
Recommended
More Related Content
What's hot
What's hot (15)
Similar to Student Diagnosis Treatment Plan
Similar to Student Diagnosis Treatment Plan (20)
Student Diagnosis Treatment Plan
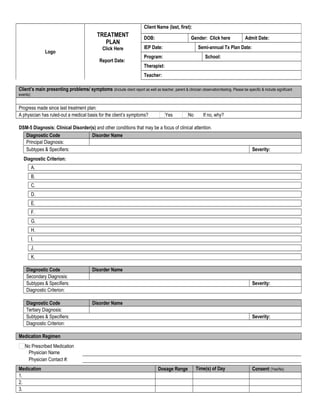
- 1. Client’s main presenting problems/ symptoms (Include client report as well as teacher, parent & clinician observation/testing. Please be specific & include significant events): Progress made since last treatment plan: A physician has ruled-out a medical basis for the client’s symptoms? Yes No If no, why? DSM-5 Diagnosis: Clinical Disorder(s) and other conditions that may be a focus of clinical attention. Diagnostic Code Disorder Name Principal Diagnosis: Subtypes & Specifiers: Severity: Diagnostic Criterion: A. B. C. D. E. F. G. H. I. J. K. Diagnostic Code Disorder Name Secondary Diagnosis: Subtypes & Specifiers: Severity: Diagnostic Criterion: Diagnostic Code Disorder Name Tertiary Diagnosis: Subtypes & Specifiers: Severity: Diagnostic Criterion: Medication Regimen No Prescribed Medication Physician Name Physician Contact #: Medication Dosage Range Time(s) of Day Consent (Yes/No) 1. 2. 3. Logo TREATMENT PLAN Click Here Report Date: Client Name (last, first): DOB: Gender: Click here Admit Date: IEP Date: Semi-annual Tx Plan Date: Program: School: Therapist: Teacher:
- 2. 4. 5. Service Discipline Frequency Individual Therapy Licensed MHP (PhD., PsyD, LCSW, MFT) Qualified MHP (ACSW, MFT Intern, Professional Counselor Intern) Group Therapy LMHP QMHP Family Therapy LMHP QMHP Milieu Services LMHP QMHP Behavior Coach As needed Collateral Services LMHP QMHP Behavior Coach As needed Crisis Intervention LMHP QMHP Behavior Coach As needed Other, specify: Discharge Planning Therapist’s Name: Signature: Date: Supervisor’s Name: Signature: Date:
- 3. Student’s main presenting problems/ symptoms (Include student report as well as teacher, parent & therapist observation/testing. Please be specific & include significant events): Progress made since last treatment plan: Student & Family Strengths (What will be used to help the student achieve their treatment plan goals & measurable objectives? Include student report as well as teacher, parent & therapist observation. Please be specific.) Diversity Issues & Considerations Long Term Goals Short Term Goals Measurable Objectives Social/Emotional Objective #1: …XX% of the time. By: ??/??/???? Current Functioning: % of the time. As of: ??/??/???? Progress made since last treatment plan: Therapist Interventions: 1. 2. 3. Mental Health Coach Interventions: 1. 2. 3. Teacher Interventions: 1. 2. 3. Student Interventions: 1. 2. 3. Social/Emotional Objective #2: …XX% of the time. By: ??/??/???? Current Functioning: % of the time As of: ??/??/???? Progress made since last treatment plan: Therapist Interventions: 4. 5. 6. Mental Health Coach Interventions: 4. 5. 6. Teacher Interventions: 4. 5. 6. Student 4.
- 4. Interventions: 5. 6. Social/Emotional Objective #3: …XX% of the time. By: ??/??/???? Current Functioning: % of the time As of: ??/??/???? Progress made since last treatment plan: Therapist Interventions: 7. 8. 9. Mental Health Coach Interventions: 7. 8. 9. Teacher Interventions: 7. 8. 9. Student Interventions: 7. 8. 9. Old Objectives (What objectives have you worked on with the student in the past and what were the results?) Family Goals Progress made since last treatment plan: Is the parent/guardian involved in the treatment of the student? Yes No If not, why? Was the parent/guardian involved in the creation of the treatment plan? Yes No Does the parent/guardian agree with the treatment plan? Yes No Parent/Guardian requested and received a copy of the Treatment Plan Therapist explained benefits, alternatives, and risks or consequences of treatment. SIGNATURES: Student Name (Print): Signature: Date: Parent/Guardian (Print): Signature: Date: Therapist (Print): Signature: Date: Supervisor (Print): Signature: Date: