
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Impact of Blood Removal on ADC in ICH Patients
Similar to Impact of Blood Removal on ADC in ICH Patients (20)
Impact of Blood Removal on ADC in ICH Patients
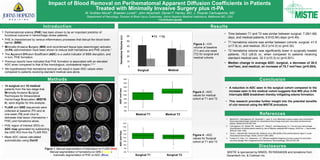
- 1. Impact of Blood Removal on Perihematomal Apparent Diffusion Coefficients in Patients Treated with Minimally Invasive Surgery plus rt-PA W. Andrew Mould*; Braeden Lovett*; John Muschelli; Daniel F. Hanley, MD; J. Ricardo Carhuapoma, MD Department of Neurology, Division of Brain Injury Outcomes, Johns Hopkins Medical Institutions, Baltimore MD, USA * Contributed equally Introduction Disclosures Methods Results Conclusion • Perihematomal edema (PHE) has been shown to be an important predictor of functional outcome in hemorrhagic stroke patients. • PHE is characterized by various inflammatory processes that disrupt the blood-brain barrier (BBB). • Minimally Invasive Surgery (MIS) and recombinant tissue-type plasminogen activator (rt-PA) administration have been shown to reduce both hematoma and PHE volume.1 • The Apparent Diffusion Coefficient (ADC) is a useful indicator of BBB disruption, and in turn, PHE formation. • Previous reports have indicated that PHE formation is associated with an elevated ADC when compared to that of the homologous, contralateral region.2,3,4 • We hypothesized that hematoma removal will result in lower ADC values when compared to patients receiving standard medical care alone. • Time between T1 and T2 was similar between surgical, 7.28(1.68) days, and medical patients, 6.91(0.84) days (p=0.49) . • T1 hematoma volume was similar between cohorts: surgical, 41.9 (±17.9) cc, and medical, 35.2 (±14.3) cc (p=0.32). • T2 hematoma volume was significantly lower in surgically treated patients, 15.2 (±8.9) cc, when compared to patients receiving standard medical care, 32.3 (±10.3) cc (p<0.001). • Median change in average ADC: surgical, a decrease of 30.5 mm2/sec, and medical, an increase of 75.7 mm2/sec (p=0.004). • A reduction in ADC seen in the surgical cohort compared to the increase seen in the medical cohort suggests that MIS plus rt-PA interrupts BBB breakdown thereby mitigating edema formation. • This research provides further insight into the potential benefits of clot removal using the MISTIE procedure. Figure 1. Manual segmentation of total lesion on FLAIR (Red) Manual segmentation of hematoma on GRE (Yellow) Automatic segmentation of PHE on ADC (Blue) • 14 surgical and 10 medical patients from the two-stage-trial, Minimally Invasive Surgical Techniques for Intracerebral Hemorrhage Evacuation (MISTIE II), were eligible for this analysis. • FLAIR and GRE sequences were collected at baseline (T1) and at one-week (T2) post ictus to delineate total lesion (hematoma + PHE) and hematoma alone. • PHE region of interest (ROI) on ADC map generated by subtracting the GRE ROI from the FLAIR ROI. • Mean ADC values calculated automatically using OsiriX MISTIE is sponsored by NINDS, R01NS046309 and donations from Genentech Inc. & Codman Inc. Figure 2 : ICH volume at baseline (T1) and one week (T2) for surgical and medical cohorts. Figure 3 : ADC values for medical cohort at T1 and T2 Figure 4 : ADC values for Surgical cohort at T1 and T2 References 0 10 20 30 40 50 60 Surgical Medical HematomaVolume(cc) T1 T2 1. Mould W.A., Carhuapoma J.R.; Muschelli J.; Lane, K. et al. Minimally invasive surgery plus recombinant tissue-type plasminogen activator for intracerebral hemorrhage evacuation decreases perihematomal edema. Stroke 2013;44:627-634. 2. Carhuapoma J.R., Barker P.B., Hanley D.F., Wang P., and Beauchamp, N.J. Human brain hemorrhage: Quantification of perihematoma edema by use of diffusion-weighted MR imaging. ANJR Am. J. Neuroradiol. 2002;23:1322–1326. 3. Olivot J., Mlynash MD, Kleinman BA, Straka M. et al. MRI profile of the perihematomal region in acute intracerebral hemorrhage. Stroke, 2010;41;2681-2683. 4. Forbes K.P.; Pipe, J.G.; Heiserman, J.E. Diffusion-weighted imagiving provides support for secondary neuronal damage from intraparenchymal hematoma. Neuroradiology, 2003;45:363-367. Surgical Medical 600 700 800 900 1000 1100 1200 1300 1400 Medical(T1( Medical(T2( ADC((mm2/sec)( 600 700 800 900 1000 1100 1200 1300 1400 Surgical)T1) Surgical)T2) ADC)(mm2/sec))ADCmm2/secADCmm2/sec Medical T1 Medical T2 Surgical T2Surgical T1