Book Paid Powai Call Girls Mumbai 𖠋 9930245274 𖠋Low Budget Full Independent H...
Guyton, Michael; Gardasil Presentation
1. Improving Rates of Gardasil and Menactra Administration at The Center
for Pediatric Medicine
Mike Guyton, MD, Jill Golden, MD, Russ Kolarik, MD
Internal Medicine-Pediatric Residency Program
Improve Gardasil and Menactra administration
rates at The Center for Pediatric Medicine to a
goal initiation rate of 80%.
HPV:
~79 million currently infected
Nearly all sexually active men and women
get at least 1 type of HPV in their lifetime
Associated with significant cancer burden
Meningococcus:
800-1,200 cases of invasive disease occur
annually
21% in ages 14-24
In the US, almost all cases caused by
serogroups B, C, Y
Baseline Survey Results
The following patterns were found after gathering
responses to the survey
Only 32% of those polled (n=32) accurately
identified how many cancers were associated
with HPV
The majority felt that the morbidity and
mortality rate of meningococcal disease had
changed from the 1950’s
~70% of those polled were unaware that a
second booster vaccination of Menactra was
recommended for healthy adolescents
Participants were accurate in identifying the
rank of cervical cancer among other cancers,
and identifying contraindications to Gardasil
administration
Based on the survey, knowledge regarding
HPV was greater than regarding
Meningococcus
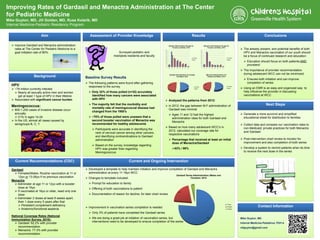
Analyzed the patterns from 2012:
In 2012, the gap between M:F administration of
Gardasil was minimal
Ages 11 and 12 had the highest
administration rates for both Gardasil and
Menactra
Based on how many adolescent WCC’s in
2012, calculated our coverage rate for
respective vaccinations
Percentage that received at least an initial
dose of Menactra/Gardasil
63% / 96%
Mike Guyton, MD
Internal Medicine-Pediatrics, PGY-4
mfguyton@gmail.com
The already present, and potential benefits of both
HPV and Menactra vaccination of our youth should
be a focus of continued research and education
Education should focus on both patients AND
providers!
The importance of provider recommendation
during adolescent WCC can not be minimized
Ensures both initiation and can improve
completion of series
Using an EMR is an easy and organized way to
help influence the provider in discussing
vaccinations at WCC
Generate a more succinct and simplified
educational sheet for distribution to families
Collect data and compare our vaccination rates to
non-Medicaid, private practices for both Menactra
and Gardasil
Post-intervention chart review to monitor for
improvement and also completion of both series
Develop a system to remind patients when its time
to receive the next dose in the series
Gardasil
Females/Males: Routine vaccination at 11 or
12yo or 13-26yo if no previous vaccination
Menactra
Administer at age 11 or 12yo with a booster
dose at 16yo
If vaccinated at 16yo or older, need only one
dose
Administer 2 doses at least 8 weeks apart,
then 1 dose every 5 years after that
Persistent complement deficiency
Anatomic/functional asplenia
National Coverage Rates (National
Immunization Survey, 2010):
Gardasil: 62.2% with provider
recommendation
Menactra: 77.3% with provider
recommendation
0
10
20
30
40
50
60
70
80
90
100
11 12 13 14 15 16 17 18
Gardasil Administration By Age for
Females and Males; 2012
Females
Males
0
10
20
30
40
50
60
70
80
90
11 12 13 14 15 16 17 18
Menactra Administration By Age for
Females and Males; 2012
Females
Males
254
246
Gardasil Administration for Females
and Males; 2012
Females
Males
172
156
Menactra Administration For
Females and Makes; 2012
Females
Males
Developed a template to help maintain initiation and improve completion of Gardasil and Menactra
administration at every 11-18yo WCC
Changes to template included:
Prompt for education to family
Offering of both vaccinations to patient
Documentation of reason for decline, for later chart review
Improvement in vaccination series completion is needed
Only 3% of patients have completed the Gardasil series
We are doing a great job at initiation of vaccination series, but
interventions need to be developed to ensure completion of the series
76%
21%
3%
Gardasil Series Administration (Males and
Females); 2012
1 Dose
2 Doses
3 Doses
ResultsAssessment of Provider Knowledge
Surveyed pediatric and
med/peds residents and faculty
Aim
Background
Current Recommendations (CDC) Current and Ongoing Intervention
Conclusions
Next Steps
Contact Information
2. Improving Rates of Gardasil and Menactra Administration at The Center
for Pediatric Medicine
Mike Guyton, MD, Jill Golden, MD, Russ Kolarik, MD
Internal Medicine-Pediatric Residency Program
Improve Gardasil and Menactra administration
rates at The Center for Pediatric Medicine to a
goal initiation rate of 80%.
