1. Issue 237 | September 2015
To download previous Researcher issues on The SourceSM
, please visit www.criver.com/thesource.
The use of biologic therapies has steadily increased since the first monoclonal antibody therapies emerged, and their growing
importance has highlighted the need to understand the immunogeneic responses these might generate. This has been further
emphasized by the regulatory bodies following submission of generic applications for biologic therapies (biosimilars), and the use
of cell-based assays to detect the presence of neutralizing antibodies has thus become a regulatory expectation. The presence of
neutralizing anti-drug antibodies against biotherapeutics is associated with reduced pharmacodynamics and loss of bioactivity,
and can cause potentially serious side effects requiring the patient to be prescribed multiple therapies or eventually stop treatment.
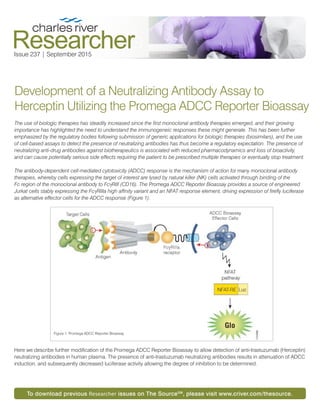
The antibody-dependent cell-mediated cytotoxicity (ADCC) response is the mechanism of action for many monoclonal antibody
therapies, whereby cells expressing the target of interest are lysed by natural killer (NK) cells activated through binding of the
Fc region of the monoclonal antibody to FcgRIII (CD16). The Promega ADCC Reporter Bioassay provides a source of engineered
Jurkat cells stably expressing the FcgRIIIa high affinity variant and an NFAT response element, driving expression of firefly luciferase
as alternative effector cells for the ADCC response (Figure 1).
Here we describe further modification of the Promega ADCC Reporter Bioassay to allow detection of anti-trastuzumab (Herceptin)
neutralizing antibodies in human plasma. The presence of anti-trastuzumab neutralizing antibodies results in attenuation of ADCC
induction, and subsequently decreased luciferase activity allowing the degree of inhibition to be determined.
Development of a Neutralizing Antibody Assay to
Herceptin Utilizing the Promega ADCC Reporter Bioassay
Figure 1: Promega ADCC Reporter Bioassay
2. Methods
To modify the Promega ADCC assay for use as a neutralizing
antibody (NAb) assay, Herceptin, anti-trastuzumab antibodies
and the relevant isotype controls were prepared at 2x the
required concentration. The Herceptin and anti-trastuzumab
antibodies (or corresponding isotypes) were mixed at a 1:1
ratio and incubated for 1 hour at 37 ºC before use in the
Promega ADCC Reporter Bioassay.
Results
To determine whether the anti-trastuzumab could inhibit the
ADCC response of Herceptin, antibody dilutions were prepared
in assay medium and mixed in a checkerboard layout. As all
concentrations of the anti-trastuzumab positive control (PC)
antibody inhibited the ADCC response at 1 ng/mL Herceptin,
and only the highest concentration of the PC inhibited ADCC
at 100 ng/mL Herceptin, 10 ng/mL was chosen as the optimal
concentration for development of the neutralizing antibody
assay (Table 1, Figure 2).
To determine the minimum plasma dilution, serial dilutions of
human pooled plasma were prepared in assay buffer (Figure 3).
Neat plasma induced an almost complete inhibition of the
ADCC response which reduced with each subsequent dilution.
As the inhibition of the ADCC response began to plateau
between a 1:32 and 1:64 dilution of plasma, a 1:50 dilution was
chosen as the minimum plasma dilution for preparation of the
anti-trastuzumab postive control.
Anti-trastuzumab or isotype control antibody dilutions were
spiked into a 1:50 dilution of pooled plasma and pre-incubated
with 10 ng/mL Herceptin or isotype control. The isotype control
induced no inhibition of the ADCC response. In comparison,
anti-trastuzumab induced a dose-dependent inhibition of the
ADCC response (Figure 4).
