1. Association between parental education level, perception of child’s weight, and acceptance of obesity counseling:
opportunities for pharmacists
Chris Anson, PharmD/MSCR Candidate1; Dan Waller, PharmD/MSCR Candidate1; Melissa Johnson, PharmD, MHS, AAHIVE 1,2; Tina Tseng, PhD, MSPH1; Ray Tseng, DDS, PhD1,3,4
1Campbell University School of Pharmacy, Buies Creek, NC; 2Division of Infectious Diseases, Duke University Medical Center, Durham, NC; 3Dept. Of Nutrition, Gillings School of Global Public Health, 4Dept. of Pediatric Dentistry, School of Dentistry, University of North Carolina at Chapel Hill, Chapel Hill, NC.
ABSTRACT
OBJECTIVES
Authors of this presentation have the following to disclose concerning possible financial or personal relationships with
commercial entities that may have a direct or indirect interest in the subject matter of this presentation:
Christopher Anson: nothing to disclose
Daniel Waller: nothing to disclose
Melissa Johnson: nothing to disclose
Ray Tseng: nothing to disclose
Tina Tseng: nothing to disclose
Purpose: Childhood obesity is a problem in the U.S. and has become the most
widespread nutritional condition affecting children today. There may be a link
between the parent’s completed level of education, having an obese child, and
perception of child’s weight. Traditionally, obesity counseling has been the purview
of pediatricians or family physicians. Counseling parents on the dangers of
childhood obesity is an opportunity that non-physician healthcare professionals,
such as pharmacists, may engage in to aid in preventing development of obesity.
The purpose of this study is to characterize the association between a parental level
of education and accuracy of perception of child’s weight, and parental acceptance
of dietary counseling from a non-physician provider.
Methods: An IRB-approved 38-item survey was deployed in a department of public
health that evaluated parental education level, perception of child’s weight status,
and willingness to accept obesity counseling. Child’s weight and height were
measured, and body mass index percentile for age and sex was calculated at time
of survey deployment. The primary outcome variable is parental acceptance of
obesity counseling from a non-physician healthcare professional. Bivariate
analyses will be used to determine if parental education level or perception of child’s
weight were associated with acceptance of counseling from a non-physician
healthcare professional. If both education level and perception of child’s weight are
found to be statistically significantly associated with acceptance of counseling then
multivariate analysis will be performed to model the data.
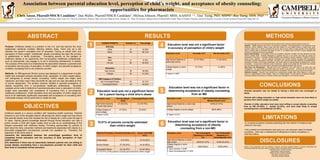
75.51% of parents correctly estimated
their child’s weight
•Parental education was not related to having a child who was overweight or
obese.
•Parents with college education vs. high school education were not more likely to
perceive their child’s weight accurately.
•Parents of either education level were most willing to accept obesity counseling
from an MD (91-96%), a dentist (41-52%), and were least likely to accept
counseling from a schoolteacher (33-36%).
CONCLUSIONS
LIMITATIONS
DISCLOSURES
1
2
RESULTS METHODS
Childhood obesity is a serious condition with hazardous health outcomes. Parental
influence is one of the strongest factors influencing the child’s weight and has shown
that parental obesity more than doubles the risk of obesity for a child under the age of
10 years. Having general knowledge learned through formal education can help a
parent provide a child with higher quality food as well as an understanding of the
dangers associated with childhood obesity. Providing opportunities for parents to
learn about the risks, prevention methods and treatments associated with obesity is a
favourable engagement non-physician provider can capitalize on. Therefore, the
objectives of this study were to:
1)examine the association between the parent/legal guardians’ level of
completed formal education and the accuracy of their perception of their
child’s weight.
2)To determine if there was an association between parents who are willing to
accept obesity counselling from a non-physician provider for their child and
their level of completed formal education.
•A convenience sample of parents presenting with their children for treatment was
utilized for this study.
•Only a dentist and schoolteacher were given as a non-physician option for obesity
counseling - there was no assessment of willingness to receive counseling in a
pharmacy setting.
3
4 Education level was not a significant factor
in accuracy of perception of child’s weight
Education level was not a significant factor in
determining acceptance of obesity counseling
from an MD
Education Level Accurate n(%) Not Accurate n(%)
High School Diploma or
some high school
37 (77.08%) 11 (22.92%)
College Degree or some
college
37 (74%) 13 (26%)
P Value= 0.7227
Education Level Felt Comfortable Speaking to a
Medical Doctor n(%)
High School Diploma or some high
school
44/48 (91.67%)
College Degree or some college 48/50 (96%)
P Value= 0.3711
CHARACTERISTIC Number (n) Percentage
Ethnicity
White 43 43.88%
Black 55 56.12%
Sex
Male 9 9.18%
Female 89 90.82%
Education
High School 48 48.98%
College 50 51.02%
BMI Category of Children
Not Overweight/Obese 54 55.10%
Overweight/Obese 44 44.90%
Parent’s Perception Parental Estimate n(%) Actual Child BMI
n(%)
Underweight 9 (9.18%) 10 (10.20%)
Normal Weight 67 (68.34%) 44 (44.90%)
Overweight/Obese 22 (22.45%) 44 (44.90%)
74 (75.51%) of the parents correctly perceived their child's weight
5Education level was not a significant factor
for a parent having a child who’s obese
Education Level Normal Weight
Child
Overweight/Obese Child
High School Diploma
or some high school
27 (56.25%) 21 (43.75%)
College Degree or
some college
27 (54%) 23 (46%)
P Value= 0.823
6
Education Level Felt Comfortable
Speaking to a Dentist
(%)
Felt Comfortable
Speaking to a
Schoolteacher n(%)
High School Diploma or some
high school 20/48 (41.67%) 16/48 (33.33%)
College Degree or some
college 26/50 (52%) 18/50 (36%)
P Value Dentist= 0.3055
P Value Schoolteacher= 0.1209
Education level was not a significant factor in
determining acceptance of obesity
counseling from a non-MD
This study was approved by the Biomedical Review Board at the University of North Carolina Chapel Hill.
Subjects. Eligible subjects came from a convenience population of parents/guardians who presented at the
Alamance County Children’s Dental Center with their children for new patient exams or dental recall visits.
Inclusion criteria were 1) Adults completing the survey had to be the parent or legal guardian of the presenting
child, 2) children had to be between the ages of 2 and 17, 3) children had to be free of chronic diseases and
conditions, including food and/or drug allergies.
Survey Administration. A 38 question survey was available in Spanish or English, and was deployed from May
2009 to October 2009. Parental willingness to complete and turn in the survey was taken as consent for
participation in the study. A medically certified translator was available to answer questions in English or Spanish
during survey collection. Surveys obtained information from several domains including child demographic
information, parental demographic information, education level, general knowledge regarding overweight/obesity,
perceptions of his/her child’s weight classification, and his/her opinion of utilizing dietary counseling from a variety
of providers. Surveys were numbered in order of collection. Height (in) and weight (lb) information was collected
from the child’s medical record and used for calculation of the BMI percentile for age and sex.
Data Entry and Management. Microsoft Excel 2007 (Redmond, WA) was used for all data entry and
management. All survey data was double-coded and verified to be accurate. Surveys that did not have full
responses to all variables of interest were excluded from the analysis. Only one survey per parent was utilized.
Statistical Analysis. Education was recoded into a dichotomous variable (high school diploma or some high
school vs. college degree or some college). Stata 10.0 (College Station, TX) was used for all statistical analyses.
Descriptive statistics and pearson Chi Square analysis were calculated for all univariate analyses.