HPV:
~79 million currently infected
Nearly all sexually active men and women
get at least 1 type of HPV in their lifetime
Associated with significant cancer burden
Meningococcus:
800-1,200 cases of invasive disease occur
annually
21% in ages 14-24
In the US, almost all cases caused by
serogroups B, C, Y
Baseline Survey Results
The following patterns were found after gathering
responses to the survey
Only 32% of those polled (n=32) accurately
identified how many cancers were associated
with HPV
The majority felt that the morbidity and
mortality rate of meningococcal disease had
changed from the 1950’s
~70% of those polled were unaware that a
second booster vaccination of Menactra was
recommended for healthy adolescents
Participants were accurate in identifying the
rank of cervical cancer among other cancers,
and identifying contraindications to Gardasil
administration
Based on the survey, knowledge regarding
HPV was greater than regarding
Meningococcus
Analyzed the patterns from 2012:
In 2012, the gap between M:F administration of
Gardasil was minimal
Ages 11 and 12 had the highest
administration rates for both Gardasil and
Menactra
Based on how many adolescent WCC’s in
2012, calculated our coverage rate for
respective vaccinations
Percentage that received at least an initial
dose of Menactra/Gardasil
63% / 96%
Mike Guyton, MD
Internal Medicine-Pediatrics, PGY-4
mfguyton@gmail.com
The already present, and potential benefits of both
HPV and Menactra vaccination of our youth should
be a focus of continued research and education
Education should focus on both patients AND
providers!
The importance of provider recommendation
during adolescent WCC can not be minimized
Ensures both initiation and can improve
completion of series
Using an EMR is an easy and organized way to
help influence the provider in discussing
vaccinations at WCC
Generate a more succinct and simplified
educational sheet for distribution to families
Collect data and compare our vaccination rates to
non-Medicaid, private practices for both Menactra
and Gardasil
Post-intervention chart review to monitor for
improvement and also completion of both series
Develop a system to remind patients when its time
to receive the next dose in the series
Gardasil
Females/Males: Routine vaccination at 11 or
12yo or 13-26yo if no previous vaccination
Menactra
Administer at age 11 or 12yo with a booster
dose at 16yo
If vaccinated at 16yo or older, need only one
dose
Administer 2 doses at least 8 weeks apart,
then 1 dose every 5 years after that
Persistent complement deficiency
Anatomic/functional asplenia
National Coverage Rates (National
Immunization Survey, 2010):
Gardasil: 62.2% with provider
recommendation
Menactra: 77.3% with provider
recommendation
0
10
20
30
40
50
60
70
80
90
100
11 12 13 14 15 16 17 18
Gardasil Administration By Age for
Females and Males; 2012
Females
Males
0
10
20
30
40
50
60
70
80
90
11 12 13 14 15 16 17 18
Menactra Administration By Age for
Females and Males; 2012
Females
Males
254
246
Gardasil Administration for Females
and Males; 2012
Females
Males
172
156
Menactra Administration For
Females and Makes; 2012
Females
Males
Developed a template to help maintain initiation and improve completion of Gardasil and Menactra
administration at every 11-18yo WCC
Changes to template included:
Prompt for education to family
Offering of both vaccinations to patient
Documentation of reason for decline, for later chart review
Improvement in vaccination series completion is needed
Only 3% of patients have completed the Gardasil series
We are doing a great job at initiation of vaccination series, but
interventions need to be developed to ensure completion of the series
76%
21%
3%
Gardasil Series Administration (Males and
Females); 2012
1 Dose
2 Doses
3 Doses
ResultsAssessment of Provider Knowledge
Surveyed pediatric and
med/peds residents and faculty
Aim
Background
Current Recommendations (CDC) Current and Ongoing Intervention
Conclusions
Next Steps
Contact Information