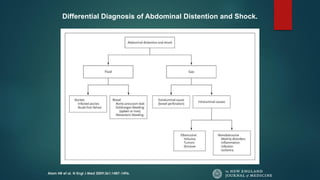
A 22-year-old male was admitted to the emergency room in a comatose state due to shock after being transferred from another hospital where he was being treated with high doses of antipsychotic medications for an acute psychotic episode from drug abuse. Imaging showed severe dilation of the intestines without obstruction or free air. The patient underwent surgery where necrosis of the right colon was found. The diagnosis was acute megacolon (Ogilvie's syndrome) likely caused by the antipsychotic medications, which is a known but rare risk. Literature review showed antipsychotics like clozapine can cause gastrointestinal hypomotility and this case highlights the need to monitor for constipation from these drugs.