plasma-fractionated metanephrines or 24-hour urinary catecholamine levels should be checked at follow-up and on
a yearly basis to evaluate for recurrence. Close follow-up is also required for patients with adrenocortical malignancy including periodic
measurement of hormone levels and imaging with CT or MRI. Local recurrences or solitary metastases may be treated with surgical resection
in select cases.
Patients undergoing laparoscopic adrenalectomy usually require minimal parenteral analgesia and are often on oral pain medication on the fi rst postoperative day, whereas patients undergoing an open procedure have a greater parenteral analgesia requirement often lasting more than 48
hours. Laparoscopic patients are started on a liquid diet early postoperatively and often can be discharged within 24 hours unless a longer period of observation is needed for blood pressure management or hormone replacement. Most patients can return to unrestricted activity within 7 to 14 days of operation.
In patients with an indeterminate adrenal mass (by imaging) opting not to undergo adrenalectomy following initial assessment, we suggest a repeat noncontrast CT or MRI after 6–12 months to exclude significant growth (⊕OOO). We suggest surgical resection if the lesion enlarges by more than 20% (in addition to at least a 5 mm increase in maximum diameter) during this period. If there is growth of the lesion below this threshold, additional imaging after 6–12 months should be performed.