0
200000
400000
600000
800000
1000000
1200000
1400000
1600000
1800000
2000000
100 10 1 0
RelaƟveLuminescenceUnits(RLU)
HercepƟn ConcentraƟon (ng/mL)
AnƟ-Trastuzumab
1000 ng/mL
AnƟ-Trastuzumab
100 ng/mL
AnƟ-Trastuzumab
10 ng/mL
AnƟ-Trastuzumab
0 ng/mL
Isotype Control
1000 ng/mL
Isotype Control
100 ng/mL
Isotype Control
10 ng/mL
Isotype Control
0 ng/mL
0
200000
400000
600000
800000
1000000
1200000
1400000
1600000
12 10 8 6 4 2 0
RelaƟveLuminescenceUnits(RLU)
AnƟ-Trastuzumab (PC) ConcentraƟon (ng/mL)
HercepƟn +
PC
HercepƟn +
IgG1
IgG1 + PC
IgG1+ IgG1
0
200000
400000
600000
800000
1000000
1200000
1400000
Neat 1:2 1:4 1:8 1:16 1:32 1:64 1:128 0
RelaƟveLuminescenceUnit(RLU)
Plasma DiluƟon
Human
Pooled
Plasma
Figure 2: Herceptin Neutralizing Antibody Assay
Figure 4: Neutralizing Antibody Assay
Figure 3: Plasma Effects on ADCC Activity
Table 1: Herceptin Neutralizing Antibody Assay - Percent Inhibition (%)
Herceptin (ng/mL) 100 10 1 0
Anti-
Trastuzumab
(ng/mL)
1000 99 99 87 0
100 27 100 91 6
10 0 56 88 0
0 0 0 0 0
Isotype
Control
(ng/mL)
1000 0 0 0 0
100 0 0 0 0
10 1 0 0 0
0 0 0 0 0
3. Intra-assay precision was assessed by plating three individual
preparations of Herceptin and anti-trastuzumab antibodies
on the sample plate, with inter-assay precision assessed on
three separate occassions. A high level of intra-assay precision
was observed for both anti-trastuzumab and the isotype
control (Figure 5). A larger inter-assay variation was observed
for the isotype control than for anti-trastuzumab, likely due
to differences in the pooled plasma preparations (Figure 6).
However, a high level of inter-assay precision was observed for
anti-trastuzumab, and the variation observed for the isotype
control was within acceptable limits.
To assess the effect of cell passage on the neutralizing
antibody assay, the neutralizing antibody assay was tested on
SK-BR-3 cells at a low and a high passage. A similar pattern of
inhibition was observed at both cell passages, with only a slight
increase in the ADCC response oberved for the high passage
cells with both the anti-trastuzumab and isotype control
antibodies (Figure 7).
Conclusion
The results of this short-term study demonstrate that the
Promega ADCC Reporter Bioassay can be successfully utilized
to assess the presence of neutralizing antibodies to therapeutic
assays with an ADCC effector function.
0
100000
200000
300000
400000
500000
600000
700000
12 9 6 3 0
RelaƟveLuminescenceUnits(RLU)
AnƟ-Trastuzumab ConcentraƟon (ng/mL)
PC
IgG1
0
100000
200000
300000
400000
500000
600000
700000
800000
900000
12 9 6 3 0
RelaƟveLuminescenceUnits(RLU)
AnƟ-Trastuzumab (PC) ConcentraƟon (ng/mL)
High Passage PC
High Passage IgG1
LowPassage PC
LowPassage IgG1
0
100000
200000
300000
400000
500000
600000
700000
800000
900000
12 9 6 3 0
RelaƟveLuminescenceUnits
AnƟ-Trastuzumab (PC) ConcentraƟon (ng/mL)
PC
IgG1
Figure 5: Intra-Assay Precision
Figure 7: Cell Line Stability
Figure 6: Inter-Assay Precision
For additional information, please visit The SourceSM
, a secure portal that provides registered users with direct access to the
technical, scientific and educational resources available from Charles River. To register, visit www.criver.com/thesource.
askcharlesriver@crl.com
www.criver.com